Multiple Myeloma: How Your Race and Age Can Affect Diagnoses and Treatment
Valarie Traynham
Multiple myeloma is the most common blood cancer among Black patients in the U.S., but many of those patients have an entirely different experience.
Studies show that Black patients respond better to newer treatments but are still twice as likely to die from the disease.
Patient advocate Valarie Traynham speaks with Shakira Grant, MBBS, of the UNC Medical Center. They discuss the barriers many Black patients face, how it impacts their care, and what can be done to help improve their outcomes.
Newly diagnosed patients [need] someone [who] they can ask questions [and] find out information and where to go for good relevant resources.
Valarie Traynham
Introduction
Valarie Traynham: I was diagnosed with multiple myeloma in 2015. Being a patient advocate, I want to be able to guide others through the process. When I was diagnosed, I did not have someone to go to and I think that’s very important. Newly diagnosed patients [need] someone [who] they can ask questions [and] find out information and where to go for good relevant resources.
I’m just so excited at the work that Dr. Grant is doing because it’s much needed. It’s an area that needs focus and she’s doing a wonderful job [of] getting that focus out there.
She focuses on a population of patients in the myeloma world that oftentimes [is] overlooked. It’s very important for that population of patients to be looked at and cared for and really understand what they are going through.
Dr. Grant is from the University of North Carolina and she focuses on geriatric multiple myeloma, health, and research.
Unfortunately, because multiple myeloma is also a disease that impacts older adults, we see this compounding effect, especially for Black older adults with multiple myeloma.
Dr. Shakira Grant
Dr. Shakira Grant: I’m primarily here to talk a little bit about our research and how this fits into sharing stories of patients and caregivers, which our team is really passionate about.
What really drew me to this type of work was this love for trying to bridge this gap in terms of the disparities that we see existing within not only outcomes but also survival for Black and white patients with multiple myeloma.
Unfortunately, because multiple myeloma is also a disease that impacts older adults, we see this compounding effect, especially for older Black adults with multiple myeloma. It’s really important for us as a research team to address some of these healthcare access barriers, which largely drive the disparate outcomes that we see in multiple myeloma.
We presented two studies. For the first one, we wanted to understand what barriers patients and their caregivers encounter when trying to seek care for multiple myeloma.
The top takeaway from that study is that many of our patients report that there’s really a delay in getting the diagnosis of myeloma and this results in them going to multiple specialists with their symptoms. Often, patients reported being dismissed by their doctors and being chalked up to just getting older and then repeating labs again in three months.
From this particular study, while we identified other barriers, including financial barriers, we do recognize that there is a need to focus on how we make the diagnosis, ensuring that patients are getting the diagnosis on time, which would allow them to enter into a care pathway where they can begin their treatment and minimize any chances that they will have any poor or adverse effects from multiple myeloma.
In terms of the other study, we wanted to look at factors that influence the participation in clinical trials for Black patients in particular. We did this by looking at the perspectives of patients with multiple myeloma as well as their hematologists.
One of our main takeaways from this is that the patient and their relationship with their doctor is really critical when trying to decide if a patient is going to be offered the opportunity to participate in a trial. Based on these findings, we do recognize that there is a need for more targeted interventions that address several steps in terms of communication between patients and their doctors to ensure that we have the best chances of offering clinical trials to a diverse patient population.
Many of our patients report that there’s really a delay in getting the diagnosis of myeloma and this results in them going to multiple specialists with their symptoms.
Dr. Grant
How do we get more diversity in clinical trials?
Valarie: I heard a lot about clinical trials. How can we get more minorities involved? What is that like for the older population that you see in the clinic?
Dr. Grant: Overall, when we think about increasing representation in clinical trials, we are coming up against two compounding factors. One is the older adult and then it’s the older adult who also identifies as having Black race.
For me, in clinical practice, one of the things that we try to do is to not only look at [the] patient’s chronologic age, but we also look at the functional age of patients. How well are they able to do their activity and to get around day to day? I believe that [is] probably better to assess eligibility for these particular patients for clinical trials in terms of Black representation or increasing representation of minoritized populations.
It is important for us to realize that myeloma does tend to affect an older adult population. We cannot really distill out and think about age and race separately, but we really should be thinking about these two things together. Our efforts to increase representation should be geared towards the older adult population, as well as thinking about the racial, ethnic, and minoritized populations.
We cannot really distill out and think about age and race separately, but we really should be thinking about these two things together.
Dr. Grant
How would you advise older multiple myeloma patients to stay positive?
Valarie: For a newly diagnosed older patient, how would you advise them? [There’s] so much going on. They’re getting the diagnosis. They’re trying to make it to the clinic. How would you advise them to stay positive and look for the good in the situation that they’re facing?
Dr. Grant: The thing that is really important that I’ve seen come out not only [from] our research but in my own clinical practice is the need to have a social support system. In our study, we looked at informal caregivers who were oftentimes spouses and, in some cases, adult children.
I really do think that having that support when you’re first diagnosed is really critical because you have, in essence, [a] second set of ears, [a] second set of eyes to help you with the amount of information that you’re getting, scheduling, [and monitoring] any potential treatment-related side effects.
I think [it’s] really important for patients to also seek knowledge about multiple myeloma from credible resources. Read as much as possible what you can about this disease, about things that you can expect, and then come to your provider’s visit prepared with those questions ready.
Having that support when you’re first diagnosed is really critical because you have, in essence, [a] second set of ears, [a] second set of eyes to help you.
Dr. Grant
Ask [about] things like clinical trial participation, if your doctor hasn’t mentioned it. It’s really important for patients to take that first bold step and say, “I’ve read about clinical trials. Do you think this could be a potential option for me?”
This really moves into this idea that we want our patients to not only have a really great social support system but also to be empowered to be able to ask the questions that they need of their physicians without feeling fearful or intimidated.
Valarie: I’m so glad you said that because that is one thing that I always try to tell newly diagnosed patients as a patient advocate. Find reputable material. Find out everything that you can about the disease. Don’t be afraid of it. It’s something that you’re going to be living with indefinitely.
We want our patients to not only have a really great social support system but also to be empowered to be able to ask the questions that they need of their physicians without feeling fearful or intimidated.
Dr. Grant
How do you build medical trust in Black communities?
Valarie: We know that trust in the African-American community is a big deal and that’s what we are focusing [on], too: raise trust and build trust in the community. As a physician, what are some of the things that patients are mainly dealing with?
I was listening to something and they talked about words matter — how you talk to patients, understanding patients, words that you use, words that the patient uses, and understanding and gathering information. Tell me [about] your thoughts on that.
Dr. Grant: What we’ve seen in our studies time and time again is that there is this legacy of medical mistrust that has been brought on by past research events where Black patients were intentionally harmed by the research enterprise and so it takes quite a while to be able to reverse those effects.
Things that we’ve learned from talking to patients [and] caregivers that can help close that trust gap is really working on our communication style as physicians, making sure that we’re using empathic communication, [and] letting our patients see that beyond the doctor title, we also are real people with real lives and lived experiences.
Don’t be afraid to pull back that curtain sometimes and let patients see that that relationship between patients and providers really helps to build up trust.
Find reputable material. Find out everything that you can about the disease. Don’t be afraid of it. It’s something that you’re going to be living with indefinitely.
Valarie
I think of a particular quote from one of our studies where a patient said that it’s all about [the] relationship and if we need to build trust, we really need to be focused on the relationship. That particular participant went on to say that really they believe that the physicians could benefit from relationship-building training.
That really stuck with me because I recognized that trust is so difficult to address. These are some strategies that, as a physician, we can do to at least start to build that and close that potential gap.
When it comes time to think about the research, there are different strategies that our team [uses] to really help foster trust and to help engage Black participants in our study. Some of those strategies have been described in the literature, but really it’s about having a team that is representative of the population that we’re trying to engage and helping them realize the value of this research and why we need to do this, especially for the Black community.
Trust is so difficult to address. These are some strategies that, as a physician, we can do to at least start to build that and close that potential gap.
Dr. Grant
We need to recognize that access to healthcare is dependent on several steps. This includes the patient’s ability to perceive their need for healthcare. Then they need to be able to seek out those services, reach the services, pay for the services, and engage with their healthcare provider.
I would encourage patients: if you are experiencing symptoms you’re concerned about and you’re seeing your provider and you don’t think your provider is necessarily answering or addressing those questions, don’t be afraid to talk to somebody else. Talk to another provider and do some additional research and see if there is potentially another option for you to have your symptoms examined.
They have to think about [the] costs of medications but also when they’re coming to the cancer center, the cost of parking, the cost of gas… all these things are really additive for patients, especially when they’re on a fixed income. This idea about having to pay twice was centered around the need to pay for all of these other healthcare services while also attending to the high cost associated with paying for parking at the health center.
In terms of other economic impacts, things like parking, don’t be afraid to tell your provider, “This is challenging for me to pay for parking,” or, “I’m having challenges just paying for my medications.” Because honestly, sometimes the visit time is so short that we don’t always have the time to ask if you are having financial concerns. We don’t want that. These financial challenges are a limitation to you getting your care on time.
Don’t be afraid to talk to your providers if you have concerns. Make those concerns known… If you’re having financial challenges, continue to share those concerns and ask about available resources.
Dr. Grant
Barriers patients face that prevent their care
Valarie: How often do you have patients that [face financial limitations?]
Dr. Grant: We actually see this, in my practice especially, quite often. It’s not uncommon at all for patients to be concerned about the cost of parking. Patients would express concerns about their ability to pay for parking. Sometimes it’s a bit of a challenge knowing what to do in those scenarios.
There are some efforts now at our cancer center to try to provide more accessible parking in terms of financial costs and reducing the cost of that, but it’s not always widely available to patients.
Don’t be afraid to talk to your providers if you have concerns. Make those concerns known. That goes from even when you’re first presenting, before you’re diagnosed and you’re concerned about it, keep sharing those concerns with your provider.
If you’re having financial challenges, continue to share those concerns and ask about available resources. There are more resources out there than sometimes patients may actually think or may actually have knowledge about.
Conclusion
Valarie: Thank you for joining us today and going over all of this. It’s so important what you do in the field of myeloma.
What we’re dealing with is meaningful. It’s life-impacting so it’s very important that you understand if you’re not being treated right or you feel that something is not right, say something because it’s not okay.
You have the right as a patient to have something done about that. You are in control of your health. Don’t settle. Without you, it would just be a missing piece.
Dr. Grant: Thank you for having me.
If you’re not being treated right or you feel that something is not right, say something because it’s not okay. You have the right as a patient to have something done about that. You are in control of your health. Don’t settle.
Valarie
Special thanks again to AbbVie for its support of our independent patient education content. The Patient Story retains full editorial control.
Chronic lymphocytic leukemia patient advocate Andrew Schorr has been living with CLL for 26 years.
In this conversation, he talks with hematologist-oncologist Dr. Nitin Jain from the MD Anderson Cancer Center who specializes in patients with CLL and ALL.
BTK inhibitors: choosing the right drug for the right patient
Andrew Schorr: With us is one of my favorite CLL researchers and experts, Dr. Nitin Jain, from MD Anderson.
Patients like me have lots of questions. We hope we can live a long, full life with CLL. You have more options than ever before.
One of the areas is BTK, Bruton tyrosine kinase inhibitors. We have Imbruvica, acalabrutinib or Calquence, [and] zanubrutinib that may be approved in CLL before long but is used in some other conditions. These drugs have made a big difference for people. What [do] we know about them now and how [do] you choose which one is right for which patient?
Dr. Jain: BTK inhibitors are oral drugs. They target a specific protein called BTK on the CLL cells.
The first one was ibrutinib. The second-generation ones are acalabrutinib and zanubrutinib. Zanubrutinib is not yet approved for CLL, but we are expecting it to be approved pretty soon, maybe in the next couple of months.
There’s a third-generation BTK inhibitor called pirtobrutinib, which is not yet FDA-approved, but it’s on track and there’s a lot of data presented about this drug.
Currently, FDA approved for CLL are two BTK inhibitors: ibrutinib and acalabrutinib. In terms of deciding which drug to choose between these two, for my patients, I really look at the efficacy and safety profile of these drugs.
There are a couple of trials done in patients with relapsed CLL, [those] who had prior therapy for their CLL then their disease came back. Half of the patients were given acalabrutinib [while the other] half of the patients were given ibrutinib.
What those studies showed is that those drugs were equally effective but acalabrutinib [had] less toxicity. Based on that and some other data, I preferentially [use] acalabrutinib these days as the BTK enabler of choice for my patients.
Again, that argument may change a bit when zanubrutinib comes [into] the picture, and certainly down the line when we get pirtobrutinib. That would be another exciting addition to the field of BTK inhibitors.
Andrew: Okay, so that’s really going to be physician and patient choice, it seems. They’re all good drugs.
Dr. Jain: It will come down to the physician, how comfortable they are using a particular drug for their patients, and the medical data and how they look at it.
I present all these options to my patients, discuss some of the clinical trial data and big picture view, give my recommendations to the patients for the treatment, and follow what their wishes are.
Andrew: Then also in this discussion is what other conditions a patient might have, right? Do they have a heart condition or other things that would determine which medicine you might go with, correct?
Dr. Jain: You’re absolutely correct. One of the things we [are] concerned about is the side effect profile. Some side effects are bone aches, muscle aches, diarrhea, and skin rash. [They] certainly can be an issue and some patients require dose reductions, especially for ibrutinib.
Some things are somewhat less common but can be more serious, such as atrial fibrillation, which is an abnormal rhythm of the heart, hypertension, which can become a problem for some patients, or bleeding issues.
If a patient has some of those medical conditions ongoing — heart issues, recent heart attack, or heart rhythm issues — then many times, I try to stay away from BTK inhibitors and use venetoclax, which is a Bcl-2 inhibitor. Among the BTK inhibitors, that will really make the case for second-generation agents, which are less toxic in terms of cardiovascular side effects.
Andrew: There’s data coming out related to zanubrutinib, not yet approved, but whether there are [fewer] concerns related to that for some patients, am I right?
Dr. Jain: Yes, correct. Similar to acalabrutinib, zanubrutinib was also studied head to head [compared] to ibrutinib in relapsed CLL. In that study, they showed that there was less atrial fibrillation with zanubrutinib compared with ibrutinib. That’s the first time two BTK inhibitors were compared head to head and they’re also showing that one is more efficacious than the first.
Ibrutinib
Andrew: Let’s just talk about the one that’s been around a long time: ibrutinib. There are thousands and thousands of patients on it. If they’re doing well, there is not necessarily a reason to change, right?
Dr. Jain: I agree with you and I think that’s a very important question from a patient standpoint. I get asked this question all the time in the clinic because ibrutinib certainly was the first drug [on] the market. It really changed how we manage these patients and really dramatically improved the outcomes of our patients.
But now, we are seeing some side effects of these drugs. There are patients who have been on ibrutinib for years and years — five years, seven years, nine years — and they are tolerating the drug well, [with] no side effects, [and] disease is well controlled.
I’m not switching those patients to a different agent at this time. We continue to use ibrutinib. However, if they’re starting [to get] side effects, then we look into moving to a different agent.
Andrew: There’s a significant percentage of CLL patients who are on watch and wait for an extended time. Is there any new thinking about doing anything differently now or is that still the standard in CLL?
Dr. Jain: As a CLL research group, we are investigating whether you can treat certain patients with CLL who are [at] high risk for disease progression early on, for example, patients who have deletion 17p and high-risk disease unmutated IGHV gene.
These are patients [who] we expect to progress a bit faster. Their time to treatment after CLL diagnosis is probably shorter than other patients with CLL.
There are ongoing randomized studies in the United States where patients with CLL are randomized. Either [they are treated] right away with venetoclax-based therapy or we watch these patients and whenever the disease progresses, which could be several years down the line, at that time, they receive venetoclax-based therapy.
That’s an ongoing and very important trial in the field. We’ll have to wait to get that medical data.
The current standard remains the same. We should watch these patients until they meet our CLL treatment criteria, which is basically having low blood counts, low hemoglobin, low platelets, big spleen, big liver, big lymph nodes, or significant symptoms from the disease affecting [their] quality of life. If you meet those criteria, then we treat [you].
Venetoclax + ibrutinib
Andrew: We talked about single-agent therapy with BTKs primarily, but you gave a presentation with longer data on ibrutinib plus venetoclax. Tell us about that and whether that combo has promise for people.
Dr. Jain: Both ibrutinib and venetoclax are FDA-approved for patients with CLL. Back in 2014, our group and many other groups showed data that combining these two drugs together is actually [more] synergistic for the two in the lab. Based on that, we started this clinical trial of combining ibrutinib plus venetoclax, two oral drugs together, for patients with CLL.
We treated 120 patients at MD Anderson. These patients have never received treatment so this is the first treatment for CLL.
Almost 70% of patients achieved MRD-negative remission in the bone marrow after getting these two oral drugs. We saw very few relapses over the course of four years. Our four-year progression-free survival was 94%.
The importance of getting an infusion vs. oral medications
Andrew: How important is it to get that infusion versus these oral medicines?
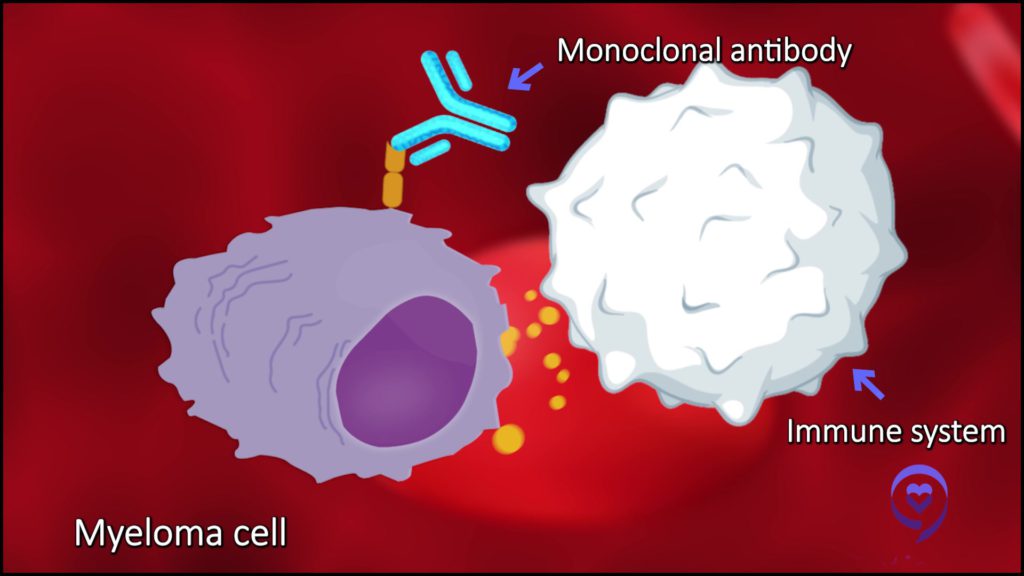
Dr. Jain: That’s an unanswered question in the CLL field right now. We know that the CD20 antibody infusion, whether it’s rituximab or obinutuzumab, works very well when we combine it with chemotherapy [and] also works very well when you combine venetoclax.
There is some conflicting data when you combine rituximab with ibrutinib; it doesn’t really work that well with ibrutinib. However, obinutuzumab, which is second-generation rituximab, works a bit better when you combine [it] with acalabrutinib.
Now when we combine ibrutinib plus venetoclax together, the two most potent drugs we have for CLL, we are already seeing very high rates of remissions.
The question is: can you improve that further by adding an antibody? This is the question of doublet versus triplet. Two drugs versus three drugs.
When we designed the study, we did not elect to use the antibody because we thought [that] antibody would add more toxicity than benefit. However, there are other medical data with triplets, which [have] been reported as well.
Right now, it’s very difficult to say because all these drugs are very, very effective regimens. Doublets versus triplets, it’s really difficult to tease out if one is better than the other.
There are ongoing randomized controlled trials where they are evaluating doublets versus triplets. I’m hoping we’ll hear from some of these trials in one to two years. Then we can have a more informed decision [about] whether you really need to have CD20 antibody when you’re using these two older drugs together.
What is the advantage of a third-generation BTK inhibitor?
Andrew: You’ve mentioned pirtobrutinib, which is a third-generation BTK in trials. What would be the advantage of a third generation? How would that be different?
Dr. Jain: Pirtobrutinib, previously called LOXO-305, is a third-generation BTK inhibitor. The main advantage here is that, unlike the first two generations of BTK inhibitors, namely ibrutinib, acalabrutinib, and zanubrutinib, they bind to a very specific protein pocket.
They bind to a residue called cysteine 481S, which attaches to these drugs. These patients, when they relapse, develop resistance mutations and then these drugs cannot bind to that pocket.
However, pirtobrutinib is a non-covalent inhibitor. It does not need that residue to bind. It just blocks the pocket. That’s why it’s able to work for patients who have failed ibrutinib, acalabrutinib, or zanubrutinib. That’s one advantage that pirtobrutinib can work against patients who have failed previous BTK inhibitors.
The second advantage is safety. We have seen [an] excellent safety profile of this drug with very few patients having atrial fibrillation, bleeding complications, or any other major issues. What we know so far is that this drug works very well and it’s also very well tolerated.
New data on Richter’s Transformation
Andrew: A small percentage of CLL patients develop a much more aggressive condition called Richter’s Transformation. Is there progress being made there? Any news that gives hope in treatment for Richter’s?
Dr. Jain: Richter’s Transformation remains a tough disease. We are working on several clinical trials looking at new pathways to control the disease, including immune checkpoint inhibitors using venetoclax. One was actually pirtobrutinib.
When you use this drug as a single agent for patients who had Richter’s Transformation, almost half of the patients respond to the treatment and the response lasted for several months. That is one important agent for patients with Richter’s Transformation.
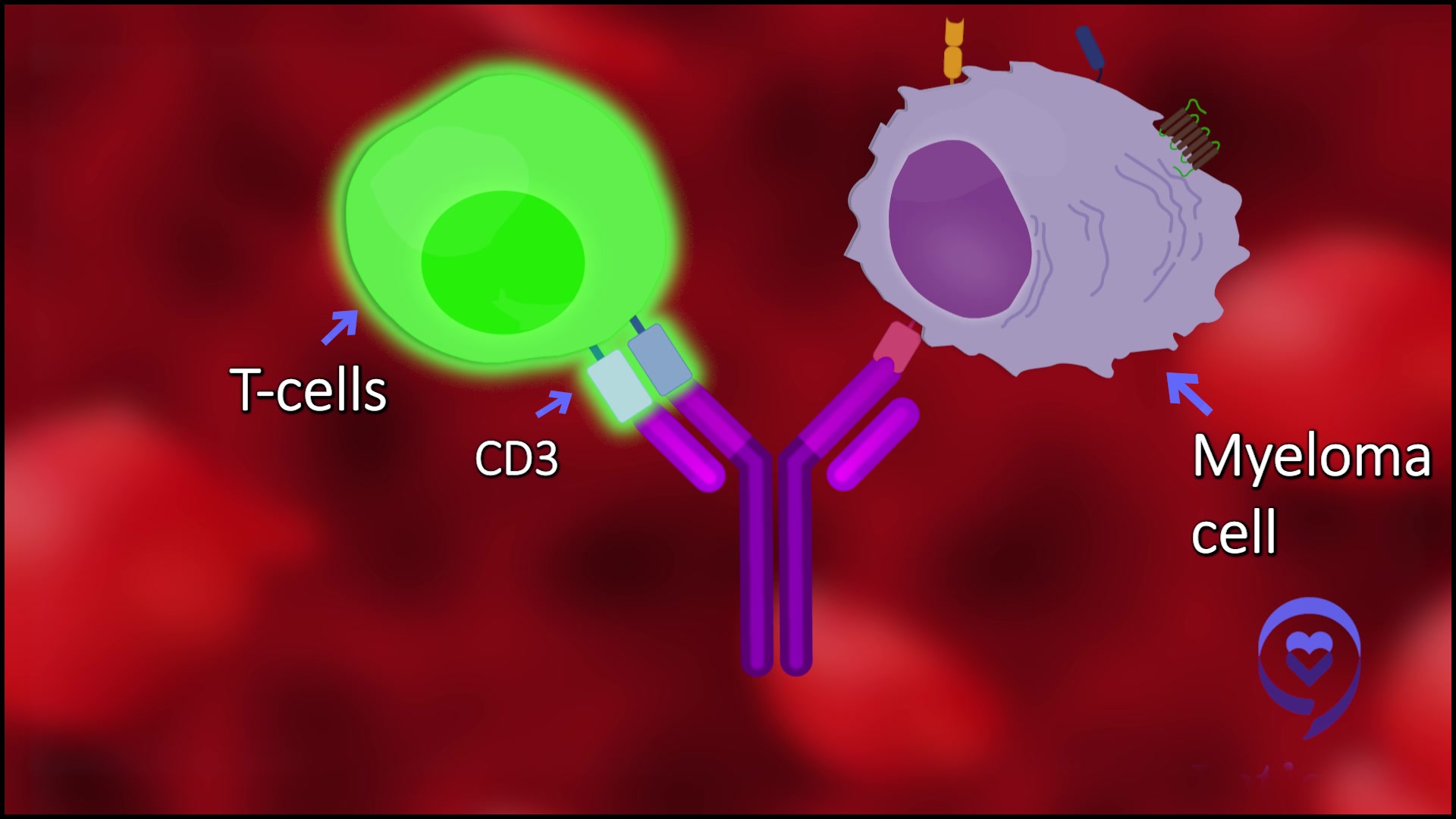
There’s also this new class of drugs called bispecifics, which on one hand bind to a protein called CD20, which is on the cancer cells, the CLL cells, or Richter cells, and then on the other hand, they bind to a protein called CD3, which is on the T cells.
What they do is bring the cancer cell and the T cells together. That has been shown in several trials to be very effective in diffuse large B-cell lymphoma. There is data presented [on] clinical activity for patients with Richter’s Transformation as well.
Those are two important classes of drugs being pursued [in] clinical trials.
The third one is CAR T-cell therapy that also several studies have started to evaluate for Richter’s Transformation, but no specific medical data was reported.
Andrew: Okay, let’s pull all this together. People are still in watch and wait, and that’s fine if their quality of life is not diminished, their blood counts are strong, etc. But when they move on to treatment now, it seems like there’s a discussion about which BTK might be right for them and whether or not they should consider BTK, still investigational, with a second drug like venetoclax. Is that correct?
Dr. Jain: Yes, correct. Absolutely.
Andrew: You have this whole line of tools that we haven’t had for that long and for people with aggressive transformation, there seems to be a glimmer of hope as well. If you had a new patient today, would you say that the likelihood is they can probably live a long and full life? You have medicines that may not cure the CLL — although sometimes you feel CLL is cured — but they can live long and live well.
Dr. Jain: Oh, absolutely. That’s exactly what I tell my patients these days, especially patients who are newly diagnosed. [When] they come for the first visit, obviously, [there are] a lot of questions in their mind. Hopefully, all patients with CLL can expect to live a normal lifespan with good quality of life.
We have excellent medicines for patients right now and the field is improving. [We have] other important, better medications, safer medications, immune therapies, [and] CAR T-cell therapies coming down the line.
I really, truly believe that we’ll be able to have patients with CLL have a normal lifespan. An important point is that you don’t need [a] cure to live a normal lifespan in the context of CLL.
You could have a small amount of disease present, but if it’s not interfering with your quality of life, your blood counts, your health, [and] what you do in your life, you can just continue to live with a very low level of the CLL.
Overall, we’re in very, very good shape in terms of the treatment paradigm for CLL patients. We’re all making really good progress.
CAR T-cell therapy
Andrew: I know CLL patients who’ve had CAR T-cell therapy. It is not yet approved. What is the future of chimeric antigen receptor T-cell therapy for CLL? It’s approved in some other blood cancers, but not yet in CLL.
Dr. Jain: I think this is one of the biggest advances in the last few years, I would say, in the context of blood cancers. It’s not approved for CLL, but [for] lymphomas, leukemias, [and] myeloma.
The field has somewhat lagged behind and we don’t have much clinical data yet. There are [a] few trials, which have been reported, but not very many.
There’s a lot of interest and discussion in general with investigators to develop CLL-specific clinical trials with some new constructs.
CAR T-cell therapy is very dependent on what kind of genes are inside of the CAR so it’s very technologically heavy where even small changes in what gene you insert can make big differences [in] how patients do. There’s a lot of effort happening [on] the lab side to draw up new constructs, which specifically could work for patients with CLL, also for patients with Richter’s Transformation.
That’s an area where I think many more clinical trials will come. In one to two years, I think we’ll have somewhat more clarity of the data in terms of CAR T-cell therapy for patients with CLL as well as for Richter’s Transformation.
Andrew: Okay. What you’re touching on is: can we get the immune system to fight the CLL and do it long term, correct?
Dr. Jain: Correct. From [the] chemoimmunotherapy era to target therapy era, now we are asking our immune system to dress [for] the job and take care of stuff.
Immune therapy works very well for melanoma, for solid tumors. So can we use our immune cells to help get rid of the CLL?
Andrew: It sounds like a great time of progress for those of us living with CLL. With the current therapies, some that may be approved even in the short-term, combinations, and then this work going on in immune therapy that’s happened in some other areas and where this pays off for us.
Dr. Jain, thank you so much for being with us on The Patient Story. We wish you well with your research and your clinical care of patients at MD Anderson.
1st symptoms: Tightness, lumps in left side of neck, severe pain in left shoulder, enlarged spleen Treatment (CLL): 6 cycles of EPOCH, clinical trial for DuoHexabody-CD37
Robyn, a three-time DLBCL survivor, and two top lymphoma specialists, Dr. Tycel Phillips from the City of Hope and Dr. Joshua Brody from Mount Sinai, discuss the latest DLBCL treatments and developments happening in the most common subtype of non-Hodgkin lymphoma: diffuse large B-cell lymphoma (DLBCL).
DLBCL, diffuse large B-cell lymphoma, is the highest incident lymphoma in America. Every year, about 90,000 people [are] diagnosed with lymphoma [and] about 25,000 of those are diffuse large B-cell lymphoma.
Dr. Josh Brody
Introduction
Stephanie Chuang, The Patient Story: I went through non-Hodgkin lymphoma treatment back in 2017 so this is a topic that’s very near and dear to me. My own experience as a cancer patient is what motivated me to start something to really help humanize the cancer experience for those of us who don’t have a science background. That was the genesis of The Patient Story.
We reach cancer patients, care partners, [and] caregivers with content; mostly in-depth stories. We also highlight conversations with specialists in the field.
The goal is to humanize cancer. What does that mean? It means you’re not alone and here’s some information we hope will be helpful.
The focus in this webinar, is the latest in DLBCL treatments and research. We have three doctors: two lymphoma specialists and one who is a three-time DLBCL survivor.
Dr. Joshua Brody is from Mount Sinai and Dr. Tycel Phillips is from [the] City of Hope. Robyn spent years on the medical side, started off [as a] radiologist seeing patients, and then became a patient [herself].
What is DLBCL? What is the standard care for first-line treatment?
Stephanie, TPS: Let’s set the stage. We hear about DLBCL a lot. Dr. Brody, what is DLBCL and what is the standard care for first-line treatment?
Dr. Josh Brody: DLBCL, diffuse large B-cell lymphoma, is the highest incident lymphoma in America. Every year, about 90,000 people [are] diagnosed with lymphoma [and] about 25,000 of those are diffuse large B-cell lymphoma.
We have about 84 types of lymphoma. People say, “Wait, do I have the good one or not?” It’s not just two types. It’s not the good one and the bad one. We divide these lymphomas into many ways so we don’t have to memorize a list of 84 things.
The first way we divide them is Hodgkin’s and non-Hodgkin’s. We are talking about non-Hodgkin’s lymphoma. We divide non-Hodgkin’s lymphoma into B-cell and T-cell lymphomas. We’re talking about B-cell lymphoma. Then we sometimes divide B-cell lymphomas into low-grade versus aggressive. Low grade, these grow very slowly: follicular lymphoma, marginal zone lymphoma, [and] some others. The aggressive lymphomas, diffuse large B-cell [is] the most common of them. Maybe you’ve heard of Burkitt lymphoma, mantle cell lymphoma, [and] some of these other things that can grow more quickly.
We’re so lucky because the treatments for lymphoma have evolved more rapidly than for any other cancer in the world. Even though we are the fifth most common cancer, we have more FDA-approved medicines than any other cancer. The reason is [that], thankfully, the progress has been very rapid. We don’t get FDA-approved medicines without progress to prove that those therapies can be pretty good.
Over the past 20 years, the standard therapies for diffuse large B-cell lymphoma [are] these alphabet recipes. R-CHOP sounds a little aggressive and it is, as Robyn can tell you. People that are working full-time before R-CHOP are frequently working part-time during R-CHOP so it’s aggressive enough that it affects your life in a real way. It affects your hair.
R-CHOP is not the most aggressive stuff we have. It is standard therapy. Today, it may not be the only standard front-line therapy. There are a couple of slightly new versions of R-CHOP that are options now. I will say that five years from now, I don’t think R-CHOP will be the standard. I think we’ll even have some better things.
The R [is] rituximab. It is immunotherapy — targeting lymphoma using your immune system to kill those lymphoma cells, but not powerful enough by itself. The P is prednisone. The CHO is chemotherapy.
All the side effects you’ve heard about with chemotherapy — hair falling out, a little bit of nausea — not so bad, but it’s a real thing and some of these other side effects you heard about.
R-CHOP, thankfully, cures about 60% of people with DLBCL — not every type of DLBCL, but overall. That’s pretty good. We’re lucky to be able to cure 60%. Not that lucky if you’re in the other 40, though, as Robyn or lots of our patients could tell you.
We actually have a lot of progress and probably still some curative things. A lot of progress, more so than probably any other cancer, and yet a lot of room for improvement still.
The treatments for lymphoma have evolved more rapidly than for any other cancer in the world. Even though we are the fifth most common cancer, we have more FDA-approved medicines than any other cancer.
Dr. Brody
Stephanie, TPS: I do want to ask Dr. Phillips to lay out the options. If somebody relapses in the first six [or] 12 months, how different is that prognosis or treatment?
Dr. Tycel Phillips: For patients who do not respond to R-CHOP and immediately relapse — what we consider primary refractory patients and that likely extends out at least into the first six months — those patients have done very poorly historically with a lot of the standard options that we have, like RICE, which are just various combinations of chemotherapy drugs. Hopefully, not cross-resistant to each other [and] provide a different mechanism of action compared to the drugs using CHOP with rituximab as well, with the goal of getting them to autologous stem cell transplantation.
Again, historically, that group has done fairly poorly because they are probably chemo-resistant. They’re not going to respond to any sort of chemotherapy drug. The whole design of chemotherapy is to prevent DNA replication or cause DNA damage at some point during the replication cycle. If a cancer drug has figured out a way to get past one, it’s likely to figure out a way to get past most of the rest.
An auto transplant really should be named an autologous stem cell rescue because it’s still just more chemo. It’s not anything fancy about the stem cells that you’re getting back there, just your own stem cells to rescue your body.
For the most part, a lot of the clinical trials that help these relapsed/refractory regimens are probably heavily dependent on these relapse patients, which are generally the patients who relapse a year or so after chemotherapy.
These are the reasons why we get the response rates for most of these regimens, such as RICE, DHAP, and the big CORAL study, which was a big regimen looking at these relapsed/refractory regimens to see which one was better. They’re really probably driven by refractory patients again because these are relapse patients. These refractory patients are not the ones that are going to drive these studies.
A lot of big emphasis recently has been on other ways to treat these patients, especially these early refractory patients or patients who relapse within six months to a year with other regimens besides chemotherapy, which brings into the CAR T discussion.
For patients who can’t get to CAR T or who are ineligible for CAR T, in the second-line setting beyond chemotherapy, there is lenalidomide and tafasitamab, which are for patients who are ineligible for autologous stem cell transplantation. That regimen itself, at least from the clinical trial, seems to be more effective in those who have only received one line of therapy versus those who are heavily pre-treated, meaning they have two or more prior lines of therapy before [receiving] this drug.
In that second-line setting, there aren’t a ton of other agents approved, even though we have options such as polatuzumab-bendamustine-rituximab. We are a bit hesitant to use that regimen in some sense because the bendamustine does cause quite a bit of depletion of your immune system, specifically T cells. The T-cell depletion can be quite profound and prolonged, which can hamper things that depend on T cells to be effective, like CAR T, etc.
There also is a new agent recently, which is a CD19 drug antibody conjugate called loncastuximab, which has a very different drug attached to it, which is a little bit different from MMAE, our usual antibody drug target. That is also another option.
Then there is selinexor, which is [an] export one inhibitor [that] was approved [for] this patient population, but probably has very little uptake because of the toxicity of the agent.
If we’re looking at currently approved agents, the chemo or the regimens I just mentioned are the currently only approved ones outside of CAR T at this point.
A lot of big emphasis recently has been on other ways to treat these patients, especially these early refractory patients or patients who relapse within six months to a year with other regimens besides chemotherapy, which brings into the CAR T discussion.
Dr. Tycel Phillips
Bringing up different treatment options with your hematologist-oncologist
Stephanie, TPS: Robyn, you’ve been through a lot: different kinds of chemo, chemoimmunotherapy regimens, auto stem cell transplant, and eventually CAR T. It sounds like you were the one who researched CAR T. How did you bring up the discussion of CAR T with your hematologist-oncologist? What were the differences for you in terms of going through the stem cell transplant and then going through CAR T?
Robyn: Overall, I did extremely well. The auto stem cell transplant was extremely difficult for me. I was very, very sick. [It was a] terrible experience. I did survive. I’m here, but I didn’t want to go through that again.
When the auto stem cell transplant failed, I did not want to go through an allo (allogeneic) transplant.
I’d gone online. There’s a site called www.clinicaltrials.gov. Anybody can get online. I really had no advantage being a doctor except that I had heard about the site so I had started looking at different trials. My husband, who’s an engineer, and I both looked at all these different trials and emailed investigators when I relapsed. We just tried to find a space and a trial.
I just thought that was the right decision for me. It was not recommended by my oncologist. [As] a matter of fact, my oncologist thought that I should go ahead and have an allo transplant using my son as a donor, as a haplo (haploidentical) and I didn’t want to do that.
I looked at it on my own. Nowadays, things are very different. In 2016, there was only one phase 1 clinical trial for Kymriah, which is what I had. I based my decision on 26 patients and 12 went into remission, which is not a big number. My oncologists were not comfortable with that, but somehow, I felt that was the right decision for me. Everyone is unique.
I did get different opinions from other oncologists. I was a very complex case. I was a younger patient who was healthy. But I was so sick during the stem cell transplant with septic shock and that helped determine what I decided to do.
Everyone is unique and it’s a big decision, but I wanted to live my life and not have the risk of graft versus host disease, which could actually limit the enjoyment of life and so that was also within my decision.
I just thought that [CAR T] was the right decision for me. It was not recommended by my oncologist. [As] a matter of fact, my oncologist thought that I should go ahead and have an allo transplant using my son as a donor, as a haplo (haploidentical) and I didn’t want to do that.
Robyn S.
Stephanie, TPS: It’s a great example of this equation. For everybody, it’s a different equation in terms of what you weigh more heavily. Is it how long you think you can get more out of life in terms of survival or is it quality of life?
Drs. Brody and Phillips, I know that this happened back in 2016 so it’s a very different landscape than now. But anything you want to add in terms of the decision-making or talking about this with a patient?
Dr. Phillips: She highlighted a very important dilemma we have. The decision for an allo transplant is probably very controversial amongst lymphoma doctors. You have some people who are very beholden to it and others who probably would never send a patient for an allo transplant based on what Robyn has already mentioned. The simple fact of the risk of graft versus host disease, finding an appropriate donor, and, with lymphoma, actually making sure the cancer is in remission before you get to an allo.
I wish we had a better system to illustrate clinical trials throughout the US. I don’t think we still have a great system, even in 2023. A lot of us depend on clinicaltrials.gov or word of mouth versus having a good system where any patient can just plug in their disease and we pop up all these studies and trials that are actually active and open.
That’s the thing about clinicaltrials.gov. Just because they list sites doesn’t necessarily mean those sites are actually up and active, which I think a lot of people don’t realize.
Dr. Brody: I agree with everything Tycel said. Robyn was either lucky or prescient or maybe a combination because in retrospect, if it was me, CAR T versus allo transplant, it would be a no-brainer.
We now have randomized trials comparing CAR T to autologous transplants for those that relapse quickly, 12 months after front-line therapy. CAR T is probably both more effective and kinder with less of those toxicities. CAR T can be toxic, but overall, head to head, I would probably rather get a CAR T-cell therapy than an autologous transplant. I think most people would probably agree.
It’s tricky. If you’re a specialist, you think that’s the way to go. A transplant doctor will say, “Yeah, we could do [a] transplant.” It’s the same with clinical trials. If you’re a doctor that doesn’t focus on clinical trials, you won’t think of that. It won’t come to mind.
Robyn is one of these rare people that can advocate very well for herself. You do need doctors sometimes to be able to help advocate for you.
The last time we looked, 25 to 30% of patients that are eligible are getting CAR T. That means the vast majority of patients are not getting CAR T.
Dr. Brody
What is CAR T-cell therapy?
Stephanie, TPS: I love that, Dr. Brody, thank you.
Let’s talk about CAR T more in depth. What exactly is CAR T-cell therapy and what does it entail in terms of how people actually go through it?
Dr. Brody: We take a little bit of a person’s immune system, some immune cells from their blood. They literally do gene therapy on your immune cells. They put a new gene into your immune cells and when we put [them] back into you, that gene allows those immune cells to go find lymphoma and then kill lymphoma.
Humans have about 20,000 genes. This gene that they stick into those immune cells is not one of those 20,000. It’s amalgamated from five other genes put together into one gene. That gene is called CAR, a chimeric antigen receptor. You get FluCy (fludarabine and cyclophosphamide) chemo and then we re-infuse the CAR T cells.
A few years ago, we would say folks with multiple-relapsed DLBCL didn’t have curative options just like patients with metastatic breast cancer. In those patients, we would say the CAR T-cells might cure 35 to 40% of patients. Going from what we call 0% to 40% sounds like it’s miraculous. Not 100% so still a lot of room for improvement. The efficacy is very impressive, miraculously impressive, but it’s not benign therapy.
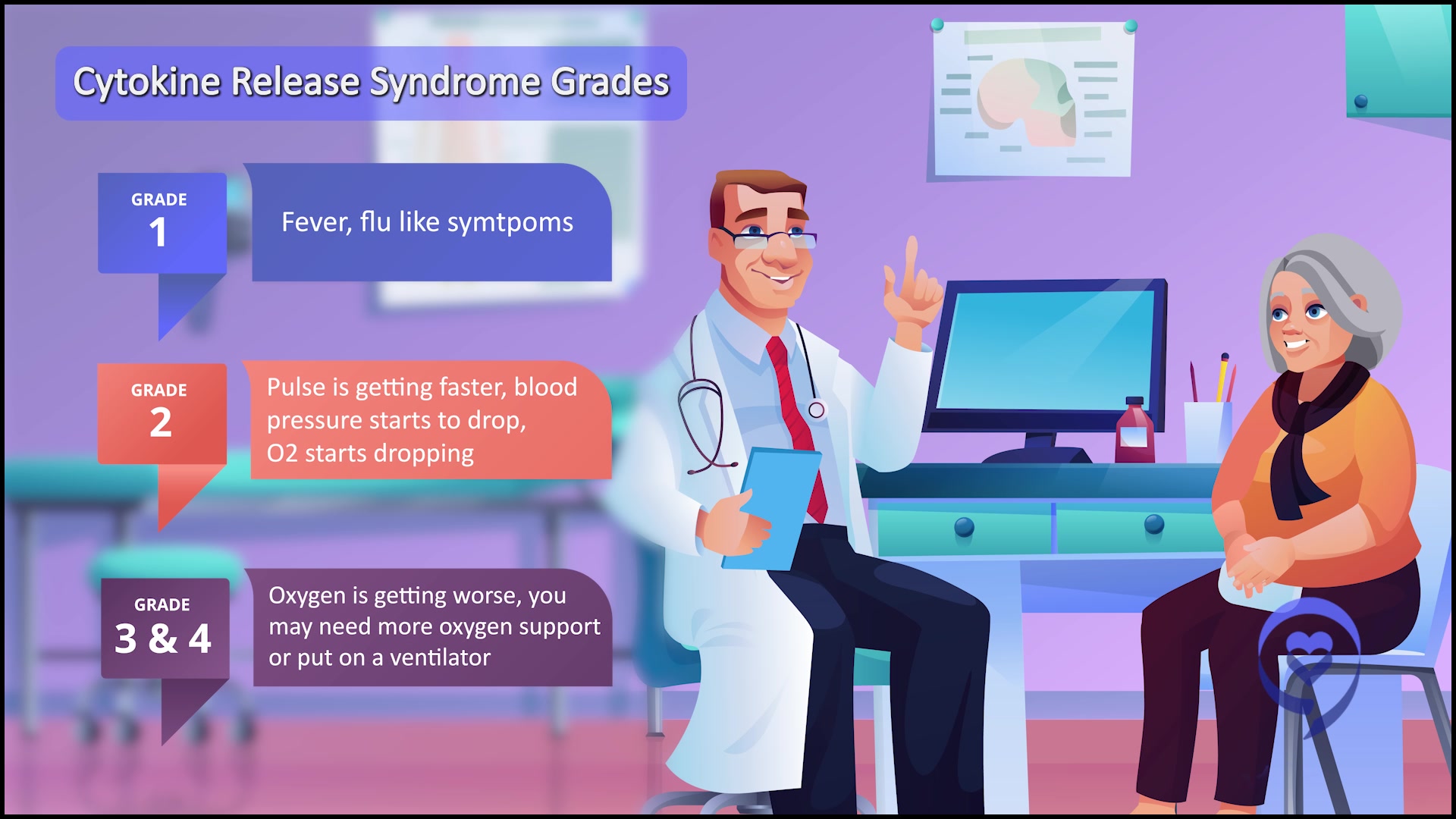
There is this risk of side effects and probably 20% of people get some of these high-grade side effects. The most commonly discussed one [is] cytokine release syndrome, CRS. It’s like having a terrible infection, but there’s actually no bacteria [or] virus infecting you and people can land in the intensive care unit because of that.
Another one [is] neurotoxicity [or] ICANS (immune effector cell-associated neurotoxicity syndrome). It can literally be a type of encephalopathy. People can start hallucinating [or] become unconscious. It can be dangerous.
These high-grade toxicities might happen in up to one in five patients. Even if it doesn’t happen in the other four out of five, we don’t know which one in five is it going to happen [to] because we have to monitor all of those patients very closely, usually in the hospital.
The last time we looked, 25 to 30% of patients that are eligible are getting CAR T. That means the vast majority of patients are not getting CAR T.
Dr. Phillips
Benefits and challenges of CAR T-cell therapy
Stephanie, TPS: With that being said, Dr. Phillips, if you could just touch on the benefits and the challenges?
Dr. Phillips: The biggest excitement is that we’ve been all talking about immunotherapy for decades and here we are with a true immunotherapy with a much better and manageable safety profile than what we typically would see with an allogeneic stem cell transplantation.
The uptake of CAR T is not what it should be. The last time we looked, 25 to 30% of patients that are eligible are getting CAR T. That means the vast majority of patients are not getting CAR T due to access issues, meaning they can’t get to a CAR T center, or they don’t have anybody that needs to be there with them or relocate to a center for a month to get CAR T.
These are all logistical challenges that we are trying to fix and overcome along the way, but it’s not been necessarily the easiest thing to get over because these patients will need caregivers, especially as we’re trying to move CAR T to an outpatient setting. They have to have somebody that can take care of them.
Financially, I don’t think CAR T is going to be feasible moving forward where, originally, patients are hospitalized for 30 days. Unfortunately, payers aren’t going to pay for that and hospitals can’t [foot] the bill for that any longer.
They do need some support to help take care of them, which is not unfortunately dissimilar to what we see with transplant patients. The hope is that requirement may ease for some patients who aren’t necessarily going through complications. But right now, unfortunately, it is a requirement in most centers that they have somebody to take care of them.
CAR T-cell therapy for refractory patients?
Stephanie, TPS: [With] refractory patients, [they undergo] different treatments [and] there’s no response. It’s not [that] you were in remission and then you relapsed. It just didn’t respond. When would you consider CAR T for someone in that position?
Dr. Phillips: Thankfully, now, in second-line. That generally would be the immediate treatment at this point, unless there’s some reason that they can’t get CAR T.
Those patients should be the patients we get to CAR T because we already have two studies that have demonstrated that CAR T was superior to autologous stem cell transplantation with both axi-cel and liso-cel in this patient population. This is the ideal patient population for CAR T.
The key thing with bispecifics, at least from what we can see from the early stages, is that they appear to be effective in patients with relapsed/refractory diffuse large B-cell lymphoma.
Dr. Phillips
What are bispecific antibodies?
Stephanie, TPS: Wonderful. Now let’s get into bispecific antibodies. Dr. Phillips, what are bispecifics?
Dr. Phillips: The easiest way to think about bispecifics is like [an] off-the-shelf CAR T product. It still works to utilize your own T cells to fight off cancer, but instead of the manufacturing process, it basically administers an antibody that will bind to some marker in your cancer, bind to your T cell, which will force an interaction between the two, [and] lead to T-cell activation and [hopefully] some sort of T-cell expansion, growth, etc.
These antibodies, at least the CD20/CD3s and some of the newer CD19/CD3s, are a bit better than what we have with blinatumomab, which was given as a continuous infusion, by allowing those Fc portions and just muting them to be still intact to the antibodies. They have a much longer half-life so these things can be administered more conveniently.
If we look at the agents that we have that will likely get approval, we have mosunetuzumab, which is approved for follicular lymphoma. [This] is given as a step-up dosing once a week until you get to [a] full dose and then once you reach full dose, given every three weeks for either eight or 17 cycles.
We have epcoritamab, which will likely get approval for diffuse large B-cell lymphoma. Again, given in a step-up dosing every three weeks, but will continue weekly through the first three cycles and biweekly from cycles four through nine, and then once a month indefinitely.
Then glofitamab, which is another CD20/CD3 bispecific antibody given in step-up dosing. This one is given with a pre-medication obinutuzumab to help reduce the risk of CRS, which is still prevalent because it’s a T cell-directed therapy, and then given once every three weeks thereafter. This one is also given for a fixed dose of just 12 cycles.
Then we have odronextamab [and] plamotamab in the pipeline of other bispecific antibodies and there are many more coming down the line.
The key thing with bispecifics, at least from what we can see from the early stages, is that they appear to be effective in patients with relapsed/refractory diffuse large B-cell lymphoma. Some studies have shown that they are effective in patients post-CAR T. The question that we’ll get into later is: which post-CAR T patient is actually a patient that’s going to respond to a bispecific?
The same side effects exist. CRS occurs, probably not to the severity and intensity [that] we see with CAR T and the management strategy will probably end up being a bit different. There is ICANS or neurological toxicity. Again, not to the degree of severity that we see with CAR T but still present.
A lot of community physicians and patients will get first-hand experience, good or bad, with these bispecifics and, hopefully, more guidance will get out there for how to best manage some of these events because a lot of these physicians haven’t dealt with this.
In a couple of years, hopefully, as more and more physicians get comfortable with these drugs, they’ll get more access to patients and they’ll be more comfortable managing the side effects. This will probably have a bigger catchment area just because of [fewer] restrictions on these drugs than what we see with really CAR T at this point.
We don’t want to confuse complete remission with cure. Just because we can’t see any cancer doesn’t mean there might not be a little bit left.
Dr. Brody
What is the comparison between epcoritamab and glofitamab?
Stephanie, TPS: Dr. Philips does a great summary of a huge space so [I] appreciate that. It sounds like, for DLBCL in particular, there are two that are a little bit more advanced in the studies than the rest although there are many that we should be watching out for. Dr. Brody, between epcoritamab and glofitamab, anything you see with the response so far [in] the clinical trials?
Dr. Brody: Overall, these two are much more similar than different.
They’ve been in many hundreds of patients. They focused on a trial of about 150 patients each and both had complete remission rates of about 39%, 39.4% for both of them so that’s pretty similar. Again, just under 40% of people. The tumor melts and disappears so that we cannot even see it on a PET scan or a CT scan.
We don’t want to confuse complete remission with cure. Just because we can’t see any cancer doesn’t mean there might not be a little bit left. But it does seem like a lot of these complete remissions are very durable [and] very long-lasting.
We definitely have patients in complete remission from these therapies for more than two years. We don’t have five years yet because these medicines haven’t been around for five years. But if a person stays in complete remission for two years, the chance of being cured seems to get pretty good. That’s true for many therapies, certainly for CAR T and for other therapies.
One little difference between them is the way they are administered. Epcoritamab is given as a subcutaneous shot, just a shot under the skin, so pretty quick. Glofitamab is given as an infusion. The first infusion is eight hours. Later on, it becomes four hours and two hours. A little bit more time intensive there, but not too bad. Maybe that’s a point in favor of epcoritamab.
I’ll give a point in favor of glofitamab, to be fair. The glofitamab studies are mostly designed to be time-limited. You get 12 cycles, about nine months of glofitamab, and then you just stop the therapy and you’re in complete remission. We just keep an eye on you. If you were to relapse, you could get more of it, but if you’re in complete remission, we just stop giving the therapy. That’s just how they were designed so we don’t have to give it forever.
The epcoritamab studies have been designed to just keep going. As long as the person is in remission and doing well, just keep giving it.
It’s hard to say which one is better [or] worse. I find half of my patients like the idea of, “Yeah, give me a break. I’ve been through a lot,” and [the other] half say, “I don’t know. I kind of want to keep getting this therapy.” We don’t know which one is right or wrong. Some people see the benefit of time-limited therapies. They don’t have to keep coming to the doctor as frequently.
Maybe a little bit of benefit of one over the other in both directions but, overall, more similar than different, [with] remarkable efficacy, and much easier to use than CAR T cells.
If I do not have a caregiver and someone’s recommending CAR T, what kind of options come up there? [The] one-word answer is bispecifics.
Conceptually, it’s the same possible side effects, but, thankfully, we’ve mostly just seen much less of them and lower-grade versions of them.
Dr. Brody
Side effects from bispecific antibodies
Stephanie, TPS: Assuming bispecifics are approved and it’s not being used as a clinical trial for somebody, what about the side effects, Dr. Brody? Dr. Phillips did [mention] CRS seems to be [a] lower grade in bispecifics as opposed to CAR T. Anything else?
Dr. Brody: As Tycel said, conceptually, it’s the same possible side effects, but, thankfully, we’ve mostly just seen much less of them and lower-grade versions of them.
The average CAR T-cell patient today is sometimes still spending 11 days in the hospital just for observation, whereas the average bispecific antibody patient usually spends one day in the hospital. Even though the vast majority of them don’t get any of those side effects, at the moment, we have to still observe them all just to make sure that we don’t miss the one out of ten that gets the bad side effect.
For DLBCL, the plan with most bispecifics still is at least one day of observation. Probably about 5% can get the high-grade version of CRS and much less than 5% get neurotoxicity. Rare, but it can happen and, therefore, requires a bit of monitoring.
If I have access to both, if I can’t get CAR T, then ideally, a bispecific is good in that situation.
Dr. Phillips
Statistically, you would want to get both.
Dr. Brody
CAR T or bispecifics for relapsed/refractory patients?
Stephanie, TPS: How do you consider which one to go to first for relapsed/refractory patients? What are the considerations?
Dr. Phillips: CAR T has the more definitive data so if you have access to both, you’re hard-pressed to put a bispecific before CAR T at this current date. I would say CAR T then bispecific thereafter, pending the response to the patient with CAR T.
If the patient has no response to CAR T, I have very little faith that they will have a response to a bispecific. We’d feel much, much [more] comfortable if a patient had some sort of response to CAR T [and] then lost it to try to resurrect that response with the bispecific.
But if I have access to both, if I can’t get CAR T, then ideally, a bispecific is good in that situation.
Dr. Brody: It’s actually less of a question of which is better, CAR T [or] bispecifics, because, frustratingly, for all the advances that we’re bragging about, the numbers are that the majority of patients are not cured by either.
Statistically, you would want to get both. You’d want to have the option to get both. As Tycel just said, if you get CAR T today and they fail 30 days from now, quite honestly, you probably won’t be able to get bispecifics because there [are] no trials that allow rapid failing CAR T patients to get access to bispecifics.
We’ve done the opposite in our patients quite a bit where they’ve got bispecific [and] if they stayed in complete remission, they kept going. But we had a few where they progressed eventually and we gave them CAR T-cells.
In a lot of cases, clinical trials are some of the best medical care that you’re going to receive.
Robyn S.
Clinical trials
Stephanie, TPS: I like that we’re comprehensive about this. We could talk about clinical trials really quickly because I think there’s a lot of misunderstanding. Robyn, you went through a clinical trial. Anything you want to say from the patient’s perspective? I think people think there’s a placebo or I’m going to be in an experiment and there’s a lot of fear. What would you like to tell people about your actual experience with a clinical trial?
Robyn: As a patient and also as a physician, it’s important that people realize that in a lot of cases, clinical trials are some of the best medical care that you’re going to receive. They’re cutting-edge. It is often the way to go in unusual cancers or some other diseases that can’t be controlled by anything else.
Dr. Phillips: That’s the thing people need to remember. It’s not guinea pigs. This is how we advance the field, especially in diseases without [a] standard of care. This is really your chance to get something that could potentially be life-saving. More people should be offered clinical trials.
Robyn: Keep your options open. Keep your mind open. Do some research. Read.
In this case, this is a blood cancer group. Talk to LLS if you’ve relapsed. See what their opinions are and get several opinions.
Be your own advocate. Physicians don’t agree on things, [which] doesn’t make somebody wrong or right. It’s a process. Science is not exact. It’s not black and white so you need to figure out what’s right for you. Do your research and don’t be afraid because a clinical trial might be the solution for you.
Stephanie, TPS: Thank you, Dr. Tycel Phillips, Dr. Joshua Brody, and Robyn. Thank you so much for making this such an enjoyable conversation about what could be very overwhelming.
Be your own advocate. Physicians don’t agree on things, [which] doesn’t make somebody wrong or right… You need to figure out what’s right for you.
Stephanie Chuang, founder of The Patient Story, celebrates five years of being cancer-free. She shares a very personal video diary with the top lessons she learned since the Non-Hodgkin lymphoma diagnosis.
Cancer details: Characteristics of both subtypes 1st Symptoms: Lower abdominal pain, blood in stool, loss of appetite Treatment: Chemotherapy (Part A: R-CHOP, HCVAD, Part B: Methotrexate, Rituxan, Cytarabine)
High-Risk Smoldering Multiple Myeloma Highlights from ASH 2022
What Newly Diagnosed Patients and Caregivers Need to Know
Jack Aiello
Multiple myeloma patient advocate Jack Aiello has been living with myeloma for 28 years.
In this conversation, he speaks with Dr. Shaji Kumar, a hematologist at the Mayo Clinic whose research focuses on the development of novel drugs for the treatment of myeloma.
They discuss the difference between smoldering myeloma and active myeloma, the determining factors of high-risk patients, and what high-risk smoldering patients can do to delay or possibly avoid progression to active myeloma.
Dr. Shaji Kumar
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Jack Aiello: I’m with The Patient Story. I’m a myeloma patient and have been for 28 years. I have followed this field very closely and always know that there’s more to learn.
Dr. Shaji Kumar: I’m a hematologist at Mayo Clinic in Rochester, Minnesota.
What is smoldering multiple myeloma?
Jack: Around 30,000 oncologists, researchers, physicians, pharma reps, and more from around the world attend the annual American Society for Hematology conference, also known as ASH, to hear the latest myeloma research from clinical trial investigators, like Dr. Kumar.
We’re going to primarily focus on a topic of myeloma called smoldering myeloma and that’s important because it’s a precursor to myeloma, although you may have never been diagnosed as smoldering.
Dr. Kumar, can you explain the differences between smoldering myeloma and multiple myeloma? And what determines high risk for smoldering vs. high risk for myeloma?
Dr. Kumar: With myeloma, we have precursor stages that clearly exist before patients actually get active multiple myeloma.
What we have learned is that the process that eventually leads to [the] development of active myeloma probably happens sometime in the 30s for many patients. We think it takes an average of about 15 years for that initial seed, so to speak, to grow into a stage where it is actually creating problems like active multiple myeloma does.
There are two distinct stages within this precursor phase. One of which is called monoclonal gammopathy of undetermined significance, essentially saying that you can find that initial condition. We can find some abnormal plasma cells, but they’re quietly sitting in the bone marrow, making protein that we can detect in the blood, which allows us to identify and diagnose this condition, but not really doing any major damage that we are aware of. We know that in some people, it can lead to some symptoms other than what we see in myeloma.
It’s important to note that this monoclonal gammopathy of undetermined significance is not something that is uncommon and certainly increases with age. In fact, if you take 100 people who are 70 years or older, you’re probably going to find that eight to ten of those people will have a monoclonal protein in their blood, suggesting that they do have this early condition that is sitting there.
We also know from long-term studies that [for] the vast majority of the people, eight out of ten people with that monoclonal gammopathy, it will amount to nothing. People will just live their normal life, a normal length, without it ever becoming a problem. But for the other two out of the ten, it can evolve into something that needs something to be done to it and that is often multiple myeloma.
When patients develop multiple myeloma, clearly they have damage to their body because of this abnormal group or collection of plasma cells or myeloma cells which have become cancerous. They can destroy the bone, produce high amounts of protein that get deposited in the kidneys and cause renal failure or kidney malfunction, can cause high levels of calcium, [and] can cause people to be anemic.
In some people, we can certainly identify them before these things happen or identify them at a stage where these things are very imminent and we can start treating them. But those definitions overall together [are] what you would call active myeloma or symptomatic myeloma that clearly needs treatment.
Wedged in between active myeloma and monoclonal gammopathy of undetermined significance or MGUS are people with what we call smoldering multiple myeloma. These are patients or individuals where the amount of plasma cells or proteins [has] progressed to a point where there is [a] considerable amount of those cells in the bone marrow, typically defined as more than 10% or an M protein in the blood that’s more than 3 grams.
Over time, what we have learned is these people are in between the markers and myeloma; [it] is not a distinct diagnosis, so to speak. It’s more of a collection of people who truly has more MGUS or more myeloma. We just can’t do one test and say you are more myeloma-like or you are more MGUS-like. We just have to depend on time for things to declare itself.
For at least half or two-thirds of people with smoldering myeloma, it is okay to sit and wait, but the other third may be at a higher risk of progressing. Those are the individuals [whom] we really think we could do something with the treatments we have and actually make a difference.
When we say make a difference, we mean [delaying] the time they actually get active myeloma, maybe [preventing] them from ever getting active myeloma, or maybe [curing] some of those people and we can just forget that they will ever get myeloma and not even worry about it again.
How do we identify those people? We need to be able to get to them in as precise a fashion as we can. We want to limit the number of people who might get exposed to these treatments, which may not have the same benefit [to] others.
One of the ways we do that is to use the International Myeloma Working Group criteria. Laboratory markers tell us the risk of that individual getting active myeloma in the next two years. If you think it’s more than [a] 50% chance, we feel like we need to do something about it.
There have been large phase 3 trials that have been done, which clearly show that there is a rationale for intervening in those people.
The difference between smoldering myeloma & multiple myeloma
Jack: You’re saying there is a method to determine high-risk smoldering. What’s the difference between them?
Dr. Kumar: We are talking about a stage that you may or may not have gone through. Not everybody has to be in a smoldering stage before they go from markers to myeloma, but many would have gone through the stage.
What we are trying to do here is to see [if] we can do something different for future patients, a course that is different than what you all went through.
The most critical thing that is different is, of course, whether it’s doing damage to your body — bone lesions, kidney problems, anemia, high calcium — or not. There are some individuals who may not have those characteristics, but the risk of getting that is very high: 80% plus in the next two years. Those people, we already consider as active myeloma and not smoldering anymore.
Jack: High-risk myeloma patients are more determined by mutations of certain chromosomes and things like that, right?
Dr. Kumar: That is right. When you talk about high-risk multiple myeloma or active myeloma, we’re talking about people with chromosomal abnormalities (translocations or 17p deletion), high LDH levels, or if they have stage 3 [based on] the International Staging System.
What is the ASCENT trial?
Jack: At ASH, you presented abstract 757 on the ASCENT trial for high-risk smoldering myeloma patients. What was this trial about?
Dr. Kumar: When you think about doing something different with people with high-risk smoldering, what’s our ultimate goal? We want to make sure they never get myeloma and they never have to get myeloma-type treatment that is often given continuously for long periods of time.
There are two approaches. One is obviously to give less intense treatment than what we do in myeloma and try to kind of kick the can down the road, so to speak. The other option is since we caught it so early, to see [if] we actually just get rid of it completely and maybe never even worry about it.
The former approach is what has been taken in the large phase 3 trials that the Spanish group did [and] the cooperative group in the US did. Both trials showed that people with high-risk smoldering myeloma, if you treat them with lenalidomide or lenalidomide and dexamethasone — far less intense than the three- and the four-drug combinations we use for patients with active myeloma — those interventions actually delay the progression to myeloma and, in fact, make people live longer.
What we’re really trying to do with the second approach is trying to cure the disease. There have been some trials looking: can we use more intense treatments and give it for [a] short duration to try and get rid of those myeloma cells?
The Spanish group did a trial called the CESAR trial, which was also updated at ASH [2022]. They treated people with the combination of carfilzomib, lenalidomide, and dexamethasone (myeloma-type treatment), did [a] transplant (this trial only included transplant-eligible patients), and then get them on maintenance treatments like what we would do for myeloma but give it over a defined period of three years instead of giving it continuously until [the] disease comes back.
With a longer-term follow-up [of] four-plus years, what they have seen is only five of the 81 or so patients that they enrolled have progressed to active myeloma. [For] many of those people who have progressed, the progressions have been predominantly just biochemical, meaning the M spike goes up [but] they don’t actually get myeloma.
What the ASCENT trial did was take a slightly different tact. Knowing that a significant number of people cannot go do a stem cell transplant, instead, we will do a monoclonal antibody, like daratumumab added to carfilzomib-len-dex. We use carfilzomib, lenalidomide, daratumumab, and dexamethasone for 12 cycles and then gave them maintenance for 12 cycles for daratumumab and lenalidomide. Basically, two years defined duration of treatment in patients with high-risk smoldering myeloma.
What we found was these results are quite similar to what we have seen in [a] myeloma setting. We get deep responses. Almost two-thirds of the people actually get what we call a stringent, complete response, meaning we can’t really see any protein. We can’t really see any myeloma cells under the microscope.
More importantly, nearly two-thirds of the people who got there also were minimal residual disease negative. We cannot even detect myeloma cells in the bone marrow by using highly sensitive approaches. It seems like this approach does manage to eradicate at least a significant proportion of the myeloma cells in the bone marrow.
The question that’s going to be really critical for us is: does this eradication mean that these cells will not grow back like what it does in myeloma? Only time will tell. I think both studies will continue to follow these patients over a long period of time to see if this emerging activity that we have seen is something that can be sustained over a long period of time without continued treatment.
How long until SMM patients are cured?
Jack: How long do you think you need to follow these patients before you can say these patients are cured?
Dr. Kumar: That is a good question and I don’t know if we all know the right answer to that. But the longer we can go without the disease coming back, I think the higher the probability that we may have actually eradicated this.
I’m just going to put a number out there. If in 10 years from the start of the treatment — that means eight years without any treatment — the myeloma hasn’t reared its head back up, I think I would call it successful. Obviously, each passing year is more and more of a success.
Jack: I guess we hope to see some plateau of the curve where people are no longer relapsing if you will.
Dr. Kumar: I think that is going to be the key because, in myeloma, we know that even if they get to be MRD negative, that curve never becomes flat. People continue to kind of fall off because of myeloma coming back. We’re hoping that it would be a different picture here, like what we see with some other hematological cancers like lymphoma and so forth.
Are there still trials open for high-risk smoldering patients?
Jack: At the IMF ASH symposium, Dr. Vincent Rajkumar said that treatment for all high-risk smoldering patients should either be Revlimid with or without dexamethasone or a clinical trial. Do you agree? Are there still trials open for high-risk smoldering patients?
Dr. Kumar: Yeah, I completely agree. We have to always build upon what we have learned and what we have learned in smoldering from two large trials that doing something is better than not doing anything. Giving them at least lenalidomide or lenalidomide with dexamethasone [not only] prevents the myeloma [from] coming back, [but] the Spanish trial has actually made people live longer. We owe it to our patients to have that discussion about the choices.
Ideally, if I had the option, I would definitely put everybody on clinical trials rather than using that treatment because there’s so much more to be learned. We don’t know if lenalidomide-dexamethasone is the right approach. Should we treat them like myeloma with three drugs, which is the focus of the ECOG trial?
The SMM trial is currently enrolling so that is a trial that can be considered. There’s [an] isatuximab trial that is currently accruing looking at isatuximab-len-dex versus len-dex. There [are] also multiple smaller trials in different institutions that are looking to try and see: are there specific combinations or specific drugs that might actually provide a meaningful benefit for patients with high-risk smoldering? It remains an area of active investigation so I would strongly encourage everyone to consider enrolling in clinical trials.
Asking your doctors about clinical trials (high-risk smoldering patients)
Jack: The important thing for smoldering patients is to ask their doctors: are they considered high-risk smoldering or not high-risk smoldering? If they are high-risk smoldering, they should be asking their doctor about trials. Most of these trials that you just mentioned can actually be done locally. They don’t necessarily, I think, have to be done at major cancer centers. Is that correct?
Dr. Kumar: That is right. That’s especially true for the cooperative group trial like the one we have in ECOG. It should be open in pretty much all the community cancer centers across the country.
Conclusion
Jack: Thank you so much. I’ve learned more about smoldering as well. As I said, you can always learn more about myeloma and different avenues of myeloma treatment. Any final takeaway from ASH that you want to mention?
Dr. Kumar: There’s a lot of data presented at ASH. Spanning all the way from simple questions like, “Should we be doing a bone marrow in patients with MGUS?” to obviously, “How do we treat those people or new drugs that would be potentially effective in people who have seen it all?” It’ll probably take hours to go through all that important data.
There are so many new therapies that are coming through that are so effective, especially immune therapies. We started seeing some of those being employed in the first-line treatment and the first relapse. In five years, the treatment of myeloma is going to look very different than what we are doing today.
Jack: Dr. Kumar, it’s always a pleasure talking with you and I want to thank you so much for providing your insights to The Patient Story.
Newly Diagnosed Multiple Myeloma Highlights from ASH 2022
What Newly Diagnosed Patients and Caregivers Need to Know
Multiple myeloma patient advocate Cindy Chmielewski has been living with myeloma for nearly 15 years. After experiencing excruciating back pain for two years, she was diagnosed with IgG Kappa stage 3 multiple myeloma.
In this conversation, she speaks with Dr. Caitlin Costello a hematologist-oncologist at the University of California, San Diego and Dr. Sagar Lonial, the chief medical officer at the Winship Cancer Institute at Emory University.
They discuss cutting-edge treatments and therapies for both transplant-eligible and transplant-ineligible patients, combination therapies and the necessity of stem cell transplants.
Thank you to Janssen for its support of our patient education program! The Patient Story retains full editorial control over all content.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Cindy Chmielewski, Myeloma Patient: I’ve been living with multiple myeloma since 2008. I was a fifth-grade teacher and I simply loved my job.
Around 2006, it became very difficult to teach. I was experiencing excruciating back pain. Standing was very hard, recess duty was almost impossible, and I couldn’t even take my class on a field trip. The tears would come down my cheeks. That’s how much pain I was in.
For the next two years, I was prescribed pain medication and physical therapy. I was a very different person than I am now. I grew up in [the] age of doctor knows best so I really didn’t question what my doctor was doing, although I thought that maybe we should be taking an X-ray of my back.
I was diagnosed with IgG kappa stage 3 multiple myeloma. The multiple myeloma was in over 99% of my bone marrow.
I started treatment immediately. The treatments back in 2008 were very different than now. In the beginning, I had a tough time. The treatments were not touching my myeloma. I had initial success, but then it stopped working. I had a stem cell transplant and that didn’t work. I was devastated. I really didn’t think I was going to live much longer.
A treatment that my doctor suggested began working for me. It worked so well that it put my disease into remission.
Since about 2010, I’ve been on maintenance therapy and able to live my life. In the meantime, I retired from teaching because I didn’t know what I was going to be doing.
I’m a different person now. I don’t teach fifth graders; I teach myeloma patients about myeloma and how important it is to be actively involved in your care, not to be that person like I was back in 2008 just blindly following doctor’s orders
It’s important to learn all you can about your myeloma, to ask questions, and to make decisions. It’s so exciting because now, there are so many treatments to choose from that if one thing stops working, there are so many other choices.
[In this conversation] I talk with two myeloma specialists about the latest happenings for the newly diagnosed population coming out [of] a meeting called ASH [American Society of Hematology].
Dr. Caitlin Costello is the hematologist-oncologist at the University of California, San Diego who specializes in treating multiple myeloma and participates in many of the myeloma clinical trials.
Dr. Sagar Lonial is the chief medical officer at the Winship Cancer Institute at Emory University, the chair of the hematology and medical oncology department, and a lead voice in the myeloma research community.
Transplant-eligible and transplant-ineligible patients
Cindy, TPS: Usually, newly diagnosed [patients] are broken up into two groups: transplant eligible and transplant ineligible. Before we even start talking about what’s happening in that area, how are those defined? How do you know if I’m transplant-eligible or ineligible?
Dr. Caitlin Costello: Good question and, actually, a bit of a moving target. [Transplant eligibility] is usually assigned at the time of diagnosis. A patient first gets diagnosed with multiple myeloma.
Historically, oncologists got kind of a gut instinct to say, “This patient is younger, older, healthier, less healthy, [have] a good performance status.” They’re independent [in] their activities of daily living. They can bathe themselves. They live alone. They do their own grocery shopping. Whatever it is. We’d look at a patient and say, “Healthy, not healthy, old, young,” and make generic assignments to people.
That’s really challenging to do when someone’s first diagnosed with myeloma because when you’re first diagnosed, you’re sick. You don’t feel good. You’ve spent months trying to figure out what’s going on. It may have taken a while to get the diagnosis at that point. Many bones have been affected by myeloma. It can be very painful. A lot of people just aren’t what we think normal health is.
Traditionally, we have made assignments when patients were first diagnosed to say, “You are healthy enough, strong enough, or well enough that you can get an intensive regimen called a bone marrow transplant or not.”
There’s been a bit of an evolution to the concept of transplant eligibility as some more data has emerged to say, “Does everyone have to get a transplant?” Maybe we don’t need to use those same kinds of assignments to make that determination.
I think the better way to distinguish between patients who may be able to get a transplant and patients who may not is frailty. Frailty is a little bit more of an objective, as opposed to a subjective, means of evaluating someone’s health and independence.
[It can] really help identify those patients who may be candidates for more intensive therapy throughout their myeloma diagnosis and their treatment. That is kind of where we’ve landed on transplant eligibility and ineligibility. Do we think people are well enough to undergo a bone marrow transplant?
Improving frailty in patients
Cindy, TPS: Frailty is dynamic now. It can’t be just measured at one point because, throughout the course of treatment, you may improve because the treatment is helping you out.
Dr. Costello: That’s our goal. So many patients are not well when they’re first diagnosed but can turn around pretty quickly where they perk up. Their bone pain is under control [as well as] their anemia, their kidney disease, or whatever way the disease manifested.
Treatments now are so good that patients are responding so quickly. They get better quickly. The way that your doctor first met you when you were diagnosed is unlikely the same person that they will meet two months down the road after you’ve started treatment.
Our job is to continually reassess your health and your general wellness to make that decision because what you were yesterday may not be what you are tomorrow.
Treatment for transplant-ineligible patients
Cindy, TPS: Let’s talk about that group, transplant-ineligible patients, people who may be not strong enough for their body to endure this treatment. What’s the most common type of treatment that this group of people usually get?
Dr. Costello: A bit of an evolution as well. We’ve had so many new drugs developed in multiple myeloma. When drugs get developed, they are first approved for patients who have had many prior treatments. They’re looking for the next newest and greatest.
That’s usually how the FDA approves these drugs. They approve it and say, “Let’s just start with this group of patients.” Over the years, it gets tested with more and more patients earlier on in their diagnosis.
One of the things that patients with newly diagnosed myeloma, who are not planning or not eligible or too frail to go to transplant, have enjoyed is the addition of daratumumab to the first treatment you receive when you’re diagnosed.
Daratumumab, [as] I like to describe [it], is a bit of a magnet. It’s technically called a monoclonal antibody, but it is a medicine that predominantly is given as a shot. It is particularly looking for a sign on the myeloma cells that says, “Hey, this is me.” When it finds it, like a magnet, it sticks to it.
That helps pop it open and it pops it open with many different approaches. It’s a real kind of targeted treatment and uses your immune system to help kill as well. I have seen daratumumab evolve into the gift that keeps on giving because it really has helped so many patients [at] various time points in their disease.
Now, being so effective, why wait? Why can’t we use it when patients are first diagnosed? That has really now turned into the optimal treatment as a basis for when older, frail, weak, or less healthy people are diagnosed with myeloma.
But remember, we like to use multiple drugs. I think of it as like the old game of Clue. Instead of just using a candlestick, a revolver, or a lead pipe, we want to use all the tools we have together as a cocktail so that we can approach the myeloma, sneak up on it, and kill it [in] different ways.
Daratumumab is great in combination with many different treatments. I’d say the frontrunner right now is the combination of daratumumab with lenalidomide, also known as Revlimid, plus or minus dexamethasone, which is something that we’ll get into.
What is maintenance therapy?
Cindy, TPS: Since this is a program for newly diagnosed patients, sometimes all these terms are hard to understand. Can we talk about what maintenance therapy is? Why is it important?
Dr. Sagar Lonial: That’s an important question and it gets into another important data set that was presented at ASH [2022], really focusing on [the] duration of maintenance therapy. What we know is that if you give highly effective therapy, you will get a deep response.
Many of the measures we use to evaluate how much myeloma remains are not perfect. Even MRD, which is minimal residual disease testing at one in a million or fewer, is still not necessarily a surrogate for [the] cure or elimination of the disease.
What we’ve learned is that a little bit of low-dose, non-intensive therapy can maintain that remission for a longer period of time. In randomized trials [where] patients that got no maintenance therapy versus patients that got Revlimid alone as maintenance therapy, the remission duration was at least double for the patients that got maintenance therapy.
The goals of maintenance therapy are to be low intensity and not necessarily impact [the] quality of life. While I’m aggressive about continuing maintenance as long as I can, I usually say we continue until progression or toxicity. Obviously, toxicity is an important variable in that discussion.
What we now know is that high-risk myeloma patients need more than just Revlimid as maintenance therapy. Our group, and now several other groups, have shown that a drug like Velcade added to Revlimid, or carfilzomib added to Revlimid, is able to induce deeper and more durable responses, particularly in high-risk patients. Maintenance means lower intensity, but the goal is to ultimately improve outcomes.
3 vs 2 drugs (MAIA trial)
Cindy, TPS: There were some updates in the MAIA trial at ASH [2022]. Can you tell us the latest and greatest from the MAIA trial?
Dr. Costello: The MAIA trial was designed for [the] patients that we’re talking about. They got the combination of three medicines — daratumumab, lenalidomide, and dexamethasone — and compared it to patients in that same group and only gave them two of the medicines — lenalidomide and dexamethasone.
The whole point was to understand: is three better than two? If so, how can daratumumab help improve above and beyond just the two? It was designed for patients when they were first diagnosed, not going to transplant. [They] use these treatments for as long as they are effective and as long as it’s tolerated by the patient.
It’s been a good number of years now since this trial started [and] ended. [They] are still following these patients for many years to try and see over time not only how successful it is but how durable it is.
The greatest thing and probably the most important thing we can do is [to] get people into remission the first go around. We like to say the first cut is the deepest. How can we have the most success when the myeloma is in its most kind of naive state? It doesn’t know any better. It’s not going to become resistant. We want to throw our best kind of weapons at it first.
[In] the MAIA trial, over the last many years, we’ve seen updates that come out that tell us time and time again that the three medicines combined are [an] extremely successful combination to get people into remission [and] keep them there.
The durability is because we are killing so much myeloma. The myeloma you can see above the surface [and] under the surface that’s very hard to detect. We’re just killing it all.
By making the myeloma stay away, people are living longer. We’re seeing all these outcomes and results from the MAIA trial year after year, showing that the success of these three medicines together is great because it works and it lasts.
Using 4 vs. 3 drugs for treating transplant-eligible patients
Cindy, TPS: The MAIA trial was trying to see for the ineligible patients if three is better than two. For the transplant-eligible patients, I know the question is, “Is four better than three? Should we be adding daratumumab to RVd (Revlimid, Velcade, dexamethasone)?” One thing that keeps coming up is quality of life. Can we talk about 4 vs. 3 in the newly diagnosed transplant-eligible population?
Dr. Costello: If we’ve proved three is better than two medicines together, it brings up the next natural question: is four better? That question is trying to answer if [they should be] adding daratumumab to another group of patients who have just been diagnosed with myeloma.
Let’s say that this is a younger, stronger, healthier group of people, who we have historically treated with three medicines called lenalidomide, bortezomib, and dexamethasone. For the last many years, that combination has been the mainstay. It’s been the most widely accepted, most successful treatment that we’ve been able to achieve ever. But we need to always do better.
The GRIFFIN study looked at patients who were younger, healthier, stronger, going to go to transplant, divided it in half, and said, “I’m going to give you three medicines like we always do. This is the current standard of care,” or, “I’m going to give this other half four medicines.” The same treatments that the first three got — Revlimid, Velcade, dex — and add the daratumumab to it for a group of four.
All patients got the treatment that they were assigned. All patients subsequently had a bone marrow transplant. After the transplant, all patients got consolidation and maintenance, which just means a little extra therapy after your transplant, followed by some amount of maintenance therapy, which is usually either fewer drugs or lower doses as a means of maintaining the successes you’ve had from all the treatments prior.
By comparing four drugs to three drugs for this group, again, daratumumab keeps winning. We see that daratumumab is effective at deepening response, killing more myeloma, making it get into remission more likely, [and] allowing patients to get back to themselves, to get stronger, and to continue on some amount of medicine that’s going to allow the myeloma to stay in remission in very deep ways.
Again, seeing the same outcomes we saw in MAIA, the addition of daratumumab to our standard of care allows for great successes that last.
Do you think the 4-drug combination will be the new standard of care?
Cindy, TPS: Do you think the four-drug combination is going to be the new standard of care for newly diagnosed myeloma patients?
Dr. Costello: I don’t think “will.” I’m already doing it. It’s hard to ignore the data when it’s that good. Granted, the reason I think why you’re asking is because the trial that was done was technically a phase 2 trial, where [there is] a lot of drug development and new combinations.
The people that are the most critical of statistics and evaluating successes are the ones that really want to see what we call big studies, phase 3 trials, randomized data, or you’re comparing the standard to something new and novel. Those are happening. The same drugs, the same study, more patients — it’s happening. We’ll get that information.
But on the same token, if I already have some information that shows me just how effective it is with a good number of people, I don’t want to wait. I want to do good and do well [for] these patients with these early successes that we’re seeing now. I think it’s here.
Who is eligible for quad-based therapy?
Cindy, TPS: When you’re talking about quads upfront, are we talking about all patients? How about frail, transplant-ineligible patients?
Dr. Lonial: I think it typically tends to be the transplant-eligible [patients]. If somebody is frail enough that transplant is not really an option for them, I’m a little concerned about whether you can really give them a quad.
There are some trials that are testing that right now and I’d like to see some of that data. In general, for the truly frail patient, the dara-len-dex (daratumumab, lenalidomide, and dexamethasone) combination is so good. Median remission is five years. It works regardless of age. That was evaluated in the MAIA trial.
I think that that’s a pretty good regimen and I’d like to see whether adding in bortezomib to make it four drugs really does improve not just death but [the] duration of response or lets us discontinue therapy at a certain point, which would be a huge step forward for that patient population.
Cindy, TPS: We’re talking about dara-len-dex upfront for the frail as opposed to RVd upfront. Is there a role for RVd now? Should it be a quad or dara-len-dex?
Dr. Lonial: I think there is a role for RVd in the frail patient, with weekly bortezomib in a patient that may have [a] high-risk disease. I still do believe that the proteasome inhibitor adds benefit there.
I don’t think carfilzomib is necessarily the right drug [for] a frail patient. I am still using RVd, in the beginning likely without dara, but certainly willing to add it in if I need to, if we don’t get where we want to go.
What does it mean to be high-risk?
Cindy, TPS: What do you mean by high risk?
Dr. Lonial: There are both clinical and laboratory features of high-risk myeloma that I think people should be aware of.
An elevated LDH, lactate dehydrogenase, is one evidence of that. Circulating plasma cells [are] another laboratory evidence of extramedullary disease. Genetics, meaning FISH (fluorescence in situ hybridization) testing, looking for certain high-risk genetics on the myeloma cells. Things like 17p deletion, where you’re missing p53, 4;14 translocation, 14;16 translocation. In general, those are considered high-risk features.
On the clinical side, patients that present with a lot of myeloma outside of the bone marrow, extramedullary disease if you will, tends to be high-risk disease as well. Some of these characteristics you can identify on lab tests. Some of them you can identify on exams or imaging. Those are the general rules that we use to try and evaluate risk at the time of diagnosis.
Side effects for different drug combinations
Cindy, TPS: The other thing that patients always are concerned about are side effects. Are there more side effects with the four drugs than [with] the three? What about quality of life? What are you seeing in your clinic?
Dr. Costello: The addition of daratumumab to any of these regimens, fortunately, is a reasonably well-tolerated medication. It is initially a little bit more inconvenient because of the frequency of the dosing.
This drug is given once a week for eight weeks then every two weeks for another eight times. After those first six months, it goes down to once a month, which is a very attractive option for patients. They can just come in once a month, get their blood drawn, get a shot, and get out of there. From a perspective on [the] quality of life from inconvenience, I think it’s a really nice option.
The greater side effect we think about — there’s probably two, I would say — that we’ve learned a lot in the midst of a COVID era.
One is [a] very small risk: 1 out of 10 patients with the first injection may have what we call an injection-related reaction, where patients may, kind of like a bee sting, have a variety of reactions.
Like a bee sting, you may get a little red spot, but some other people may need to have an EpiPen. With your first dose, we have to kind of stare at you a little bit [to] make sure that you’re not having those reactions. After that first administration, the likelihood of having a reaction is somewhere about 1 to 2% thereafter, so very low. The reaction risk is small but important.
The second one — and I think it’s a little bit more relevant these COVID-era days — is that multiple myeloma patients inherently have a weakened immune system. Their immune system is so busy making myeloma that it’s not making adequate amounts of your normal immunity.
If you take a drug that’s designed to kill the immune system problem, you’re going to take some innocent bystanders with it. The daratumumab is going to try and kill all those myeloma cells, but those myeloma cells are plasma cells. Plasma cells are designed to make the weapons you need to kill the bad guys, whatever it is — flu, COVID, pneumonia, whatever.
If we are taking patients who already have a somewhat weakened immune system or [are] trying to get their immune system to build back up, there is going to be some effect on the immune system that puts patients more at risk for getting infections.
It’s important to make sure we are prepared for that. Vaccinating against the handful of different things we know are important for myeloma patients, whether it’s COVID, flu, or pneumonia, and sometimes using preventative antibiotics when patients are first diagnosed.
I’m glad to say that unlike other medications that we use with myeloma that cause neuropathy where you have numbness, diarrhea, or severe fatigue — things that really can affect your day-to-day lifestyle — I don’t think daratumumab affects it as much.
The necessity of stem cell transplant (DETERMINATION trial)
Cindy, TPS: We have all these wonderful drugs that you’ve been talking about now. In the era of these novel therapies, is stem cell transplant still needed initially?
Dr. Costello: The million-dollar question. It’s ironic because it keeps getting asked. I think everyone is so hopeful that we can get rid of auto transplants because we have all these new medicines. Every time a new medicine comes out, the question is posed. A trial is done to say, “Do we still need [a] transplant or is this better?”
That’s what this trial was designed to do. It took patients who were eligible for transplant, divided them in half, and gave everybody the same medicine: our triplet combination of Revlimid, Velcade, and dex.
[Then they] said, “You get this and you go to transplant. You get this and you don’t go to transplant. Let’s see what happens between those two,” with the idea of looking at [if] one group [is] going to have their myeloma come back sooner than the other group.
The DETERMINATION study was the U.S. version of it. The French had their own version and they’re always ahead of the game with us with clinical trials. They were able to complete enrollment, get the results, [and] publish it well before we did.
They showed that patients who got [a] transplant stayed in remission longer than those who didn’t. But after looking at the data for a handful of years, what they saw was that there was no difference in how long people lived.
[There are] lots of arguments about whether that is important — and one would argue yes — [and] whether enough time had passed by to say, “Here we are. We keep applauding and patting ourselves on the back for how well these treatments are working. Maybe we haven’t had the full time pass by, enough to say that there’s going to be a great difference in survival or not.”
When the Americans did theirs, the only subtle minor difference was that after [the] transplant, patients stayed on Revlimid maintenance indefinitely, as long as the maintenance was working.
If they did not go [for a] transplant, they stayed on Revlimid as long as it was working, which was different from the French. They only took it for 12 months and then stopped.
There were a good number of people who stopped therapy and often never had progression for 6 [to] 7 years. What the American side of the trial showed was similar. The transplant group stayed in remission longer.
The survival was no different, but there did seem to be improved time to staying in remission because, we think, of the longer-lasting use of the maintenance Revlimid.
I think it begs the question: is it that we need to get rid of transplant or is it that transplant is complementary? They parsed through that data left, right, up, and down to try and understand: was it the blondes who did better, was it the African Americans who did better, or [did] someone who had different kidney function do better?
[They] tried really to see: is it a general statement we can make across the board? I think the thing that was the most helpful for me to try and parse through whether or not transplant was important or still has a role… While I would love to know that it saves lives, let me hearken back to my “the first cut is the deepest” comment.
If we are really trying to make a deep impact in myeloma when it’s first diagnosed with the presumption that that’s going to allow for the longest periods of remission until the next newest and greatest comes out, then it’s pretty clear the way they parse the data to say that those who had transplant are more likely to get to what we call MRD negativity, minimal residual disease, which is [myeloma] way under the surface.
We have lots of tricks to count myeloma. I can do a bone marrow biopsy instead of my pathologists. They look under the microscope and say, “Yep, I see it. Nope, I don’t.” But in 2023, shouldn’t we have super high-tech technology that can look for myeloma in the smallest little micron of DNA?
Dr. Costello: We want to try and get rid of every last bit of myeloma because those patients, we can tell time and time again now, are the ones who are staying in remission the longest.
The DETERMINATION study was helpful for me to say we’re not saving lives. We’re not letting people, as far as we know, live longer because of doing a transplant, but we are having patients stay in remission by doing it.
Maybe we need more time to pass by, maybe we don’t. I think for the meantime, transplant really seems to me — disclaimer, I’m a transplant-er — that it’s complementary. I think it works with our novel agents, not better or worse than our novel agents.
Dr. Costello: Maybe we can try and figure out if our initial treatments didn’t do the job, maybe that’s the group of people who should proceed. So stay tuned. Lots to come.
Dr. Lonial: I think that with the results of the DETERMINATION study, it’s pretty clear to me that even with good drugs, transplant continues to offer [a] benefit.
There are a lot of folks that say, “Well, if you’re already MRD-negative [and] it’s cycle 4, maybe you don’t need the transplant.” We actually don’t have any data that says that. My goal is to maximize the duration of that first remission because the myeloma is never more sensitive than it is at the time of the first presentation.
By the time it relapses once or twice, you may lose the ability to gain the benefit from high-dose therapy, really high-dose melphalan. Certainly, at our center, we encourage patients to go into transplant in the first remission.
IVIG and daratumumab
Cindy, TPS: What about the use of IVIG with dara? Is that being used at all?
Dr. Costello: It is. I call [IVIG] a magic trick to try and build your immunity up a bit. Whether your myeloma is not making enough of an immune system or the treatments have compromised your immune system, your IgG, which is one of your weapons to kill the bad guys, can be decreased, can be accidentally killed, [or] can [be] whatever to suppress your immune system.
If your immune system is weak because your IgG levels are low, why don’t I just give you some IgG? That’s what IVIG is: intravenous immunoglobulin. If I can give you some booster to your immune system, perhaps that will prevent some of these infections from happening.
Historically, the way IVIG has been approached is to say if someone has severe, recurrent, life-threatening infections, those patients should receive IVIG. As we’re getting more and more aware of some of these infections that can happen with a variety of different medications that are out there for multiple myeloma, I know I have become much more liberal with my IVIG use because I think it could only potentially help.
Dexamethasone
Cindy, TPS: Let’s talk about this other drug that’s been around forever. As a matter of fact, I think in ancient times it was the only drug used to treat myeloma: dexamethasone. It’s always part of every combination.
Some studies being presented show that in the frail population, after a couple [of] rounds of therapy, we can maybe start lowering or dropping dex. Can you talk a little bit about that, too?
Dr. Lonial: In my experience and those of many of my colleagues, when we use dex, particularly in older, frailer patients, we tend to use a lower dose and for a shorter duration of time.
In my mind, the maximum benefit of dexamethasone is the first four to six months. I will often start to taper after the first or second cycle to try and get to lower doses and then hope to be off between month 6 and month 12.
That approach is something that many of us are doing in general. [For] patients getting daratumumab, for instance, the label says dex before and after the dose. We only have to do that for the first two cycles at the most then you can get away with dex around daratumumab.
The same with Tylenol and Benadryl that is often used as pre-med. I know a lot of people say, “Benadryl knocks me out for the next 6 to 12 hours.” After the first few doses of dara, you don’t really need that anymore.
Some of that is just experience, knowing that that’s what we did in the early trials, and that it’s okay to do it now. If you’re not seeing somebody that sees a lot of myeloma, you may just be on a plug-and-play where everything just gets recycled from cycle to cycle without necessarily reducing or taking them off to make life easier for the patient.
Dr. Costello: Dex is clearly the drug that everyone loves to hate. I think it’s important to say that dex is an oldie but a goodie. It’s been around for a long time. It is not a chemo, but it is designed inherently to kill myeloma.
That’s an important part because patients oftentimes ask, “Well, can I just stop it?” I want to say, “Yes, but remember, consider this part of your treatment regimen also.”
It is hard. I’ve heard people say, “It’s a dex day,” and I look at the spouse or the caregiver and say, “How’s it going?” Because that can affect your quality of life more than any of the other treatments do. People plan out their lives around the days they’re taking dex or the days after their dex.
It behooves us to really understand the importance of dex for all of these regimens because if it is playing a huge role in killing myeloma, then sometimes, it’s worth it.
If we are using it for an initial period of time to make a dent in the myeloma, for example, if we can get people off dex and continue the rest of the treatment, sometimes that makes it much more manageable for everyone across the board, let alone older, frailer patients.
At ASH, we heard about a trial [that] was one of the first, if not the first, randomized trial that was done specifically for frail myeloma patients. This trial took frailer patients, divided them in half, and said, “One half, you’re going to get Revlimid and dexamethasone. The other half, we’re going to do Revlimid, but instead of the dexamethasone, we’re going to do daratumumab.”
It’s similar to the MAIA study we’ve talked about when combining daratumumab and Rev, but this time with the hope of using as little dexamethasone as possible to see if these two groups, both receiving two medicines, can have good outcomes still without using the steroid in the study arm.
Now, I’ll say that these patients did get dex for the first two cycles, I think it was. That’s important. I think dex plays a role in helping to mitigate reactions to the daratumumab. Beyond that, maybe we can get rid of it.
They compared these two groups and said, “Dara-Rev, Rev-dex, how does it go?” Again, the dara-Rev group won. It is possible, we’ve learned, to get rid of the dex on our older, frailer patients.
[It] is [likely] going to be practice changing to say if we can drop the dex as soon as possible, patients may not have the same side effects: emotional lability, water retention, feeling swollen, appetite, [and] not sleeping at night.
If it’s not going to play a huge role, it’s in the best interest of everyone to get rid of it. This was the first time we’ve seen not only for a frail group but how we can successfully get rid of dex. I think it’s practice-changing.
Cindy, TPS: My house was always the cleanest on dex stays and most organized.
Dr. Costello: It just really affects everybody in different ways, but it’s life-changing.
FasTCAR T cell therapy
Cindy, TPS: Is there anything that we did not touch upon that you think we need to share about the newly diagnosed multiple myeloma patients from ASH?
Dr. Costello: One thing I really liked from ASH [is] super exciting. I don’t know if this is here to stay. It was only 17 patients, but the FasTCAR study in the newly diagnosed myeloma.
This was a Chinese group that developed a CAR T-cell. Right now, there [are] two different CAR T-cells that are approved by the FDA for refractory myeloma for patients who’ve had more than four prior lines of therapy. Again, these are patients who had myeloma [for] a long time. They’ve had lots of treatments.
Right now, it’s not available in the U.S. for patients who are just diagnosed. The Chinese designed a CAR T-cell and have started doing clinical trials, evaluating it for someone who’s just diagnosed with multiple myeloma.
In the U.S., the CAR T-cells that we have take five [or] six weeks, sometimes longer, to manufacture. [The Chinese study] figured out how to manufacture it in one to two days. The initial results they presented at ASH showed that it worked for 100% of the people they treated and 100% of those patients were MRD negative, meaning that they cleared out every last myeloma cell.
One of the things that we are very excited about is CAR T in general, but how can we use it earlier in the disease course? This is one of the first trials we’ve seen where somebody is trying exactly that with what seems like good success. Disclaimer: it’s a very small group of people. To be determined, but exciting.
Cindy, TPS: It was exciting. I like the idea of the FasTCAR because even the FasTCAR in the relapsed/refractory setting would be helpful because too many people are waiting too long or they don’t have [the] ability to wait.
Seeing a myeloma specialist
Cynthia, TPS: This is something that patients should be asking their doctors if their doctor didn’t tell them. You’re always giving us this little pep talk that all patients at some point should go see a myeloma specialist. Can you explain that again?
Dr. Lonial: The field is moving really fast. Things [change] once, twice, three times, or 10 times a year.
We’ve had multiple drugs approved in the last four years. Even through COVID, we still saw drug approvals. I think that the field is moving fast enough that if you have a really good general oncologist, they may be able to keep up to date, but they may not know the latest and greatest.
For that reason, I think having a myeloma center of record, if you will — a place that’s close to you, a team you feel comfortable with — that can partner with your local oncologist really guarantees that you’re getting access to the latest and greatest agents or combinations [and] that your team knows what approaches are going to be the most forward-thinking approaches to keep you going for the longest period of time.
Conclusion
Cindy, TPS: We talked to Doctors Lonial and Costello about newly diagnosed myeloma patients and treatment options for them. We learned about transplant-ineligible patients and the MAIA trial. We’ve talked about transplant-eligible patients, the GRIFFIN trial, and different ways to modify treatment. We also talked about stem cell transplant and if it’s really necessary.
It’s really important to be actively involved in your care. Take some of these points of information and have discussions with your doctor to see what may be the best treatment options for you.
Special thanks again to Janssen for its support of our independent patient education content. The Patient Story retains full editorial control.
Myelofibrosis Highlights from ASH 2022: What Patients & Caregivers Need to Know
Patient advocate Ruth Fein has been living with MPN for nearly 30 years. Despite the diagnosis, she lives a very active and full life.
In this conversation, she speaks with Dr. Serge Verstovsek, founder and director of the largest MPN clinical research center in the world, and Dr. Naveen Pemmaraju, director of MD Anderson’s rare disease program and executive director of the Cancer Network.
They discuss cutting-edge treatments and therapies, combination therapy as a focus in treating myelofibrosis, and the importance of being an educated patient and being your own advocate.
Thank you to Karyopharm Therapeutics for its support of our patient education program! The Patient Story retains full editorial control over all content.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Ruth Fein, Myelofibrosis Patient: I’m an MPN patient with myelofibrosis. I’ve been living with one form or another of an MPN for nearly 30 years. When I was first diagnosed in the 90s, [it wasn’t] even called a blood disorder.
What I went through in diagnosis is very different than what’s happening today, where the initial diagnosis is that Big C, which of course is a fear I didn’t have to deal with. But now with myelofibrosis, it’s a game changer.
I’m very fortunate, as we all are, that research is moving so rapidly, changing our prognosis as the research advances. In fact, [I’ve been] on a clinical trial [for] almost three years now.
I remember it really clearly. I was in New York. It was supposed to be a routine appointment. Rain was pouring hard. I was soaking wet. I was carrying around my luggage. I sat down for my appointment with my super specialist and I’d had a bone marrow biopsy that surprised me. I had a new diagnosis. All of a sudden, I went from ET (essential thrombocythemia) to PV (polycythemia vera) to myelofibrosis, and that’s the progression people are worried about.
Immediately, I felt shocked. Then three hours later, I felt completely comfortable.
I’m seeing a super MPN specialist and she said, “I have the perfect clinical trial for you.” I got all the information [and] decided it made sense for me — that was three years ago and I am doing incredibly well.
I’m still gardening. I’m a health and science writer. I garden, I walk every day, I cycle, I swim. I’m the mother of two adult boys, a wife of a very active, wonderful man, and I happen to be a patient with myelofibrosis as opposed to my life being about myelofibrosis. My life is very full.
There’s so much we can do as patients to ensure that we’re getting the best care we can [get] to help us live longer and to live well as long as we’re here. And that’s why we have these conversations so we can bring you the expertise and the collective wisdom of the super specialists in the world.
Today, it’s all about MPN, specifically myelofibrosis. Two incredible docs are lending their insights so you can take your questions to your own doctors.
Dr. Serge Verstovsek with MD Anderson, founder and director of the largest MPN clinical research center in the world, and Dr. Naveen Pemmaraju, also with MD Anderson, who is the director of its rare disease program and executive director of the Cancer Network.
We’re having this discussion coming out of the biggest meeting of the top blood cancer and MPN specialists in the world. Our goal is to highlight what’s likely to be most impactful for those of us dealing with myelofibrosis, for both patients and caregivers.
We have some promising data on a therapy that could potentially not just address myelofibrosis symptoms but eliminate the disease for some of us. That’s very early, but it’s exciting as it was picked to be one of just a handful of highlighted sessions out of thousands at this conference that just wrapped up.
First, let’s set the stage. Most myelofibrosis patients and care partners go to a community care center. That’s, of course, where I started 20 years [ago] Even if a lot of what we’re going to talk about today is still potential or in clinical studies, what are the questions patients and caregivers should be asking?
The importance of being your own advocate
Dr. Serge Verstovsek: Thank you very much for having me. It’s a pleasure to share my excitement with you.
First, a little proactive approach is always good to learn about the condition and the disease and see how the treating doctor is about providing the answers. It’s a team effort. Nobody knows everything. Be mindful of that.
Then, if necessary, go for a second opinion [with an] MPN specialist because ideally, there would be a team — a local doctor, the MPN specialist, and the patient — who decides what to do at what time. The patient is actually in charge. We are only suggesting.
Be an advocate for yourself because it’s a lifelong condition, which has [the] potential to shorten [your] life. Engage and don’t be mad or sad. There is a lot to do together with the local doctor [and] with the MPN specialist.
Ask questions. If there are no answers, seek the answer. Be one of the contributors altogether to improve your own condition.
Be an active participant. As I always say, who is the decision maker? It’s the patient. The educated patient, engaged patient is the best patient.
Cutting-edge treatments and therapies
Ruth: Great tips, Dr. Verstovsek. You’ve been leading the way in MPN research for decades, as many of us know, and it seems there have been so many developments in terms of cutting-edge treatments and new therapies for myelofibrosis. What should patients and their partners know about that?
Dr. Verstovsek: You’re right, there is a lot going on in the MPN field. I like to divide this [between] excitement about what’s coming soon and what’s coming maybe not soon enough.
Back in 2004, when I really engaged in MPN, there was no standard of care and there was no study or studies. We were trying to seek friendly people in different companies where we would perhaps use the drugs that are already on the market for something else, like thalidomide or lenalidomide.
People probably resonate well with these drugs. We try them and other colleagues in the field try them in myelofibrosis. They do help but not too much and not too often. Then the discovery of the abnormalities — JAK2 and others — led to [a] real interest in developing more specific drugs for myelofibrosis.
Where we are now, it’s like night and day. Now, there are three approved drugs for myelofibrosis. This fourth one, momelotinib, may be [approved] next summer. So four and numerous phase 3 studies. Numerous studies in general so that you have options. We just seek more patient participation.
Ruth: Thank you, Dr. Vertsovsek. Let’s dive into what many of us know more about — JAK inhibitors. We have 3 FDA-approved ones now:
Ruxolitinib (Jakafi)
Fedratinib (Inrebic)
Pacritinib (Vonjo)
There was an update on pacritinib for myelofibrosis patients. Can you share more?
Dr. Verstovsek: [Pacritinib] is a JAK inhibitor that decreases the spleen [and] improves the quality of life.
It was approved in February 2022 for patients with low platelets, which is below 50, because it does not suppress the blood cell count like ruxolitinib or fedratinib, the other JAK inhibitors that have already been on the market for quite some time. The novelty is that it can improve anemia in some patients and that appears to be added value to it.
I actually tell my patients I treat with pacritinib — and these are the ones with the lower platelets — [and] that it’s not going to suppress your blood cell count. It may actually improve the anemia and it is good for the spleen and symptoms.
There is added value now that we know of, with [a] very [good] description of that value at ASH 2022. That’s on the recently approved drug.
Much enthusiasm is about a JAK inhibitor called momelotinib, which will be likely approved by summer 2023 because the application was submitted and it’s under review by the FDA.
This particular drug is different. It’s a pill like all the other JAK inhibitors. It may improve the symptoms and the spleen like all the other JAK inhibitors, but the real value is that anemia benefit. That is the primary reason why you would use momelotinib.
In a phase 3 randomized study that was done during COVID, it was proven to be very valuable for patients after initial ruxolitinib for control of the anemia, improving the anemia, improving the symptoms, and improving the spleen.
We expect that momelotinib, which is also very safe, will be one of the major new drugs particularly in the second-line setting once people fail ruxolitinib. All of these came from the ASH 2022 analysis. And it’s durable.
We will then have choices. We would have pacritinib for people with very low platelets or momelotinib for patients with anemia. We would optimize our care of patients for a longer period of time because we have been limited in what we could do once ruxolitinib fails.
Dr. Naveen Pemmaraju: I hope — and I know all my colleagues do, too — that we have dozens of these drugs to offer to different patients. Hopefully, one day we have a biological, molecular approach to selecting them as well.
Combination therapy to treat myelofibrosis
Ruth: Dr. Pemmaraju, let’s move to another big headline — combination therapy as a focus in treating myelofibrosis patients.
Dr. Pemmaraju: Combination therapy not only in the relapsed/refractory setting but we’re also investigating it now in the front-line setting. We have to keep in mind: how is the patient tolerating? Are there too many side effects? What is the actual benefit of adding the second agent compared to the JAK inhibitor alone?
Ruth: This always goes back to not all patients are alike. There isn’t a cookie-cutter approach. One thing I always say about MPNs and myelofibrosis is the only predictable thing is that they’re not predictable.
Dr. Pemmaraju: We always talk about personalized, individualized, targeted therapy. This is the era that we’re in now. Each patient may have a different comorbidity profile — other diseases and diagnoses that they carry outside of the myelofibrosis.
[They have] different ways they metabolize drugs [and] different molecular mutations in their myelofibrosis. We’re in a whole new era of trying to select either clinical trial drugs or, hopefully, one day, even standard-of-care drugs.
Ruth: Thank you, Dr. Pemmaraju. Let’s talk about some of these combinations. One update has been on a BCL inhibitor, navitoclax, in combination with a JAK inhibitor. Where would that come in?
Dr. Pemmaraju: This is excellent. We all work on these clinical trials together. I think the navitoclax agent, BC-LXL, is important. It’s not yet FDA-approved for anything.
What it’s showing is that in myelofibrosis in particular, either as a single agent or in combination with [a] JAK inhibitor, it has possible disease-modifying effects.
We showed very good overall survival in suboptimal patients who are already on a JAK inhibitor and added the navitoclax. Some variant allele fraction reduction, some bone marrow fibrosis improvement.
The navitoclax agent is now in phase 3 randomized global study: ruxolitinib plus navitoclax versus ruxolitinib alone essentially. We hope to have those results in [2023] so that we know if the combination approach is beneficial to our patients in the front-line, untreated setting.
Ruth: I want to talk about another phase 3 trial, a drug close to my heart: pelabresib. That’s the trial that I’ve been on for three years and that’s used again with a JAK inhibitor. I understand the results have been very promising. In fact, my doctor calls me a poster child for this clinical study.
Dr. Pemmaraju: Yeah, exactly right. In this class of combinations, we mentioned the BC-LXL strategy and navitoclax. You also have this bromodomain or BET inhibition with pelabresib.
Very encouraging results there as well, which again started out in the single-agent, relapsed/refractory setting and then was added on to the ruxolitinib and now is being investigated in patients. Again, [the] same thing: phase 3 randomized study, front-line.
For you and I that have been in the field for longer than a decade, what this marks is for the first time, we’re moving combinations into the front-line setting. That means a patient who’s newly diagnosed with myelofibrosis is then put forward with two drugs instead of one. That’s the big deal here and we’re starting to hear those results.
What should patients consider when seeking treatment?
Ruth: This is really exciting because we’re talking about options here. But if you were to say anything more as a specialist, a super specialist in myelofibrosis and other MPNs, you are seeing a patient and you’re making decisions on which way to go with therapy. What other considerations are there since you have so many options now, thankfully?
Dr. Verstovsek: There is no real reason to switch right away. If one thing doesn’t work, maybe you can optimize it. What does this mean? This means that you can combine things together.
There are a number of medications that are not JAK inhibitors that are improving the red blood cell count, the spleen, or symptoms in myelofibrosis patients [and] that can be combined. [They are] being tested in advanced clinical studies to help the patients right from day one. Day one [means] the patient needs the therapy [and is] newly diagnosed.
Why don’t we use two drugs together instead of one? There are medications like pelabresib, parsaclisib, navitoclax, or luspatercept. Basically, giving four is to enhance what the JAK inhibitors do. More of the spleen [and] symptoms control and perhaps much more durable.
Luspatercept is for anemia control while you are treating with a JAK inhibitor or ruxolitinib. One aspect of drug development [is] starting with the best combination from day one. If you start with ruxolitinib alone, you add in suboptimal responders, [which are] people who benefit but not optimally.
You add another agent later. That’s like parsaclisib, another daily pill that was proven in a presentation in ASH to be very valuable in people who are already on JAK inhibitors [and] doing okay, but there is room for improvement. You add parsaclisib on top of it, another pill, and you enhance the spleen or symptom control.
We [don’t] necessarily need to go from one drug to another drug to another drug, which is the common path, and it’s always there to do. Maybe we need to talk about combinations in specific clinical situations. We are developing multiple different combinations for different clinical scenarios.
One will be better than the other or applicable more in one patient than the other. If that doesn’t work, you go to another drug and then maybe another combination. Maybe within the next three to five years, we’ll have a number of choices not just as a single agent but the combinations.
Deciding which combination to try first
Ruth: How do you decide which combination first? I know there was data also presented [about] ruxolitinib with different agents, including novel agents such as selinexor, [which was] first approved in multiple myeloma. Now it’s being used in myelofibrosis treatment research. Can you shed some light on this?
Dr. Verstovsek: We have been studying several combinations already. I mentioned those medications, but there are newcomers, which may be better. Difficult to say from the beginning, but selinexor is another drug that is approved for multiple myeloma that may be active in myelofibrosis. It seems so from the preliminary results.
Interestingly, there was also a presentation by Dr. Kiladjian from France on adding interferon to ruxolitinib, which also enhanced the ability of ruxolitinib to do the job on the spleen and symptoms. There were some intriguing results on molecular improvements as well.
Perhaps it’s not only about combinations with a completely new, unproven yet, or completely investigational drug. Sometimes you may just look back in time and say, “Is there something there that I can use that is already established as [an] agent or a drug interferon?”
We are having a larger umbrella here without limitations in our attempts to optimize the care for our patients. It’s pretty exciting. You can have selinexor as an example. We think that’s approved for something else so much different than myeloma. You try it in a completely out-of-common-sense approach, like myelofibrosis, and it does work. We’ll follow that particular clinical study of that combination very carefully as well.
Dr. Pemmaraju: There’s this new era of novel drugs. They either come straight out of the lab or they’re borrowed from some of the other blood cancers. Selinexor is a novel one. It’s actually already US FDA-approved, for example, in multiple myeloma, but sometimes, the doses are higher or lower [or] mechanisms of action combinations.
Again, that combination, that new drug is following the same pattern we’ve seen, which is single-agent activity for relapsed/refractory and then now moving into the front line in combination with ruxolitinib, a JAK inhibitor.
Kinase inhibitors
Ruth: One other area of inhibition, if you will. You mentioned these different kinds of inhibitors. Along the way, you mentioned kinase inhibition. That’s something that could be coming over the horizon.
Dr. Pemmaraju: Yes, exactly. The third category outside of these two is what’s called PI3 kinase inhibition. Kinase, the word itself when it’s used, really means messenger or pathway in some of these cancer cells.
We didn’t have these clinical trials five [or] seven years ago. What we’re starting to do now is pick out individual pathways in the cancer myelofibrosis cell outside of JAK-STAT.
[We’re] trying to pick pathways that may complement JAK-STAT so that you can get a dual or combined approach. That’s what a lot of these phase 2 and phase 3 trials are doing and even more novel agents than these first three that we’re talking about.
Treatment, health, and transplants
Ruth: One important point here is the thought [that] transplants can be very intimidating for a lot of people. Do you feel that some of these newer therapies or combinations will help alleviate the need to go there?
Dr. Verstovsek: I think, at the moment, it’s the other way around. We are trying to improve the condition of the patients and make them physically better, metabolism to improve, inflammation to be controlled well, and get the patients to transplant in the best possible shape.
At the moment, transplant is still the only procedure that can eliminate disease and cure patients. There are limitations on the medications. We are trying hard to extend the benefit of pills, but they have limitations. Nothing really works forever.
I hope that there are actually more patients going through the transplant as we improve their condition and then the transplant success is even higher when you get the “healthier” patients.
Unless we develop the drugs, something that would potentially eliminate disease antibody in calreticulin-mutated patients. This is in the future; it’s not even in the studies yet [of anything that] has that potential. At the moment, we encourage people to go through the transplant when they are in the best possible shape on a JAK inhibitor.
Dr. Pemmaraju: Allogeneic stem cell transplant remains the only curative modality for our patients with myelofibrosis. It’s tough to say that because it’s such a difficult procedure for many of our patients. Many of our patients are older [or have] comorbidities.
Across the world, as I meet with patients and doctors, they don’t have access [to] or follow-up for it. That’s tough. That’s the hope and optimism that I personally have: can we offer these combinations or other novel agents to try to cure the disease outside of stem cell treatment?
Unfortunately, I would say stem cell transplant is the only curative option, but again, unfortunately, it’s not available to the vast majority of our patients.
Ruth: Speaking of cure, that is the big splash that just came out of this ASH meeting. Dr. Verstovsek, what was all that buzz about?
Dr. Verstovsek: It has to do with the development of a possible new therapy. The key word is “possible” because the presentation was on preclinical testing. [It’s a] possible new therapy for a third of the patients with myelofibrosis or ET (essential thrombocythemia) that have a specific mutation: calreticulin mutation.
Everybody probably knows about the JAK2 mutation, but there are a couple of other mutations that are important that are mutually exclusive. You have JAK2 mutation, calreticulin mutation, [and] MPL mutation. These are mutually exclusive and present in about 90% of the patients with myelofibrosis and 90% of patients with ET (essential thrombocytopenia).
What they do is activate inside the bone marrow cell this pathway that we call a cascade of protein. My patients call it a highway. It jacks that highway. It’s always active because of these driver mutations. That makes your cells grow and causes inflammation.
Because this mutated protein is on the surface of the cells, we can identify malignant cells. This is a marker of [a] malignant cell. Now, the presentation was on [the] development of [an] antibody. Another construct would be attaching specifically to the cell with the mutated calreticulin and basically [letting] it die off over time, so elimination of the disease.
This is a potential of such a therapy, [an] antibody for mutated calreticulin, which will be given to patients with myelofibrosis or ET that have calreticulin mutation by genetic testing. It’s easy to do and that’s the potential of inhibiting the growth of malignant cells specifically. Elimination of the malignant ones is what everybody is talking about.
We hope that in the near future, perhaps [in] 2023, we’ll have a study of it with the antibody for patients with calreticulin mutation. Extremely exciting because we usually talk about improvement in the bone marrow function — anemia needs to improve, decrease in symptoms, or smaller spleen. This has a potential [for] what we call molecular response — decreasing the number or eliminating potentially the malignant cells.
Ruth: That is exciting! To be clear, this calreticulin-targeting therapy is not in [a] clinical trial yet, so the hope would be for it to enter a phase 1, first in humans, study hopefully this year.
Speaking of clinical trials, I’m a part of one now. You’re trying to get more people to know about and ultimately participate in clinical trials, too?
Dr. Verstovsek: Participation in the study would be the ultimate goal in my view from the patient’s perspective. You get the standard, but you get something extra on top to make it even better. Why not?
From your own perspective and from the perspective of benefit to the community of MPN patients, why not seek participation in a clinical study if it’s not mentioned already by the treating doctor?
Importance of being an educated patient
Ruth: That’s exciting because it helps people understand the importance of where all cancer therapies are hopefully heading into with understanding more data about the person. In this case, the mutation.
What is your message to patients and their care partners [or] caregivers about the importance of making sure they understand or [are] asking questions of their doctors about mutations?
Dr. Verstovsek: The best patient is [an] educated patient. In our own practice, we try to provide the patients [with] everything we know about their condition unless the patient says, “No, no, no, you are the doctor. Don’t tell me anything,” which is not very common.
We have a very enthusiastic group of patients that would like to know everything and be part of decision-making and planning, which is the optimal care in my view. We embrace everybody and we want everybody to participate and understand.
The disease is there for some reason. We cannot really say, “This is why it happened,” but we can describe it very well by molecular testing, the testing of chromosomes, the testing for fibrosis grade in the bone marrow, and as you measure the spleen and the red blood cells.
You want to know everything you can. Sometimes, that information is useful for therapeutic decision-making; sometimes, it’s not. Patient education and understanding of what it is, what can we do about it, and how is very important.
Calreticulin mutation in the future — some reservations here — can potentially really make a difference for these patients. We’ll see.
Conclusion
Ruth: It seems that two things are going on. One is medical science is moving forward. Personalized medicine is the name of the game and patients need to have an active dialogue with their doctor as to where they are now with their myelofibrosis and what applies, either in a trial or with an approved or newly approved medicine, right?
Dr. Pemmaraju: You could not have said that better. I really want to emphasize what you said because we are now beyond the point where we only had one treatment option or one standard-of-care option. That’s awesome.
Dr. Verstovsek: I always try to emphasize to our colleagues in the field and the patients themselves who are savvy and go online that there is so much going on. Get engaged. Standard care came to become [the] standard of care from research. It didn’t just appear.
The combination [and] new drugs that are in development, potentially better than the standard of care, are subject to research. That’s how you do it. We are here to team up with the companies, with the regulators, and with the patients all together for [the] betterment of therapy for myelofibrosis. Be alert. A lot is going on. Be a participant.
Ruth: Thank you both, Dr. Verstovsek and Dr. Pemmaraju, for joining us in this conversation to help us, myelofibrosis patients and care partners.
Dr. Pemmaraju: Thank you so much and thanks for having me.
Dr. Verstovsek: My pleasure. I hope it was useful to everybody. I’m here to help.
Ruth: Thank you to the patients and loved ones who are so engaged in understanding more. There is a lot to be hopeful for.
Special thanks again to Karyopharm Therapeutics for its support of our independent patient education content. The Patient Story retains full editorial control.
Relapsed/Refractory Multiple Myeloma Highlights from ASH 2022
The Role of Bispecifics in the Treatment of Relapsed/Refractory Multiple Myeloma
Patient advocate Jack Aiello is a 28-year survivor of multiple myeloma. When he was diagnosed, he was told he would only have two to three years to live and only two treatment options were available.
Jack underwent two transplants and then went onto a clinical trial for thalidomide but nothing worked until a third transplant.
In this conversation, he speaks with Dr. Ajai Chari, the Director of Clinical Research at the Multiple Myeloma Program at Mount Sinai in New York and Dr. Sandy Wong, a blood disease specialist at University of California, San Francisco, with a special interest in multiple myeloma.
They discuss game-changing treatments for relapsed/refractory patients, bispecific antibodies, treatment side effects, and emerging clinical trials.
Thank you to Janssen Oncology & AbbVie for their support of our patient education program! The Patient Story retains full editorial control over all content.
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
For today’s newly diagnosed patient, you can be more optimistic about your diagnosis than [at] any time in history. We don’t have a cure [but] we have treatments available to manage this disease.
Jack Aiello
Introduction
Jack Aiello: I’m a 28-year survivor of multiple myeloma. When I was diagnosed in 1995, the doctor told me I had two to three years to live and [that] there were only two treatment options available. I remember going home to my wife, [telling] her the little bit I understood about this disease, and, suffice it to say, we shared a good cry.
I had kids who were 16, 14, and 10 years old at the time. I knew I was going to have to go to the hospital so I just told them that there was something wrong with my blood and I was going to have to have it treated. But I wondered, would I be seeing the kids graduate from high school? Who was going to teach my son to hit a curveball in Little League? Who was going to pay for them [to go] to college? It was a difficult time.
Since then, we’ve had 13 or 14 new drugs approved by the FDA, more combinations of these drugs, and even more are in clinical trials today.
I really believe that for today’s newly diagnosed patient, you can be more optimistic about your diagnosis than [at] any time in history. We don’t have a cure [but] we have treatments available to manage this disease.
For relapse/refractory patients, you’ll hear some great results from the recent ASH meeting. Many abstract presentations were on the topic of drugs and a category of drugs called bispecific antibodies.
To help us understand more are Drs. Ajai Chari and Dr. Sandy Wong.
Dr. Ajai Chari is the Director of Clinical Research at the Multiple Myeloma Program at Mount Sinai in New York.
Let’s kick off the conversation with what was the big buzz this year: bispecific antibodies. We’ve heard of monoclonal antibodies like daratumumab. Most recently, the FDA approved a bispecific antibody called teclistamab or Tecvayli. What exactly is a bispecific?
Bispecific antibodies
Dr. Ajai Chari: It’s a really exciting time. I’ll start with one of my favorite stories about the development of immunologic treatments in all humans. In [the] 1980s, the Nobel Prize was actually given for creating a standard antibody that was taken by fusing a myeloma cell with a spleen cell.
Every human antibody that we use — whether it’s for COVID, autoimmune diseases, [or] cancers — owes its legacy to myeloma. The first naked antibody, which is this Y-shaped structure, was not approved [for] myeloma until about 30 years after that Nobel Prize was given even though antibodies were helping everybody else.
The first naked antibodies were daratumumab and elotuzumab. The ends of the Y-shape bind to one target and typically that’s the myeloma cell or whatever cancer cell.
It’s either a handcuff or double-sided tape. Basically, what it does is it takes one side of the Y, binds to a T-cell through a target known as CD3, and the other side can bind to a myeloma cell. You can change that up based on the protein.
The one that’s commercially available now that’s called teclistamab binds CD3 and the T-cells to BCMA or B-cell maturation antigen.
It’s remarkable how well these agents are working.
Dr. Ajai Chari
Jack: So the difference between that and a monoclonal antibody is the monoclonal antibody doesn’t have that second arm connecting to the T cell, is that correct?
Dr. Sandy Wong: That’s correct. Monoclonal antibodies activate the immune system in a different way.
For example, drugs like daratumumab or isatuximab activate the immune system [in] several ways. One is they act almost like Post-It Notes, if you will, where they flag cells [that] are not supposed to be there, i.e. the myeloma cells, and that leaves the immune system to know, “Hey, this is not supposed to be there. Let’s get rid of this myeloma cell.” That’s how a monoclonal antibody works.
Bispecific T-cell engagers physically attach to T cells and bring the T cells in physical proximity with the myeloma cells. The T cells get rid of myeloma cells that [are] not supposed to be there so they secrete their toxins, etc., and get rid of the myeloma cells. They work very differently.
Dr. Chari: It’s remarkable how well these agents are working. Basically, it’s an off-the-shelf product so that’s important.
A lot of people may have heard about CAR Ts that also target BCMA, but the difference is this is ready to go. It doesn’t have to be manufactured for each patient.
You don’t need to go through the T cell collection, manufacturing, and waiting. This is an off-the-shelf product. That’s the same for every patient with myeloma.
What the drugs do is basically traffic the T cells in our bodies to whatever you’re trying to bring them to. In this case, the T cells in a patient are preexisting or trafficked to wherever the myeloma is, and when the T-cells are brought right up against the cancer, they recognize the cancer.
They release certain chemicals or cytokines that poke holes in the cancer cell and that lead to cell death. I say it’s like bringing your army straight to the enemy, as opposed to hoping and praying that they find the right place to go.
It’s a mind-changing, game-changing era that we’re in with this immunotherapy treatment.
Dr. Chari
Treatment for relapsed/refractory patients
Jack: The teclistamab that was just approved and the other bispecifics, just to let the [readers] know, are so far for relapsed/refractory patients. Those [are] patients who have gone through several lines of previous treatments before getting to these bispecifics. Is that right?
Dr. Chari: Yeah, that’s exactly right. Just to put this whole space into context, about five [or] six years ago, the way drugs get approved is that they’re first tested in heavily treated patients — as you mentioned, relapsed/refractory myeloma.
The benchmark to get a new drug approved was about [a] 20-30% response rate, lasting about three to four months. Those numbers sound modest, but we have to keep in mind those are in patients who had exhausted all available therapies.
When I started in myeloma 17 years ago, thalidomide was just coming on the scene. At that point, [to treat] relapsed/refractory, you had thalidomide and maybe a transplant. Now, typically, we’re talking about the big five drugs:
lenalidomide (Revlimid)
pomalidomide (Pomalyst)
bortezomib (Velcade)
carfilzomib (Kyprolis)
CD38 antibodies, such as daratumumab or isatuximab
That is a very different patient than somebody who just had had thalidomide. As we keep approving drugs, this unmet need, which is patients who have exhausted their currently available therapies, keeps changing.
In spite of that, what’s remarkable about the entire T cell redirection, whether it’s bispecific or CAR T, is we’re saying 70-100% [response rate] is the new 20-30%. That’s how many patients are responding to these drugs. Even though these are much, much sicker patients and have had more treatments [and] more drugs, we’re getting better responses.
That’s what’s really exciting. I literally have patients [with] whom we had discussed hospice a few years ago and now they’re in their deepest, longest remission they’ve had in years. It’s a mind-changing, game-changing era that we’re in with this immunotherapy treatment.
How is talquetamab is different from other bispecifics?
Jack: For one who’s been watching new treatments being developed and now seeing [a] 60% or 70% response rate, it’s pretty incredible.
Dr. Chari, you presented a different bispecific called talquetamab, also from Janssen, the same manufacturer of teclistamab. Can you share the results of this trial and what might make talquetamab different from other bispecifics?
Dr. Chari: First of all, this work takes [a] tremendous team, starting with the patients and their caregivers and then the entire study team, Janssen, the pharmaceutical, the FDA, and other regulatory agencies.
With the phase 1 portion of the study, we’re looking to just find the safety and what’s the right dose and schedule. The phase 1 study just got published in [the] New England Journal so that was very exciting. It was also a large phase 1 study with over 200 patients.
Efficacy and safety (how well it works in the safety profile) were then validated in this phase 2 study and that’s what we presented at ASH [2022]. The phase 2 study had 3 major cohorts of patients:
One got a dose of what we call 0.4 mg per kg subcutaneously every week
A second cohort got 0.8 mg per kg every two weeks
The third cohort could have gotten either one of those doses, but [in] a very important subgroup of patients who already had prior T cell redirection therapy, meaning patients who had had other CAR Ts and bispecifics
Even though these are 60-100% response rates, we’re still seeing relapses so you still need new agents. The goal of this study was to really look at these three subgroups. I would start with who these patients were. These were patients with heavily-treated disease.
About 60% were high-risk in some way, which is a very high number. That could be defined either by what we call high-risk genetics, so cytogenetics and FISH; high risk because they had myeloma coming out of the marrow, what we call extramedullary disease; or high risk because they had so-called ISS stage 3 disease at the time of study entry.
In this population, with the typical five to six lines of therapy over six to seven years where almost 95% of patients were refractory to daratumumab, 75% were what we call triple-class refractory (proteasome inhibitor, IMiD, and CD38) and 95% of patients were progressing on their last therapy.
In this heavily, heavily treated group, as a single agent drug, we saw [a] 73-74% response rate in both of those schedules that we mentioned. That response rate was maintained in high-risk patients, ISS 3 patients, and patients regardless of lines of therapy, regardless of the number of drugs they were refractory [to].
One group who had [a] slightly lower response rate was those with extramedullary disease and even those had a 50% response rate, which I think is outstanding. I think safety is also equally important and distinguishes this from some of the other drugs.
What makes alnuctamab different from other bispecifics?
Jack: Dr. Wong, you presented on a bispecific called alnuctamab from Bristol Myers Squibb. Can you share the results of this trial and what might make alnuctamab different from other bispecifics?
Dr. Wong: We presented both the updated follow-up on the intravenous alnuctamab cohort as well as the subcutaneous alnuctamab cohort. The intravenous cohort was actually presented initially in ASH 2019 so there’s been quite some time that’s elapsed.
Basically, the take-home message with the IV alnuctamab was that even though the response rates initially looked exciting, when we got to target doses of 10 mg, there was a lot of high-grade cytokine release syndrome. People got really sick from CRS and one person actually died from it so it was not really optimal in terms of the side effects. Obviously, we don’t want people to get sick from these treatments.
Patients that were on the intravenous alnuctamab responded for a really long time so we’re really, really excited about that. However, we had to pivot to the subcutaneous alnuctamab because of those safety concerns. With the subcutaneous alnuctamab, the overall response rate was at 65%, which is very much in line with other T-cell engagers.
In terms of safety, all the CRS events were very low-grade. They were short-lived. They’re what we call grades 1 to 2 and, in terms of safety profile, it was a lot more manageable compared to intravenous alnuctamab.
That was what was really exciting about our presentation. Not only is subcutaneous obviously more convenient for patients, but the CRS events were much easier to handle and the overall response rate was 65%.
How does this stand out from the other T cell engagers? Several things. This is not the only subcutaneous BCMA-directed T cell engager, but there are some that are intravenous. For example, ABBV-383 is intravenous. So this is great that this is subcutaneous.
It’s hard to compare apples to oranges because all these different BCMA-directed T cell engagers have different follow-up time frames. For this one, the follow-up was very, very short. The median [was] only around four months.
In terms of infectious events, in terms of opportunistic infections, we really haven’t seen much of that for this particular drug so maybe that eventually will pan out longer follow-up studies but unclear because follow-up is pretty short.
What is really exciting is that the MRD negativity was 80% despite these patients [not being] followed for that long. That is actually really exciting. We don’t have a signal for these high-grade infections or opportunistic infections though. Again, follow-up is pretty short with this drug.
What are common side effects for bispecifics?
Jack: Speaking of infections, what are the common side effects we’re seeing with bispecifics altogether? I understand some research is unearthing data about how myeloma patients on certain drugs do with COVID and the vaccine.
Dr. Chari: I’ll start with what’s the most severe toxicity and then we’ll go to what’s common because I think they’re different and they’re both equally important to address. From a patient perspective, if it’s severe but rare, you may not be as concerned, but if it’s common and frequent, that’s different.
The most severe side effect is low blood counts. We see that in about a third of patients with this drug. Typically, it happens in the first few cycles.
My personal hypothesis, I think what’s happening is when the army is going to the marrow where a lot of myeloma lives, you kill the myeloma but you may temporarily also affect the rest of the marrow. Then once the myeloma clears, you see that [improvement].
Jack: Patients may hear that called cytopenia. Is that correct?
Dr. Chari: Correct. That’s exactly right. It could be the white cells, the red cells, or the platelets. Those are important. This is already a little bit less than some of the other drugs, which can have as high as 60%. This is about half of that.
The second huge thing, which you alluded to and it’s very important, is the infection. I can tell you, being in New York City [during] the pandemic, this was really a difficult situation. We had patients on experimental therapies and we were facing these life-threatening COVID decisions every day. We didn’t know what to do with this setting.
I think the infection profile of talquetamab is very unique. I’ll give you three ways why I think it differs from some of the other products.
First, the rate of severe infections was about 10-15%. We want it to be zero, but to put that into context, some of the other drugs are 45%.
We’re not just talking [about] minor infections, which can be seen with any myeloma patient because of the nature of the disease. [These are] severe, life-threatening infections, what we call grade 3-4. That was relatively modest.
Second, the COVID signal is very different with this agent. Talquetamab as well as a lot of the other bispecifics are all accruing during the era of COVID. Yet in the phase 1 study that was published in [the] New England Journal with about 250 patients, there were zero COVID-related deaths.
In this study, there were two COVID-related deaths despite 10% of the patients having COVID. That’s a unique signal. In fact, in our laboratory at Mount Sinai, when we’ve tested people getting talquetamab [and] their response to the COVID vaccine, they do very well. They’re able to generate antibodies, which we don’t see with some of the other bispecifics because of the nature, I believe, of the target.
The third and final difference between this drug and some of the other bispecifics is the need for infection-prevention treatments. Is there anything we can do to reduce infection? There is IVIG, which is intravenous immunoglobulin, that’s an intravenous infusion given once a month to boost IgG levels. Here, only about 10% of patients needed IVIG.
All of those features of this drug are very unique. Some of the other products are having as high [a] rate [as] 40% of patients needing IVIG. I think this bodes well because these are probably the two most important features, which [are] cytopenia, blood count, and infections in terms of how these drugs are used in the future.
The ability to combine drugs depends on each agent’s side effect profile. Because infections and blood count issues are quite common, that can make some of these bispecifics difficult to combine. I think, in contrast, that bodes well for talquetamab.
There are some issues with talquetamab that are common but typically low-grade. One you’ve alluded to is cytokine release.
I would say as a class, all the bispecifics have cytokine release syndrome on the order of 70% or so, typically low-grade. In contrast, some of the CAR Ts have a little bit higher, more severe cytokine release.
What is cytokine release? It’s when the army recognizes the cancer. The T cells release their chemicals and those chemicals can cause symptoms such as fever, low blood pressure, low oxygen, confusion, lethargy, seizures, and even death, in rare cases. With bispecifics, it’s generally very low-grade. Most of the patients are getting a fever.
Everybody eventually would love to be able to use these drugs [in] an outpatient setting… If we’re able to do this safely as an outpatient, that would be really a big game changer for patients and their quality of [life].
Dr. Sandy Wong
Lowering cytokine release syndrome with treatments
Jack: There’s a big focus on lowering cytokine release syndrome with treatments like bispecifics. In particular, I saw one trial which looked at trying to reduce CRS by giving tocilizumab ahead of time. I’ve seen things like step-up dosing to reduce side effects. I know doctors have asked for possible pre-treatments for reducing infections. Can you share more about this?
Dr. Wong: Everybody eventually would love to be able to use these drugs [in] an outpatient setting. Nobody wants to be admitted to the hospital for a week just to get started on these drugs. If we’re able to do this safely as an outpatient, that would be really a big game changer for patients and their quality of [life].
Dr. Chari: We have to keep in mind one of the very things that’s going to make bispecifics different than CAR T.
CAR Ts are done at transplant centers and specialized large academic centers. These are off-the-shelf products that we hope eventually can get to the community because we recognize that most myeloma patients are not being treated in the global setting and academic centers. They’re being treated by community doctors.
If we want to get these drugs out to the community, we have to make them as safe as possible. How do we reduce that 70% cytokine release? One is by giving tocilizumab. In one of the studies with a bispecific known as cevostamab, [the] rate of cytokine release dropped from 70-80% to about 30%. That’s very encouraging.
The other way to do that, which you mentioned, is don’t throw the whole army at the disease at once. Gradually increase the doses so that if there is some chemical release, it’s not all at once. That creates a lot of drama. You start with a low dose and you gradually work your way up.
Both strategies are being done. With talquetamab, we did do preventative tocilizumab, which is the anti-IL-6 antibody, which blocks the fever. We were allowed to give it when patients had cytokine release, but we didn’t give it preventatively, which is what was presented at ASH [2022] in that one study.
The other side effects [of] this drug are three things. One could ask, “Why is this one different than other drugs in terms of why potentially the infection was better? Why were the blood count issues perhaps not as bad?” We think it has to do with the target.
The target is GPRC5D, which is basically a protein that is expressed on myeloma cells primarily. We think [it’s expressed] less so [in] normal plasma cells and even less so in the normal hematopoietic compartment, which is the precursor cells that give rise to our blood counts.
Perhaps the specificity of this protein is what underlies the favorable blood count and cytopenia issues, as well as the infection profile. There are a few tissues that do express GPRC5D and, fortunately, it’s not the major organs. We didn’t see [the] heart, lung, liver, [and] kidney. Those organs were not affected.
The main thing we did see is GPRCs expressed on heavily keratinized tissue. Keratin [is] in the skin, nails, hair, etc. We didn’t see a lot of hair loss, but we did see some rashes in the early part of the treatment, which [is] typically managed with either oral or topical steroids.
We did see some nail changes and taste changes. We saw dryness, difficulty swallowing, [and] change of taste. That, I think, is the most difficult to manage. We’ve tried artificial saliva and other things.
In spite of everything, the one signal that you can look at to see the tolerability of a drug is how many people came off for non-progression. This was 5%, which means that we were able to manage the side effects to keep people on the drug. I still think we need to do better.
We have to keep in mind that the side effect profile that a heavily treated population might accept is going to be different than the side effect profile of maybe somebody who’s only had one line of therapy.
The good news is that we do think these side effects are responsive to modulating the dose and intensity, so either dropping the dose or skipping a dose, giving it less frequently. Those seem to help. I think that’s why the rate of discontinuation was relatively low.
Again, a huge shout-out to the nurses because they’re really on the front lines and helping patients deal with these side effects. I never take my entire outstanding, talented nursing colleagues for granted. They’re really doing an amazing job. Those are basically, I think, the main side effects to cover with talquetamab as well as most bispecifics, I would say.
We have to keep in mind that the side effect profile that a heavily treated population might accept is going to be different than the side effect profile of maybe somebody who’s only had one line of therapy.
Dr. Chari
Managing side effects for bispecifics
Jack: Let’s summarize the side effect profiles for these bispecifics. I would stay on bispecifics typically until they stop working. I take them every two or three weeks, depending on how they’re dosed. Do these side effects change? Are they worse at the beginning? Whatever side effect I get at the beginning, [does it] continue as I’m taking the drug?
Dr. Chari: There [are] three major bispecific targets that are being explored. We’ve talked about GPRC5D with talquetamab. There’s actually a second company also pursuing that. That was also presented at ASH [2022] from Roche, targeting GPRC5D.
The BCMA is a very busy space. I think it’s like the statins of myeloma, like Crestor [and] Lipitor. It’s great for patients because more competition means more choice [and a] better cost profile. I think it’s great for the market.
I would say the BCMAs seem to keep having a rate of infection that we don’t see a plateau in. That’s what’s concerning to a lot of us. How do we find the right dose, schedule, and duration?
It’s one thing to have an infection in somebody whose myeloma is uncontrolled because that we’ve seen before. Myeloma patients whose myeloma is uncontrolled will get infections because that’s part of the cancer.
What can be sometimes difficult to tease apart in these single-arm studies is you can’t isolate what’s coming from the patients (like if the patient is a very sick patient), what’s coming from the disease of the myeloma itself, and what’s coming from the treatment because you don’t have a control arm in which to compare it to.
One of the things, as your question astutely asked, is there any change? With the infections, we’re not seeing that level off with the BCMA. With talquetamab, we’re not seeing it as much.
I would say with the cevostamab, it’s probably somewhere in between. That’s targeting another protein called FcRH5. I would say [with] infections, we haven’t found the right magic sauce yet. Perhaps IVIG.
One other interesting paper that I think speaks to this topic is Genentech/Roche, the same company that did the prophylactic or preventative toci (tocilizumab) also happens to have the only bispecific that is a fixed duration. They don’t treat the progression. They treat for about a year.
What we saw is there’s a small number, but about 17 patients that had come off the therapy and were in longer follow-up on that study. What we know so far is of the patients that had a deep remission, they’ve been doing pretty well off therapy. Again, [that’s] amazing for patients to have a treatment-free interval.
With talquetamab, we’re not seeing that relentless increase in infection — and to the opposite, the side effects [with] skin, nails, and taste actually seem to get better with time. There may not be as much of a need to do the fixed duration there. Maybe it’s once-a-month dosing or something.
We’re pursuing all of these different strategies, but I would say that we’ve got to look at everything. We’ve got to look at the dose, the frequency, [and] the duration of treatment and figure [it] out for a given patient, based on a given target and on their response.
That cevostamab data, which [was] discontinued for those patients that were not in a complete response, did have [an] earlier relapse.
I think you can’t have a blanket statement. You just got to look at each patient as an individual. It’s nice to have these options that are giving such outstanding responses.
Bispecifics are here. It’s a dawn of a new era… We have multiple drugs against multiple targets that are showing impressive response rates.
Dr. Wong
Next steps for research
Jack: Thank you so much. I’ve learned a lot about bispecifics. I can also tell there’s still a lot of work to do to understand the dosing, to understand if there will be prophylactics that go along with them to minimize those side effects, to see if fixed duration or use till progression will be the right treatment, or just to reduce the dosing going forward.
I still go back to what you said earlier that we’re seeing response rates so high for just this drug, not even combined with something else, and for patients that have already gone through lots of prior treatment lines. It’s certainly an exciting field.
Dr. Chari: Not only are we seeing these responses, [but] the median time to response is one month and the median time to best response is two months. I mentioned those points because it gives us, as physicians, a lot more comfort in backing off on the dose and schedule.
You’re seeing the response early and it’s deep. If somebody has side effects, you’re not as worried about backing off. That’s what’s really nice about these drugs. Even if somebody does have side effects, it’s very gratifying to them to have this myeloma that was shooting off and suddenly it’s completely flattened out. That’s why I think the side effect profile we’ve got to do more work on.
What are the next steps? All the phase 1 and phase 2 single-arm studies have confirmatory randomized studies where the drug’s being combined with different backbone agents.
Also, because of the unique side effect profile, talquetamab in particular is also being combined with all those standard myeloma drugs in single-arm studies as well as with the other bispecific, which is really cool. Completely chemo-free teclistamab with talquetamab is being studied.
Lastly, we’re trying to also improve the T cell function because we think one of the reasons the drugs may peter out is because of T cell health. There [are] approaches using things like checkpoint inhibitors, which boost your T-cell function, in combination with these agents.
Bispecifics are going to be a fabulous treatment option for myeloma patients… I’m excited to see what comes next in myeloma.
Jack
Final takeaways
Jack: Doctors, as we wrap up this discussion on the latest in myeloma, specifically bispecifics, what are your thoughts on where we are in myeloma treatment and research? What’s your message to myeloma patients and families in 2023?
Dr. Wong: Bispecifics are here. It’s a dawn of a new era because finally, we have [an] off-the-shelf drug, which means that you can just take it right off the shelf and just give it to a patient. And for an off-the-shelf drug to have a response rate of 60 to 70%? That is absolutely amazing.
Previous to this, dara (daratumumab) was our darling drug. We use it so common nowadays in the front-line setting and the relapse setting. When dara was FDA-approved, the single-agent response rate in patients who are relapsed/refractory was only around 30%. Right now, we’re hitting 60 to 70% so this is extraordinary.
And it’s not just one drug. We have multiple drugs against multiple targets that are showing impressive response rates. I think really good news this ASH. I’m really excited to see all that amazing data being presented.
Dr. Chari: I think it’s a really exciting future. We’re just in the beginning and, of course, in less heavily treated patients, it’s also a big area of investigation in addition to combination. Stay tuned for all of those exciting new studies, hopefully soon.
Jack: Bispecifics are going to be a fabulous treatment option for myeloma patients. Thank you so much, Dr. Chari and Dr. Wong, for your presentations, [for] helping us better understand bispecifics, and [for] being part of this conversation.
I hope you took away something helpful and hopeful from this conversation. I’m excited to see what comes next in myeloma.
Special thanks again to Janssen Oncology & AbbVie for their support of our independent patient education content. The Patient Story retains full editorial control.
The Patient Story founder and DLBCL advocate Stephanie Chuang leads this conversation with Dr. Josh Brody, who leads the Lymphoma Immunotherapy Program at Mount Sinai’s Tisch Cancer Institute, and Dr. Lorenzo Falchi, an oncologist at Memorial Sloan Kettering Cancer Center with special research focus on immunotherapies for B-cell non-Hodgkin lymphoma.
Thank you to Genmab for its support of our patient education program! The Patient Story retains full editorial control over all content.
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Stephanie Chuang, The Patient Story: I was diagnosed with cancer when I was 31 years old and, like many people, I was completely overwhelmed [and] freaked out. I thought, Am I going to die? I think that’s a pretty common thing to think when you’ve been diagnosed with cancer. I was really thankful to learn that there was a standard of care treatment in chemotherapy that seemed to have a pretty good impact on cancer and DLBCL.
I underwent dose-adjusted R-EPOCH — a little bit different from the usual R-CHOP. I remember my doctor telling me, “Look, Stephanie, if you can hit two years after treatment is done and the cancer is gone, you’re still in remission. That’s a really good sign.”
It’s great news that I was able to get through treatment and get into remission. But that wait was really hard. Lots of anxiety and scanxiety as it’s known. I was able to hit two years and, in fact, most recently I celebrated my five years. But so many people cannot say that.
That’s where the problem is. There’s a really great need for more options in treatment. If that first treatment fails, when cancer comes back or if it never responded, [relapsed/refractory cancer] and that’s what we’re talking about.
What are the treatments out there? What are the options? What should you know to ask your doctor in terms of the research that’s going on out there?
There’s good news. There [are] a lot of different things happening in clinical trials, whether it’s new drugs or new combinations, new tactics, and a lot of immunotherapy using your own immune system to fight cancer.
I’m really excited to bring together two top DLBCL specialists and, hopefully, shed some light for you, especially during what is a very difficult time.
There’s a lot of new information and updates coming out of the biggest meeting of top blood cancer doctors and researchers called ASH or [the] American Society of Hematology, which just took place.
Dr. Brody, a lot of people wonder — I certainly did when I was diagnosed — why me? What did I do to get this? This is something you hear a lot from your patients as well.
There’s nothing you did. You got this for the same reason that people get hit by lightning. Nothing that they did.
Dr. Brody
Dr. Josh Brody: In the very beginning, when patients get diagnosed, a lot of questions [are] coming out of a place of fear, [which is] very natural and understandable. How did I get this? What did I do? As though someone wants to blame themselves for this. I guess it’s natural.
Our first thing is to go and say, “There’s nothing you did. You got this for the same reason that people get hit by lightning. Nothing that they did. You got this, primarily for most patients, because of one cause and one cause only: bad luck. That’s why you got this.”
Then we say, “In context, it could have been worse luck because there are worse things you could even have.”
Of course, the questions are, “What can I eat to make this get better? What vitamins can I take?” The answer is you should eat [healthily] and be healthy. Being healthy is not just about eating; it’s about physical activity and exercise.
We have a ton of data that physical activity and living healthy improves outcomes for cancers, for lymphomas. But we don’t micromanage and have a specific, “Oh, you need these blueberries, this green tea, this antioxidant.” Healthy eating [and] healthy living is critical, but the details [are] probably not critical.
Being healthy is not just about eating; it’s about physical activity and exercise. We have a ton of data that physical activity and living healthy improves outcomes for cancers, for lymphomas.
Dr. Brody
Immunotherapy for DLBCL
Stephanie, TPS: What can be critical is how much we know, as patients and caregivers or care partners, to make sure that we’re getting the best care.
The standard of care has been R-CHOP as a first-line [treatment] for people in aggressive chemotherapy. But if that doesn’t work for the patient, then there’s that gap. What can we go to?
There’s been this big focus on immunotherapy and we’ve heard about CAR T-cell therapy and that’s been approved in DLBCL. What was really exciting at [ASH 2022] is bispecific antibodies and that’s really had a lot of progress in research, too.
Dr. Brody: We were already lucky in lymphoma to have more progress than before. [In the] last couple of years, I would say the rate of progress has only increased.
If there’s a unifying theme of things that are being invented in labs by companies [and] in academia, it’s immunotherapy [or] using our patients’ immune systems to kill their own cancer.
People thought this was a bunch of hocus pocus 15 [or] 10 years ago. We’re going to use your immune system to fight this problem. But now, it is a real, measurable, making-people-live-instead-of-die thing.
The progress in DLBCL immunotherapy has been unprecedented, especially [in] the last couple of years. The most obvious examples are CAR T-cells. When I describe this science-fiction-like immunotherapy to my patients, they say, “But that’s not a real thing.” I say, “No, it’s real,” and then we describe it. It’s quite remarkable.
[There is] even this somewhat-simpler type of immunotherapy that I think will actually have [a] greater impact overall than CAR T-cells, which is this class of medicines called bispecific antibodies. [It’s] another immunotherapy that gets your immune cells to kill cancer cells.
The progress in DLBCL immunotherapy has been unprecedented.
Dr. Brody
CAR T-cell therapy in earlier lines of treatment for DLBCL
Stephanie, TPS: To be clear, the idea of using your own immune cells to kill cancer is an idea that’s been around but in the last few years is when we’re really seeing the impact of this.
Before we dive into this big buzz of bipecifics, let’s talk about CAR T. As some people may or may not know, there have been three CAR Ts that have been approved in DLBCL, but they’ve been approved for third-line of treatment. Again, the first treatment didn’t work, [the] second treatment didn’t work, [and] now we’re going to the third one.
Dr. Brody, as you mentioned, CAR T has been able to put many patients into deep, complete remission, which is what we’re looking for. But the last year has shown that CAR T can be promising even earlier on. Is that right?
Dr. Brody: Some big trials [are] showing remarkable benefit [with] CAR T-cells as second-line therapy — not as the first therapy, but as second-line therapy. They had to show that they were better than the standard in that place.
That standard for second-line was aggressive chemo and autologous stem cell transplant, which is just very aggressive chemo. It was focused on the highest-risk people, [those] with DLBCL who relapsed within the first 12 months. That meant a lot of people relapsed in month 3 [and] month 6. Some of them didn’t even relapse at all; they got no response at all from the front-line R-CHOP chemotherapy.
On these highest-risk patients, the benefit of CAR T-cells compared to the old standard was remarkable. Many more of them [are] staying in remission for months now. Now, at [ASH 2022], we have a year-and-a-half follow-up. One of those trials [shows] many more patients staying in remission.
[With] the old numbers with CAR T-cells, we thought maybe we were curing 35-40% of patients just with CAR T-cells. We’ll see if those numbers reproduce or might even be better now [by] using them in the second-line setting. That is for the highest-risk group of DLBCL patients that we’re talking about.
Bispecific antibodies are a real breakthrough class of medications for lymphoma and many hematologic malignancies… I like to refer to bispecific as the third big milestone in immunotherapy for lymphoma.
Dr. Falchi
Bispecific antibodies in the treatment of DLBCL
Stephanie, TPS: That’s really great. Let’s go into bispecific antibodies or bispecifics. Dr. Falchi, what is going on with them? Why are people so excited by them and how do they work?
Dr. Lorenzo Falchi: Bispecific antibodies are a real breakthrough class of medications for lymphoma and many hematologic malignancies, that is blood cancers. What makes them a breakthrough is they’re novel technology that really translated into very impressive clinical results and a real benefit for patients.
I like to refer to bispecifics as the third big milestone in immunotherapy for lymphoma. The first [is] monospecific antibodies, like rituximab that most people are familiar with in the field. The second [is] CAR T-cell therapy. I think the third would be bispecific antibodies.
Dr. Brody: Bispecific [antibodies are] actually very similar to CAR T. CAR T sounds so fancy. It’s hard to believe. We take some immune cells out of your blood. It takes a few hours, not too big of a deal. We put a new gene in them. The gene is called a CAR gene.
You put that CAR into the T-cells. Now they call them CAR T-cells. We take the blood out, mail this someplace — it used to be Santa Monica, now there [are] a few places — and then they mail it back to you. Then you reinfuse those CAR T-cells into the patient.
Bispecific antibodies [use a] very similar idea, just maybe a little simpler even. We don’t actually have to take T-cells out to make them recognize lymphoma. We put in a bispecific antibody.
Many folks have heard of rituximab. The regular antibody binds to one protein on one cell. [A] bispecific antibody binds to two cells. It binds to your lymphoma cell, binds to your T-cell, [and] brings them together. One of my colleagues said, “This is like the ‘Lady and the Tramp’ with the spaghetti in between them.”
At the very end of the spaghetti, in this case, it’s the kiss of death, because the T-cell kills the cancer cell. That “Lady and the Tramp” image is a pretty good one. I have to credit Dr. Matthew Lunning for the “Lady and the Tramp” metaphor. [With] that kiss of death, these T-cells are highly activated and able to kill. That immune cell kills that cancer cell quite effectively.
In folks where standard therapies didn’t work, where CAR T-cells weren’t working, it seems like more than a third of patients with these bispecific antibodies are getting complete remissions. Again, that’s the highest-risk group of patients. In the worst-case scenario, it seems like more than a third of them are getting complete remissions.
Even when the best things weren’t working, bispecifics, [and] epcoritamab in that case, [was] still highly effective.
Dr. Brody
Bispecifics in clinical trials
Stephanie, TPS: Let’s break down what we should be looking for in terms of bispecifics. As we know, these drugs are being developed in clinical trials. There are different phases where they’re bringing them to patients and seeing how patients do on them, studying dosages, and not just how effective they are in terms of how much more people can live without the disease but how well. What are the side effects? Which ones currently in clinical trials are expected to get approvals sooner?
Dr. Falchi: I think it emerged quite clearly that the two main actors in the world of bispecifics for patients with diffuse large B-cell lymphoma are epcoritamab and glofitamab. These drugs are both highly potent. Very, very powerful. In fact, before using them in patients, it was shown in experiments that their potency is exactly the same.
Dr. Brody: Because they have so many patients now, they really got to parse out the patients with high risk, super high risk, and all the different risk factors.
As we said, CAR T is very promising but a year or two ago, if CAR T failed, the options were not great. About a third of the patients in both the epcoritamab and glofitamab trials already had CAR T. CAR T didn’t work because it’s not a guarantee. It’s great, but it’s not a guarantee.
Epcoritamab or glofitamab — at [ASH 2022], we’re talking more about epcoritamab in that parsing of the data — [were] still giving complete remissions in more than a third of patients. Even when the best things weren’t working, bispecifics, [and] epcoritamab in that case, [was] still highly effective.
Glofitamab so far has some advantage in that all the recipes for them have been written as time-limited. You get 12 cycles and you’re done. Nine months of therapy and then you get a break.
Epcoritamab studies have been written so far to be continuous therapy, as long as it’s helping you and not hurting you. Whether we need to keep giving it for a long time, we don’t really know. At least, it’s a difference so far.
The other big obvious difference is that [with] epcoritamab, the way we [give it] is different. It is a subcutaneous injection, so it’s a quick little shot and you’re done. You’d almost think you could just get it at home, but we haven’t worked on that yet. Glofitamab is an IV infusion still.
Rates and severity of CRS for bispecific antibodies appear to be, at least at this stage, quite substantially different compared to what we see with CAR T-cell.
Dr. Falchi
Cytokine release syndrome (CRS)
Stephanie, TPS: We don’t have any FDA-approved bispecifics in the DLBCL space yet. The hope is that maybe there will be approvals sometime in 2023. This is information based on these research studies.
A very important topic is side effects and quality of life. We can extend life by X number of months or someone’s in remission for this amount of time. But we also truly want to understand: are we going to be able to live well while on this treatment or even once we get off of the treatment? Can you set the stage for what kind of side effects we’ve seen so far in the studies with bispecifics?
Dr. Brody: We talked about all the promises. We do not want to oversell this. There are also side effects of these medicines. The most significant or maybe concerning side effect of all of these bispecifics, really all these immunotherapies, is the risk that we push your immune system too hard and you get a reaction as though you had an infection, but there is no infection. It’s just that we pushed your immune system to react.
One version of that is a side effect [is what] we call CRS: cytokine release syndrome. CRS can be significant. [It can] make you get a high fever [and] make you get low blood pressure. If you get a [really] bad version of this, you have to be in the hospital for observation and sometimes for treatment of that.
With CAR T-cells, those high-grade CRS events were pretty common. They’ve gotten better as we’ve gotten more experience using them. With bispecifics, the numbers are better but that risk is still there.
For both bispecifics, epcoritamab [and] glofitamab, the standard today is that people have to get hospitalized for at least one day just to observe them after they get the first higher dose of that infusion.
Dr. Falchi: Both administrations are given usually without side effects. The main side effect that ensues a little bit later is something called CRS or cytokine release syndrome. For those who have experienced CAR T-cell, this is a very well-known adverse event.
It’s an inflammatory reaction where people can have fever [and] chills, their blood pressure could decrease a little bit, [and] there can be some confusion. It can be scary because it comes up quite suddenly and it may become quite apparent quite early. Very rarely, it requires hospitalization and may need care.
For the most part, we were very pleased to see, in both the epcoritamab study and the glofitamab study, that the percentage of patients who have a severe cytokine release syndrome is much less than 5%. The majority of patients will have some fever [and] chills, and generally, these will resolve within a day or two.
These rates and severity of CRS for bispecific antibodies appear to be, at least at this stage, quite substantially different compared to what we see with CAR T-cell, particularly Axi-cel, which is one of the most utilized products for diffuse large B-cell lymphoma.
In the CAR T-cell studies, we’re looking at [a] double-digit percent of higher grade CRS. For that reason, most patients, particularly those who are a little bit more advanced age, need to be hospitalized for several days after receiving CAR T-cell.
For bispecific antibodies, we’re looking at a 24- to 48-hour hospitalization. We’re confident that in the future, as we gain more experience, there is a possibility that these drugs — [which are] off-the-shelf products so [they are] immediately accessible — can be given on a fully outpatient basis without having [to be] admitted to the hospital.
Although none of these [bispecifics] are currently approved by the FDA, it is hoped that one or more of them will be approved in the near future because of such promising results.
Dr. Falchi
Deciding whether to give bispecific antibodies or CAR T-cell therapy
Stephanie, TPS: To be clear, we’re not saying that with bispecifics being so promising if they are approved, they’ll erase the need for CAR T-cell therapy. But what we’re talking about is there are details that are coming out in this research that will help doctors, patients, and care partners determine the best treatment path for each individual.
Some of those factors include what is available [and] what is quicker to get because sometimes, time is going to be a big factor. What are the side effects? How long would someone need to be monitored in the hospital or the clinic for side effects that are more severe, like CRS, the way you’ve both described?
Is there anything else that you would consider in making the treatment decision about whether someone should go on a bispecific or CAR T?
Dr. Falchi: On a logistical basis, CAR T-cell therapy is quite an involved therapy. It needs to be administered by specialized centers.
In the US, there [are] many such centers, but they’re not everywhere so it’s important to know where these centers are [and] who can administer those therapies. Doctors have to be certified. Centers have to be certified. It is not a therapy that everyone can give.
They require hospitalization for the majority of patients. Some patients can receive CAR T-cell therapy on an outpatient basis but for now, I would say, that’s a minority of patients. The majority will require hospitalization and monitoring. Even after discharge, oftentimes patients will be required for a period of time to stay in the area where [the] CAR T-cell therapy was administered.
In the post-CAR T-cell therapy period, there’s periodic monitoring where the doctors will want to look at blood counts, other blood work, or scans multiple times in the months ensuing CAR-T cell therapy.
As far as bispecific antibodies are concerned, these are drugs that are administered either subcutaneously or intravenously for the most part, on an outpatient basis. And this is important because although none of these drugs are currently approved by the FDA, it is hoped that one or more of them will be approved in the near future because of such promising results.
Therefore, it’s important for us as academic clinicians and for our colleagues to become very familiar with this product. I think, really, the point to make about these drugs is that they can be safely administered as outpatient therapy. Their main side effect, which is cytokine release syndrome or CRS, is something that is to be expected in a certain percentage of patients and we all will need to become familiar with it and how to manage it promptly.
Management of CRS from bispecific antibodies has not been as “complicated” as it has been for CAR T-cell therapy in the sense that drugs like acetaminophen, drugs like steroids including prednisone or dexamethasone, which are drugs that we very commonly use and most patients are familiar with, are the mainstay of therapy for most cases of CRS related to bispecific antibodies.
Only rarely will patients treated with bispecific antibodies need [a] higher level of care that includes hospitalization and other drugs that are used to calm down a more severe CRS.
With these easier-to-use bispecifics, the next step is how we can combine them with some standard therapies.
Dr. Brody
Bispecifics given as single agents and in earlier lines of treatment
Stephanie, TPS: Bispecifics right now [are] being studied both as single agents, meaning just the bispecifics alone, but also in combination with other treatments that are already being used. We’ll have to see how those turn out.
As we’re also talking about different bispecifics, we know that they’re being tested for later lines — third, fourth, fifth — and then typically what happens is the research tries to move them earlier.
Dr. Brody: The real future of that is not just how good they are alone because we never really cured any cancers alone. We don’t cure some DLBCL patients with C; we cure them with R-CHOP. Combinations are the basis of oncology.
With these easier-to-use bispecifics, the next step is how we can combine them with some standard therapies. That’s already being done. We have some data about that at the ASH [2022] annual meeting and those response rates are extremely high. That is the future.
For now, it’s third-line patients where everything else has failed, but they are very quickly moving up into the second line. We have some data about the second line.
We’ve already started studies bringing them into the first line in combination with standard therapy. It’s a rate of progress. We’re very lucky.
The luckiest thing would be to have no cancer at all, but if you had to have something, [it’s] better to have something where the progress is being made this quickly.
Dr. Falchi: As single agents, I think what we’ve seen is that now, with longer follow-up for these studies, some of those individuals who had a very good response early on tend to maintain that response. There is a suggestion that some of these patients may become long-term disease-free. In other words, being alive and well without evidence of disease at a relatively long follow-up time.
We’re all very cautious toward the word cure, but we certainly believe that there is a potential for these people not to have a recurrence.
[The goal of] adding epcoritamab to that second-line platinum chemotherapy [was] just trying to get complete remission rates up high enough that the transplant would work better.
Dr. Brody
Epcoritamab for transplant-eligible patients who didn’t do well post-transplant
Stephanie, TPS: Thank you, Dr. Falchi. One example is a study that was presented on patients who are eligible for transplant but didn’t do well after the transplant so they’re studying epcoritamab or epco for these patients. What was the main takeaway there?
Dr. Brody: There’s one abstract about epcoritamab plus this aggressive platinum-based chemotherapy. R-DHAOx or R-DHAC are aggressive, platinum-based chemotherapies that are usually a plan B.
Plan A [is] something like R-CHOP and if it doesn’t work, plan B for younger, healthier patients would be to get platinum chemotherapy [like] R-DHAC, R-DHAOx, [or] other similar ones. R-ICE is another similar one there. They’re all just platinum chemotherapies. If it works well, then [they] go on to autologous stem cell transplant.
Stem cell transplant sounds a little elegant because stem cells are involved, but it mostly involves tough chemotherapy. Folks are hospitalized for a while and out of work for a while.
[The goal of] adding epcoritamab to that second-line platinum chemotherapy [was] just trying to get complete remission rates up high enough that the transplant would work better.
In that trial, although patients intended to go on to stem cell transplant, some patients that got complete remission with just epcoritamab plus platinum chemo never did go on to the transplant and are still in remission at beyond a year now.
We cannot yet say if those patients are cured. They may be. A little more follow-up would hopefully confirm that. Epcoritamab is clearly making that chemotherapy work much, much better.
Dr. Falchi: We participated in that study and the early results on a relatively small number of patients appear very promising.
For those patients who are able to complete the program, their chance of response was 100% and the majority of them were complete response, meaning that lymphoma really disappeared. Obviously, we don’t know what’s going to happen in the long term, but there’s certainly a very, very good start.
Importance of patient-reported outcomes
Stephanie, TPS: That sounds so promising. One thing we’d like to highlight is that research relies so heavily on data, on the numbers, and that’s for a very good reason. Putting the numbers and percentages into context is really important.
Some of the research presented at the conference is called PRO or patient-reported outcomes. Very simply, it’s something I hope there’s a lot more of because it gives that context.
There was one report for epcoritamab on quality of life where 61% of interviewed patients reported [a] positive impact on their daily activities after being on the bispecific. Around 40% reported a positive impact on physical, emotional, and/or social functioning and 80% of patients reported being “very satisfied or satisfied with treatment.”
Now, again, [we] want to stress [that] this was a limited sample size. It was in this clinical trial of more than 100 patients. But I do want to ask you, Dr. Brody, why is this information so important to study?
Dr. Brody: Patient-reported outcomes are critical because the other version of that kind of data is so unfulfilling. It is just these kinds of graphs of adverse effect frequencies but that does not tell the story.
If someone had grade-3 toxicity for 20 minutes or for two years, it adds up as the same on the graph. It’s just they had a grade-3 toxicity.
A human experience is that 20 minutes [is] not so bad. Two years? I would rather have a grade-3 toxicity of many types for a day than have a grade-1 toxicity for a year. Grade-1 toxicity for a year, you maybe can’t go to work or can’t work well.
That’s why patient-reported outcomes [are important] especially, I think, for these immunotherapies, especially for bispecifics.
This main side effect for bispecifics, the most common one, is cytokine release syndrome. It can be bad. It can be serious. You can end up in the ICU from it.
The nice thing about it is people either have it or they don’t. Maybe 20% of people have a bad version of that immune overactivation and [for] those that do, [it] mostly lasts for about a day or two. Then they pretty much don’t ever have it again. That is a grade-3 toxicity, but for most people, it is two days, God-willing, out of their life.
The way we normally report these in meetings, abstracts, and publications falls short because the patient’s perspective is that a two-day side effect is not the same as a two-year side effect. It’s totally neglected in the way we present the data. That’s why the patient-reported outcomes are critical and why the numbers, I think, are very promising for these types of immunotherapies.
These are breakthrough therapies that offer hope to a substantial proportion of individuals, of people that would otherwise have very little outlook suffering from a recurrent lymphoma that can be unforgiving.
Dr. Falchi
Breakthrough therapies for DLBCL offer hope
Stephanie, TPS: Asking patients for their perspectives is so important and, again, something I hope will trend in that upward direction.
What is the general takeaway for DLBCL patients and for their loved ones as we go deeper into 2023?
Dr. Falchi: My general takeaway about bispecific is one of great excitement. It is my line of research because I truly believe that these are breakthrough therapies that offer hope to a substantial proportion of individuals, of people that would otherwise have very little outlook suffering from a recurrent lymphoma that can be unforgiving.
Opening avenues of hope for patients with diffuse large B-cell lymphoma that recurs after one or more lines of therapy, which is very, very challenging to deal with, is something that I think we’re all excited about. I’m personally just looking forward every day to what’s coming next and how many more people we can cure hopefully more and more each day.
Stephanie, TPS: Thank you so much, Dr. Falchi and Dr. Brody. So excited by the things that were discussed. We couldn’t cover everything that’s happening. We’ll definitely be putting on more conversations for people who are wondering more comprehensively what’s available out there.
The numbers are promising, but how soon are we going to see this at our hospital or at our clinic? Will it be accessible? What are the side effects? Will I be able to live life while I’m on this treatment?
With everything that’s happening right now, it is so important to be up to speed on the latest that’s happening so that you can ask those questions of your doctor and make sure that you or your loved one is getting the best care possible. Remember, you are not alone.
Thank you to Genmab for their support of our patient education program! The Patient Story retains full editorial control over all content.
Stephanie Chuang, founder of The Patient Story, celebrates five years of being cancer-free. She shares a very personal video diary with the top lessons she learned since the Non-Hodgkin lymphoma diagnosis.
Cancer details: Characteristics of both subtypes 1st Symptoms: Lower abdominal pain, blood in stool, loss of appetite Treatment: Chemotherapy (Part A: R-CHOP, HCVAD, Part B: Methotrexate, Rituxan, Cytarabine)
Dr. Matasar sat down with Samantha Siegel, MD, a relapsed/refractory Hodgkin lymphoma patient, to discuss some of the most exciting news coming out of ASH 2022.
The American Society of Hematology (ASH) hosts an annual comprehensive meeting that covers new research, scientific abstracts, and the latest topics in hematology.
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Introduction
Dr. Sam Siegel, The Patient Story: My name is Sam Siegel. I’m a mom of three, a physician [in] internal medicine, an avid jogger, and somebody who generally lives a very healthy life and enjoys life. I was pretty shocked when I was diagnosed with stage 2 Hodgkin’s lymphoma on the eve of my 38th birthday.
That’s got a pretty high cure rate of about 90%, especially if you go through with the recommended chemotherapy, which I did. I took six months of the standard chemotherapy regimen called ABVD.
I completed all six months and had a scan shortly after finishing that declared that I was in remission. I had no evidence of disease and what some people would even consider cured. But I really wasn’t feeling well. Even though the scan was clean, I wasn’t feeling right.
Ultimately, I had to get chest surgery to get a lymph node right near my heart in order to get diagnosed with the relapse. Once that was diagnosed, I started targeted therapy.
It’s been an incredible journey from doctor to patient and pretty soon back to doctor as I start easing back into practice towards the end of my maintenance chemotherapy that I’m on post-transplant. But it’s taken a long time to recover and to evolve as a person and make meaning of this experience.
[During] the first round of this, I kind of felt victimized by the whole process and that if I did what the doctor said and followed through with everything, it would be a nuisance of four to six months. I’d lose my hair but it’d be cured and I’d never hear from the thing again.
When it didn’t work out that way, I began to see it differently altogether. I choose to believe that this cancer came into my life as an opportunity to learn about my health and my well-being, about setting realistic goals and expectations for myself, about taking care of myself and making a space for my own self-care.
And that’s one of the main reasons why we’re having this conversation today with top Hodgkin’s lymphoma specialist Dr. Matthew Matasar with Rutgers Cancer Institute. What are the most up-to-date treatments? How should patients be thinking about Hodgkin’s lymphoma in this new era of immunotherapy and all the new therapies that are offered?
The landscape of treatment has really changed in the last 10, 20 years and that’s after decades and decades of very little change in Hodgkin’s treatment. So I think it’s a really hopeful time and a really wonderful time to be having this conversation.
Tell us about your journey into medicine
Dr. Siegel, TPS: Can you tell us a little bit about your journey into medicine and how you became interested specifically in blood cancers and lymphoma?
Dr. Matthew Matasar: When I was in college, I was a philosophy major and I went to medical school because I wanted to become a medical ethicist. I was told by my philosophy professors that if you want to be a medical ethicist, you need to have an MD or else nobody listens to you. You have no chops. So I went to medical school with the intention of being a philosopher [and to be] a medical ethicist.
When I got to medical school, there was patient care, research, and science. It turned out to be super interesting, fun, richly rewarding, and hard. And I was hooked.
Then [I] was trying to figure out where I could have an impact. My thinking has always been, “I want to be somewhere where what I’m doing matters and where if you’re good at it, it really matters.” If I can work hard and be good at something, I can actually make the world a better place in some small way. And that led me to cancer medicine, to oncology.
I was introduced to the field of lymphoma by wonderful mentors and I was overwhelmed by how little I knew and how little we knew about these diseases. I was like, “Yeah, I could imagine doing this for 30, 40 years, and I still won’t know everything I want to know, but maybe I can make a difference and help people along the way and I’ll never be bored.” And here we are.
My thinking has always been, ‘I want to be somewhere where what I’m doing matters and where if you’re good at it, it really matters.’
What’s new at ASH 2022 on Hodgkin’s lymphoma?
Dr. Siegel, TPS: Do you have any hot-off-the-press, new announcements in Hodgkin lymphoma that you’d like to share?
Dr. Matasar: ASH is chaos incarnate. There’s just a ton of science. Everybody is presenting everything new.
We continue to learn how best to use our best medicines in treating patients with Hodgkin lymphoma when they’ve been newly diagnosed as well as when, unfortunately, the disease has come back despite receiving good treatments.
There [are] a lot of questions about the best way to treat patients when they have a new diagnosis. We have all these good medicines — chemotherapy programs, targeted therapies, novel therapies, [and] immunotherapies. We have all these tools in our bag, each of which has good effects in terms of treating or hopefully helping to cure Hodgkin lymphoma, and each of which has bad things about it — side effects, risks, toxicities, things that it does that hurt people.
How do we mix and match all of these tools to come up with the best approach for an individual person? How [do we] personalize that approach? How do we tailor it so that we’re maximizing the chances of cure and, at the same time, minimizing short and long-term risks from treatment? This is the holy grail of Hodgkin lymphoma. How do you maximize cure and minimize risk? We have some good insights [from ASH 2022] in Hodgkin’s and [we’re] continuing to move that forward.
This is the holy grail of Hodgkin lymphoma. How do you maximize cure and minimize risk?
There’s long been this understanding that immunotherapy treatments, [which] harness the immune system to kill cancer cells instead of just poisoning them with chemotherapies, are very powerful treatments [for] Hodgkin lymphoma. We know this and there [are] many FDA-approved treatments to treat Hodgkin lymphoma when it’s come back after traditional treatments have failed. A lot of us want to figure out how best to use those medicines for patients before their lymphoma comes back. How do we use those to cure them the first go around?
There [are] a lot of different ways that you can imagine doing that. You can imagine we’re going to use these medicines in everybody who’s diagnosed with Hodgkin lymphoma — if you have a little bit, if you have a lot, if you have early stage, advanced stage, if you have bulky disease, [if] you don’t have bulky disease. Maybe everyone should get immunotherapies. Maybe nobody should get them. Maybe only people with high-risk disease should get them. Maybe we should only use them when treatments look like they’re not working as well as they should.
We’re continuing to get [a] first look at a lot of the clinical trials, evaluating using immunotherapies in combination with chemotherapy for patients with newly diagnosed Hodgkin lymphoma with the intention of trying to maximize cure, minimize risk. I would say the data at ASH is a little bit of a mixed bag. We’re seeing very good success in terms of getting patients into remission by combining chemotherapy and immunotherapy.
We also see that incorporating immunotherapy into treatment programs for patients with Hodgkin lymphoma comes with a price. And I don’t just mean financial price. They come with risks.
Immunotherapies activate the immune system. That can cause trouble because that activated immune system can then act against your body, [which] can lead to immune reactions where the immune system is injuring healthy parts of your body and causing lung inflammation, inflammation of your intestines or your skin, and vital organs like your heart. We have greater insight now into that risk-benefit profile [and] the risk balancing of using these treatments in patients with newly diagnosed Hodgkin lymphoma.
My read on the data is that we’re going to need to be a little bit choosier in who we use these powerful but not-without-risk treatments. It shouldn’t be a one-size-fits-all approach. I think that’s the wrong way to do it. The data at ASH supports that. If you use it as [a] one-size-fits-all, you’re going to lead to side effects that maybe were avoidable.
We need to be a little bit more nuanced, a little more subtle, [and] a little smarter in picking who we think needs these treatments in order to achieve cure and not have to go through the rigors of the treatments that we use to cure this disease when it’s come back after good first treatments.
We’re continuing to get [a] first look at a lot of the clinical trials, evaluating using immunotherapies in combination with chemotherapy.
How do chemotherapy and immunotherapy work?
Dr. Siegel, TPS: Could you tell us a little bit more about how traditional chemotherapies work, how immunotherapies work, and how the safety and side effect profiles compare with the two therapies?
Dr. Matasar: We can do that by taking a little bit of a walk back and looking at how the treatment for Hodgkin lymphoma has evolved over these last few years.
Since I was in medical school, the treatment was ABVD chemotherapy. A, B, V, D — four medicines. Each one of the different chemotherapy medicines [is] given in combination. These medicines [are] given by vein every other week for some number of months, up to six months in total. And this treatment cured many, although not all, patients.
We always wanted to do better. We knew that ABVD chemotherapy has side effects, particularly B in ABVD — a medicine called bleomycin — and that medicine is well-known for its risk of potentially causing lung injury, which obviously is not anything that we ever want our patients to experience. We’ve been trying to get rid of that drug and a very important clinical trial was conducted globally.
ECHELON-1 was a large randomized clinical trial. The great computer in the sky flipped a coin. If it came up heads, they would get ABVD and if it came up tails, instead of the B, they would get a new medicine called brentuximab vedotin or BV for short, and that would get switched out instead of the old bleomycin. It compared this new AVD plus BV compared to the old ABVD treatment.
In that study, we learned that patients who get the new treatment with BV are more likely to be cured and live longer than patients who receive the traditional ABVD treatment. That was a landmark event. It tells me that I now have a better tool to cure more people and help them live longer than I could before, which is awesome, so that moved us forward. Now we have AVDBV as our new and improved standard treatment.
My hope is that we will be able to cure more people using immunotherapies the first go around
The question is: can we do better and can we then incorporate things like immunotherapies on top of that? Many people are looking [and] saying, “Can we add immunotherapy onto AVDBV or switch one of those drugs out and add in immunotherapy? And can we continue to ratchet up the sophistication of our treatment to cure more people and help them live longer?” We don’t know yet. That’s the work that’s ongoing.
My hope is that we will be able to cure more people using immunotherapies the first go around but we need to figure out exactly [which] patients benefit the most, who needs it the most, as well as who’s more likely to have side effects with this medicine.
Dr. Siegel, TPS: How are those medicines given? Would that look like an infusion every couple of weeks like ABVD?
Dr. Matasar: In some ways, logistically, the patient experience is similar, whether you’re getting ABVD, AVDBV, [or] incorporating immunotherapy.
Typically, what this looks like is you come in [and] you see your doctor or his or her team to make sure you’re doing okay. They check your blood [and] make sure everything’s copacetic.
You get your treatment intravenously [by] putting an IV into a vein in the arm. If they have trouble getting IVs, [there needs to be] some way to give the medicines intravenously safely and that can be some form of a catheter, which is a tube that goes into a blood vessel in the chest, or what’s called a mediport, which is a little button that gets put under the skin of your chest with a little tube that goes out.
These treatments are typically given every other week. For patients with advanced-stage diseases, treatments are typically given for six months or six cycles or 12 treatments, however you want to parse it out. But that’s often what patients can expect to experience.
There is no stage of Hodgkin lymphoma that’s not curable… Stage is important because it tells us how hard we got to work at this.
What does staging mean in cancer?
Dr. Siegel, TPS: You touched on staging and I think that’s a really important clinical point for patients. You mentioned we’re trying to individualize treatment for Hodgkin’s patients based on their risk of relapse, their age, and their underlying health. There are terms going around like early stage but unfavorable versus later stage. What does that mean? There are a couple of different classifications.
Dr. Matasar: For a lot of cancers, stage is king. Cancers start in an organ in the body — your breast, your colon, your prostate, or some part. Stage is oftentimes the most important thing about what this is going to look like for you. What’s your experience going to be? Stage 1 — Yay! We got it so early! Stage 4 — often a very different conversation.
This is not the case for Hodgkin lymphoma. There is no stage of Hodgkin lymphoma that’s not curable. Staging is just fancy [medicalese] for describing where in the body the cancer is. Stage 1 means it’s in one lymph node or one lymph node area. Stage 2 is in a couple of lymph node areas but all on one side of the body.
We think of the diaphragm as the Mason-Dixon line for the body. If it’s on both sides, then that’s advanced stage or stage 3 — lymph nodes above and below the Mason-Dixon line.
Stage 4 just means it’s in lymph nodes and something else in your body — could be an organ like your liver or your lung.
When some types of cancer have spread into other organs, that’s a very different situation from where those cancers start. Hodgkin lymphoma is a lymphoma, a cancer of lymphocytes, of immune cells, so this is [a] cancer that comes from the immune system. By its nature, your immune system is through the whole body so it shouldn’t be a surprise if these cancers show up in more than one spot. It doesn’t have anything to do with whether or not that illness is curable.
[The] stage is important because it tells us how hard we got to work at this. Patients who have less disease generally need less treatment to achieve their best chance of cure. Patients who have more disease will often need to receive a more comprehensive course of treatment in order to give them the best chance of achieving the cure, which we not only know is possible, but usually expect to achieve for our patients.
That question of whether we should do risk-adapted intensification of treatment is still, I would say, an experimental approach.
Where do PET scans fit in the treatment plan?
Dr. Siegel, TPS: Where do PET scans fit in there? There’s this idea [of] PET-adapting therapy — getting your PET scan when you start, then getting a PET scan after you’ve had some treatment, and then using that to tailor the treatment as you go. What does that mean and how can that be used?
Dr. Matasar: A PET scan is a type of body scan. It’s a way of taking pictures of inside the body, like a CAT scan where you will often use medicine that lights up the blood vessels so you can see what you’re looking at — very clear black and white pictures. A PET scan is more like an Andy Warhol painting — very bright, vivid colors and you get a lot of information about what’s going on.
What lights up in a PET scan is metabolism. It’s what parts of your body are actually using sugar for energy and the more sugar that absorbs, that sugar then is actually a little bit radioactive, and it glows for our cameras — not radioactive in a dangerous way, but radioactive in a I-can-take-pictures-of-that kind of way.
By doing a PET scan, you can see what areas in the body have unusual or abnormal metabolism. We know that Hodgkin lymphoma is very metabolically active. Those cells are using lots of energy so they light up very brightly on a PET scan. I can see those areas that are lighting up and that is really how we best stage our patients. It’s the best look at where the cancer is and isn’t at the start of treatment.
We know that many patients with Hodgkin lymphoma will have very quick improvement [in] their PET scans, even after only two months of treatment. Oftentimes, after just that little bit of treatment time, that PET scan will often be already normalized. That’s often our expectation going into treatments that the scans should get that much better that quickly.
Back when we were doing ABVD chemotherapy, I’ve already mentioned that bleomycin can be hard on the lungs. We know that the more bleomycin we have to give our patients, the more risk there is of causing lung injury. So we used the PET response adapted approach.
We would do treatment for two months and we’d do a PET scan. If that PET scan was already looking great, yeah! Awesome! We’re on the right track. Let’s not give any more bleomycin. Let’s take it easy on those poor lungs and just do AVD — no more B — and finish the next four months or six months of total treatment, but no more bleomycin to spare lung injury.
We’re not doing so much ABVD anymore. We’re doing a lot of BVAVD. We don’t have the same approach right now in terms of tweaking our treatment along the way based on that PET scan that we do after two months. We still tend to do it because we think it gives us pretty good predictive power in terms of how things are going.
There are situations in which that scan after two months may be so spooky looking to us that we may recommend moving to an even stronger chemotherapy program in order to try and make more progress. Two months, not such great news so far, kick it up a notch.
That question of whether we should do risk-adapted intensification of treatment is still, I would say, an experimental approach. We continue to see data emerging at ASH and other congresses as people look at ways of trying to address people who have an unfavorable or worrisome scan after the first two months to try to make more headway.
We recognize pretty well that radiation therapy, as effective as it is, carries a long-term risk for some patients, depending on where the radiation therapy is delivered.
Where does radiation fit in all this?
Dr. Siegel, TPS: Where does radiation fit in all this for Hodgkin’s?
Dr. Matasar: I would say that radiation therapy is still absolutely an important treatment modality that we have in our pocket. If you want to be rigorous about it, we would say that radiation is the single most active treatment in the treatment of Hodgkin lymphoma. It’s the thing you can do that is most guaranteed to get a quick response when you need it.
We are using radiation therapy a lot less than we have in months, years, and decades past and that’s because we’re trying to maximize cure but also minimize short and long-term risks. We recognize that radiation therapy, as effective as it is, carries a long-term risk for some patients, depending on where the radiation therapy is delivered.
Chemotherapy goes to the whole body from the nose to your toes so it can affect the whole body in terms of side effects. Radiation therapy is a focused treatment on a certain area and wherever the beam shines is wherever is being affected. If that beam shines on healthy tissues, there’s a risk of causing injury to those healthy tissues.
Radiation therapy for Hodgkin lymphoma is well-known for carrying certain important risks, depending on where that beam may shine. What if that beam is shining on breast tissue? In younger women and women under the age of 35 — definitely 30 — we know that if radiation therapy touches breast tissue at that young age, it can confer an increased risk later in life of developing breast cancer. And the last thing any of us want to do as doctors is to give treatments that put our patients at risk of other cancers later in life.
It’s very challenging. Do we use it anyway? Yes, if you have to. If it’s that or Hodgkin lymphoma presenting a peril to life and limb, then, of course, you have to do what you have to do. Then you are talking about how you apply good survivorship care after Hodgkin lymphoma has been cured to work to protect and safeguard a patient’s health in the months and years to come.
For patients and their caregivers, the most important thing to remember is that survivorship care is cancer care.
Survivorship & patient care
Dr. Siegel, TPS: You just touched on survivorship and some of the most important issues that survivors are facing long-term. Survivorship becomes a really, really important issue for the decades after patients are cured of their Hodgkin’s. What are some of the top things, in addition to the potential injuries to the tissues or secondary cancers that patients may get from having had the treatment?
Dr. Matasar: For patients and their caregivers, the most important thing to remember is that survivorship care is cancer care. Everybody who’s gone through Hodgkin lymphoma deserves to receive compassionate, thoughtful, wise survivorship care as they survive and live with their history of Hodgkin lymphoma.
Everybody should be able to generate what’s called a survivorship care plan, which is simply an easy, straightforward document that says this was my diagnosis — Hodgkin lymphoma. This was the treatment that I received — which medicines, which doses, how many rounds or cycles, did I need radiation therapy or not? If I did, what tissues in my body were touched by the radiation? What are the recommendations from my oncologist and their team regarding my care going forward? What do they think I need to do to be able to safeguard my health the best?
Whether it’s a digital document in your electronic medical record or something that you simply have in a file at home, that simple document can then go with you, [which] you can then share with your other doctors, your primary care providers, your other providers so everybody’s on the same page. Everyone understands what you went through and what everybody should be attentive to protecting your health going forward.
What goes into that in terms of what to do and what we advise our patients in terms of safeguarding their health depends on the treatments that you received and the risks that are associated with the various treatments that we give.
[For] people getting ABVD or BVAVD, the A in that program is a medicine called Adriamycin or doxorubicin. We know that medicine carries a risk of some small magnitude — but not zero — of increasing the risk of heart problems later in life. People that get these treatments should have attention to their heart health in the years and decades to come.
How much we need to scrutinize the heart, how often we need to do testing, and what types of testing vary from person to person based on how much of that medicine you needed and how healthy you are otherwise. Do you have other heart health problems or other medical issues that may complicate your heart health? That can be personalized in a survivorship care plan.
If there [are] complex needs, then people can actually get that care at survivorship clinics, which increasingly exist in the context of cancer centers. Patients who are survivors at [the] highest risk for complications from treatment can be followed in a more multi-disciplinary, thoughtful, data-driven way so that we can really do the very best job at protecting our survivors.
We’ve made such great strides in the treatment of patients, few though they are, who have their lymphoma come back despite good first treatments.
Advances in the treatment of the relapsed/refractory Hodgkin
Dr. Siegel, TPS: The relapsed/refractory group is a small subset of people in Hodgkin’s. My understanding from what I read of the abstracts at ASH seems hopeful even for patients who relapsed after having had a transplant and that’s really exciting for those of us who have already relapsed once.
Dr. Matasar: We’ve made such great strides in the treatment of patients, few though they are, who have their lymphoma come back despite good first treatments. Right now, we are able to cure the majority of people even when their lymphoma comes back after the treatment.
What I always tell my patient when I meet them for the first time, as I’m describing the choices that we have together to treat their lymphoma, I say, “Don’t forget that even if things go wrong and your lymphoma comes back, which is not what I hope or expect, but just remember that if it comes back, that is not a death sentence. We are still likely to cure the disease at that point. Cure meaning go away, never come back again, happily ever after, the end.
“That may require a little heavy lifting. It may require a little bit of creativity. But our expectation is still, even if it comes back, that we would and will be able to cure it. Just remember that. [On] those dark nights when you’re lying in bed and you’re worried about, ‘What if this isn’t working?’ You can remember, ‘Nope, Matt said that that’s not a death sentence and that there [are] lots of good things that we can do there.’”
That is true now after ASH just as it was true before and all the more encouraging. Where’s my encouragement coming from in this setting? I’ve been talking about those immunotherapies, as nuanced as I think we need to be about their use in patients with newly diagnosed Hodgkin lymphoma because those patients are often cured without such treatments.
In patients who have the disease come back after chemotherapy, we know that immunotherapies are very powerful and can really lead to a tremendously greater chance of cure than we had before those treatments were available to us.
We’re now understanding better how to combine those immunotherapies with other chemotherapy medicines that we traditionally use after [the] first chemotherapies have failed us. This combination of chemotherapy and immunotherapy for patients when their lymphoma comes back after good treatment is proving to be very powerful, safe, and highly successful at getting patients into remission or back into remission.
This combination of chemotherapy and immunotherapy for patients when their lymphoma comes back after good treatment is proving to be very powerful, safe, and highly successful at getting patients into remission or back into remission.
Dr. Siegel, TPS: That’s wonderful. I feel so lucky to be alive [at] this time in medical science and [have] accessibility to medicine. I think it’s just incredible. We’re so lucky that people are excited about this and interested and have continued to develop the science to help keep us alive.
Dr. Matasar: This is really a global effort. The amount of work that is being done at a global scale to improve outcomes for patients with Hodgkin lymphoma is breathtaking. And what that means is that the pace of discovery is breathtaking and our ability to continue to cure more patients safely and effectively and to restore them back to health, it’s truly inspirational.
The pace of discovery is breathtaking and our ability to continue to cure more patients safely and effectively and to restore them back to health, it’s truly inspirational.
Any words of advice to patients and caregivers?
Dr. Siegel, TPS: I agree. Any last thoughts that you think are important to relay to patients or caregivers?
Dr. Matasar: Don’t be afraid to ask questions. So often I have patients come in and they are overwhelmed — and of course. There’s so much relief to hear a plan, to hear good news that there [are] treatment options, and that cure is attainable that there’s a reluctance to want to rock the boat, to advocate for yourself, to ask questions, and to learn more.
That deference to the physician on this side of the chair? I don’t want that. I don’t need that. I would much rather be in a partnership and a conversation. What I tell my patients is that this is not my journey. This is your journey. You’re the one climbing the mountain. I’m the Sherpa. I’ll drag your bags alongside you. But this is your journey and I need you to be as prepared and ready, as informed and engaged as possible so that we can do this together.
Ask questions. Learn. Satisfy your curiosity. Ask the what-ifs. Understand your risks. Understand what your role in this is. How can I improve my outcomes? What can I do to keep myself safe [during] treatment? What should I do with exercise? What about diet? What about sexual activity while I’m on treatment? How does it affect my life? What about work? How do I disclose this to people that I’m dating? All of this stuff. The questions that naturally swarm all of our brains.
We’re trying to understand this terrible thing that’s going on. If you don’t ask those questions, you’re doing yourself a disservice and you’re not giving your doctor a chance to do the right thing with you and for you. So my one piece of advice: ask questions.
Ask questions. Learn. Satisfy your curiosity. Ask the what-ifs. Understand your risks. Understand what your role in this is.
Dr. Siegel, TPS: One of my favorite questions that my doctor asked me was, “What’s really important for me to know about you to take good care of you?” And I told him, “I love being a mom, I love playing guitar, and I love running.” The lung toxicity [was] really important to me. Neuropathy, which is really important. Knowing that was a key part of knowing how to take good care of me because we watch out for nerve issues, for trouble breathing, and things that could really impact my quality of life.
Dr. Matasar: Sounds like a wonderful oncologist.
Dr. Siegel, TPS: Absolutely. Thanks so much for taking [the] time to chat with The Patient Story. We’re so lucky.
Dr. Matasar: It’s my privilege. There’s nothing more important than this piece of things. What we do is about our patients, their caregivers, [and] their loved ones. This is all it’s ever about so the opportunity to share my thoughts is an honor.
There are so many developments happening in multiple myeloma! While this is wonderful, it is getting harder to keep track of all the potential updates and changes for those living with and caring for a loved one with myeloma.
The Leukemia & Lymphoma Society (LLS) and The Patient Story bring you this program out of the biggest blood cancer/disease conference every year where top doctors and researchers discuss the most important updates (American Society of Hematology, or ASH) which took place December 2022.
Thank you to Karyopharm Therapeutics for its support of our patient education program! The Patient Story retains full editorial control over all published content.
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Stephanie Chuang, The Patient Story: I’m the founder of The Patient Story and I’m also a cancer survivor [of] lymphoma.
The Patient Story is co-hosting this program with The Leukemia and Lymphoma Society or LLS, which, as many of you already know, is an incredible organization with top resources to help guide you through myeloma — diagnosis, treatment, and everything in between.
We also want to thank Karyopharm Therapeutics for its support of our educational program. We do want to stress that The Patient Story and the LLS retain full editorial control.
Many of you are probably very familiar with Jack Aiello. He’s been living with myeloma for almost 30 years and even more incredible than that alone is for a lot of this time, Jack has dedicated himself to the research of the latest and greatest — what’s coming out in terms of the developments in therapies and the knowledge in terms of how to deal with myeloma — and he does this not just for himself but for those of you out there as well.
Jack Aiello: I was diagnosed with stage 3 multiple myeloma in early 1995, 28 years ago. At the time, I had been married for 20 years and had young kids — 16, 14, and 10 years old. I remember when the doctor told me that at my stage I was probably going to live for only two to three years, that was pretty scary. I didn’t know what to say to my wife. We shared a good cry and I remember talking to my kids and saying I had something wrong with my blood because I was going to be in the hospital for 96 hours. I tried to leave it at that. You try to protect your children as much as possible.
Ultimately, I ended up having a tandem autologous transplant — two autologous transplants about four months apart — but they only gave me a year and a half remission.
In late ’97, I started a clinical trial for thalidomide, which was really important to the world of myeloma because a third of the patients responded to that treatment. Unfortunately, I was refractory. I didn’t respond at all. My disease condition got worse as I was on it. I tried other chemos — they didn’t work.
I had one other available to me — in this case, [the] fourth line of treatment — called an allogeneic transplant, meaning that instead of using my own stem cells as was done in an autologous transplant, I used donor stem cells. It worked. It’s not done much today because even back then, there’s a 40 to 50% mortality rate just from the transplant. Today, we have so many other safer treatments that it doesn’t make sense to do. But it was the only option available to me back in ’98. And I haven’t been on any treatment now since the early 2000s.
Two things I did right. I found that we had a myeloma support group in the San Francisco Bay Area, where I live, and they helped educate me about myeloma and [the] questions I should be asking. The second thing I did that really made a difference was seek out expert opinions. Ultimately, I went to Little Rock, Arkansas, to go through most of these treatments. Back then and still today, Little Rock [is] a premiere center for treating myeloma patients so that made a huge difference for me.
Today, whenever I talk with myeloma patients, I always suggest that they get a second opinion from expert doctors and there are so many more available these days from around the world. I’m fortunate enough to be pretty knowledgeable about myeloma these days.
The top doctors and researchers from around the world meet [at ASH] to discuss the latest in blood cancers, specifically myeloma. Two of those doctors are joining our conversation today: myeloma specialists Dr. Josh Richter and Dr. Muhamed Baljević. Both are committed to seeing myeloma patients in their clinics and also furthering research to get us those next improvements in treatments.
We will be highlighting the summary of top takeaways in myeloma from the ASH conference for first-line therapy patients all the way through later relapse. The big buzz at ASH for myeloma patients was the word bispecifics. But before we go there, there was some update that could actually change treatment for some myeloma patients today. And it has to do with steroids.
Cutting back on the use of dexamethasone
Dr. Muhamed Baljević: There was an important piece of data presented in frail, newly diagnosed patients where we demonstrated that it’s possible to cut back on dexamethasone completely. This is really important for patients. We’ve all received these questions.
Glucocorticoids are not easy to tolerate with [a] multitude of side effects. In these frail patient populations where patients have multiple comorbidities — some may have diabetes, brittle diabetes that’s insulin-dependent — it’s really a success that we are presenting data like this, that we can show that it’s safe and feasible.
Quite frankly, even in my own clinic, I and many others are trying to see if we can pull back on the use of glucocorticoids long-term. Perhaps, in the beginning, there’s some bigger role but later on, would be lower.
What are bispecific antibodies?
Jack: Let’s go now into the big area of buzz — bispecific antibodies. Dr. Richter, can you help us understand what bispecifics are? We actually know about monoclonal antibodies like daratumumab. But what’s a bispecific antibody?
Dr. Josh Richter: People may be familiar with monoclonal antibodies like Rituxan or Darzalex. It’s got one arm, grabs onto the cancer cell, and kills it. Bispecifics have two arms and classically, right now, each of those arms does this one thing: one arm grabs onto our T-cells and activates them to attack the cancer [and] the other grabs onto the cancer cell. This arm that attaches to the T-cell attaches to something called CD3. It’s on all T-cells. That, for the most part right now, is the same. But the arm that grabs onto the cancer cell is different.
At ASH, we’re seeing presentations from four different other arms. BCMA, some people may have heard of. It’s the target of many CAR T therapies and a drug called Blenrep. Talquetamab targets something called GPRC5D. There’s another drug called cevostamab that targets FcRH5. There’s another drug that targets CD38, the same marker that’s attacked for Darzalex, but also using the T-cells, and that drug goes by the name ISB 1342.
Really excited about talquetamab because right now, the majority of our T-cell redirecting therapies [have] all been BCMA. We have two FDA-approved CAR T-cells. They both attack BCMA. We have one FDA-approved bispecific. It attacks BCMA. We had an antibody-drug conjugate called Blenrep. It was taken off the market, but there are two ongoing phase 3 studies — the DREAMM-7 and DREAMM-8 study — which will hopefully bring the drug back within the next year, year and a half. Fingers crossed.
Dr. Baljević: I personally think it’s a good drug and it’s an important drug for some subsets of patients. We learned that we will still be able to give that [to patients] on compassionate access. I think that’s important because not all patients will be eligible for CAR Ts and maybe even for bispecifics.
How soon will patients be able to start on bispecifics?
Jack: Let’s talk [about] real-world access for patients and caregivers. With all of the bispecifics, how soon are we talking?
Dr. Richter: Teclistamab was approved. We have started giving the drug. Commercially, it’s available. As opposed to a CAR T where there [are] limited slots because of production, this drug is available. But let me put a little caveat on that.
Right now, the way the drug is recommended to be given by the FDA is that you get several step-up dosings and this is done mostly inpatient. You have to be admitted to the hospital for about seven to 10 days. We can’t admit 30 patients at a time. Every institution is developing [its] own SOP of how many patients they feel comfortable with [in] a week. Right now, we have a list of patients that have been waiting and now that we’re giving the drug, we’re going through that list pretty [quickly]. My guess is that within the next couple of months, we will have gotten through that list and we’ll be able to say, “Okay, you’re progressing. You need the drug. You can get it.” It’s going to happen a lot faster than for CAR Ts.
When will bispecifics be available in Community Cancer Centers?
Jack: How about true availability? For instance, CAR T has been limited to certain sites, mostly bigger and academic hospitals. Will bispecifics be available for those of us getting care in the community?
Dr. Richter: That’s a really, really great point. The short answer is yes. Yes, it is, but it’s not going to be given in the community just yet. There [are] still pretty high rates of CRS. It involves admission. It involves some of the management strategies that a lot of these doctors are not as familiar with.
A lot of hematologist-oncologists out there are used to dealing with [the] side effects of classical chemo. Then they got used to dealing with the side effects of checkpoint inhibitors. It’s going to be a learning curve.
We’re willing to partner with the community. You come to us, you get that first inpatient dosing, get you through the risky part, and then get you back to your community to get your regular treatment.
What is cytokine release syndrome?
Jack: We hear a lot about CRS — cytokine release syndrome — as a side effect, especially when it comes to these T-cell therapies. Dr. Richter, can you share what it looks like in patients from low to high grade when they experience CRS and how it’s managed?
Dr. Richter: There’s a grading system. What does it mean? There is something called the CTCAE, the common terminology [criteria for] adverse events, and it grades everything from a grade 0 to a grade 5 — from stubbing your toe to a heart attack to CRS. Grade 0 is you don’t have it, 5 is you’ve died from it, and 1 through 4 is gradual worsening.
In clinical trials, we often look at grade 1, 2 as being the milder ones and 3, 4, the more serious ones. In general, grade 1 CRS is just some fever. You spike a little temperature. You feel fine. Your other vital signs are fine. You’re not having any trouble breathing [or] anything like that. For grade 1, you don’t really need to do anything. If it persists, you can start adding drugs like tocilizumab. For early grade 1, you could just give Tylenol if you want. Simple things like a little IV fluid [and] a little Tylenol will settle them down.
Grade 2 is where your pulse is getting a little faster or your blood pressure is starting to drop. If your O2 sats starts dropping, that’s starting to get into grade 2, that’s where we’re really coming at there with things like tocilizumab.
Then as we get to 3 and 4, that’s where oxygen is getting worse. You may even need more oxygen support, even getting to the point of being on a ventilator. Not very common.
Will bispecifics be given in the outpatient setting?
Jack: With that in mind, will bispecifics be able to be given in the outpatient setting?
Dr. Richter: There are already a number of people starting to give these completely outpatient. There are certain risk factors for higher-grade CRS. If you have a very high tumor burden, we know you’re more likely. If certain markers like your LDH are already cranked up or circulating plasma cells, we know you’re more likely to have it. If we have someone that doesn’t have all those risk factors, we could give it as an outpatient.
But there’s actually some data from another bispecific being presented at ASH that is going to make it more applicable to the outpatient.
Thoughts about patients needing hospitalization with bispecifics
Jack: For teclistamab, there is the initial two-step dose, then the third full-strength dose, all given at least 48 hours apart. Patients are then required to be in the hospital to manage possible side effects for at least a week. What are your thoughts about the requirement for patients to be hospitalized with bispecifics for the time being and the burden associated with that?
Dr. Baljević: This is really important because it’s really essential that we use this drug safely. The label is advising that inpatient admission and monitoring be considered for each of the doses in this step-up schedule, which is basically one, four, and seven — seven being the first full dose that they would continue with. Potentially, that does imply that people would need to spend nine days in the hospital.
There are a number of efforts that are going to be attempted to see what we can do. Can we consider doing some of this therapy in the outpatient setting, partially or maybe even fully? There’s also [the] possibility of having [a] slightly different step-up schedule of one, three, five with [a] seven-day admission rather than nine. Cutting back a little bit on the days spent [inpatient] has an impact on how hospital systems can deal with the costs associated with therapies and reimbursements for these therapies.
Really important period ahead for how this drug is going to be used in the broader sense in academia but also in [the] community importantly.
Dr. Richter: Cevostamab is another one of those bispecifics — CD3 to grab onto the T cells, something called FcRH5 that’s on all the myeloma cells. There [are] two presentations at ASH that I think in and of themselves wrap into a nutshell how we are likely to approach all bispecifics in the future. If you put them together, this is the blueprint.
We’re talking about CRS. We recognize that some people [are] going to end up in the hospital, have high grade, or get sicker. When you develop CRS, we give a drug like tociluzimab. What happens if you use it as a pre-medication? What happens if you give it before you even give the first dose? Can you mitigate or prevent CRS? And that’s exactly what they did for cevostamab. They took patients and they gave them a prophylactic dose of tocilizumab and it took the overall all-grade CRS rates from over 90% down to the 30th percentile. And that’s just the beginning.
People will just say, “Well, wait a minute. If we give toci, are we going to affect the efficacy?” For cevostamab? Absolutely not. We have not affected efficacy, but we’ve markedly reduced the incidence of CRS.
We’re all starting to talk about how we’re going to approach this. Should we consider giving people tocilizumab before we give them bispecifics, particularly for the people we worry may not tolerate it? 40-year-old, no medical problems? Not as worried. 80-year-old, [with] multiple comorbidities, may not be able to tolerate that grade 2 to 3? Consider giving them tocilizumab.
Dr. Baljević: I think that’s really interesting because we may yet use the findings of that cevostamab study to try to plan how we can reduce the incidence of CRS in other bispecifics and maybe even in the CAR Ts. A lot of interesting data [was] presented.
Limited duration treatment with bispecifics for relapsed/refractory myeloma patients
Jack: There is also research pushing towards the possibility of limited duration treatment with bispecifics for relapsed/refractory patients, meaning not having to continuously be on treatment. Can you share more about this?
Dr. Richter: The whole standpoint is [to] treat until progression or intolerability. We don’t stop therapy. It’s true for all the bispecifics, except cevostamab. This is fixed duration — 17 cycles, which rounds out the drugs every three weeks so it’s step-up dosing. It’s one year of therapy and then you stop.
We’re starting to see patients who’ve completed that and we’re monitoring them off therapy. In that trial, they have the option of being re-treated if they progress while they’re off [treatment]. We have patients greater than six months and we have a number of patients greater than 12 months. Patients completed a year of therapy and are now another year in complete remission, off of everything, and living their lives. If at some point the disease comes back, we come right back in with a drug that put them back into remission.
This gives us a number of advantages. Number one is obviously how patients feel. But there [are] two other big ones. One is something called T-cell exhaustion. If you give these drugs that activate the T-cells and you say, “Fight, fight, fight,” eventually they get tired. Maybe they’re getting tired [to the] point where you don’t need them and when you do need them, they’re not ready to go. Giving someone a break off the drug, those T-cells can recuperate and when you need them, they’re back ready to fight.
Dr. Baljević: [A] deeper understanding of T-cell function, T-cell exhaustion, and resistant mechanisms is needed and that’s where some of these other agents that have [a] positive impact in those situations can lend themselves even more useful. For example, selinexor is such an agent where some of the preclinical data has already been published and demonstrated maybe some of these roles.
Jack: Is the hope that other bispecific can also test this finite duration?
Dr. Richter: Absolutely. That is the big buzz when you talk with all of the pharma companies [at ASH]. Because why did cevostamab choose a year? We even asked them and they couldn’t give an answer, but I’ll give the answer. One year is a nice round number. It’s not a biological thing. It’s a nice round number. But what this is becoming thought-provoking for all the other bispecific manufacturers is to say, “We need to do this, but with a biological endpoint.”
For example, complete remission and then two more cycles and then stop or MRD negative and three more cycles. But right now, the big discussion is to not just pick a random number but to have a biological response. Right now, these are the big discussions in the halls of ASH: how do we design the next series of trials?
Who would qualify for bispecifics?
Jack: Remind us: who would qualify for bispecifics?
Dr. Richter: You can say patients who’ve had four or more prior lines. Another thing we talk about is triple-class refractory so refractory to a drug like Revlimid, a drug like Velcade, and a drug like daratumumab. Now we’re even going [to] the next step: also refractory to a drug like a BCMA drug.
What we know is once that gets those approvals towards the end, we start learning more. We move it further up. New combinations. There [are] already trials in bispecifics in one to three prior lines and a few that are on the verge of opening as upfront therapy. Very new, not a lot of people on them. We’re still trying to figure that all out.
Dara had a response rate of 30% in the end and when you give it upfront, in combination, it’s 100%. What happens when you take a drug that [has a] 70, 80% response rate in someone who’s had an average of six prior lines? If you move it upfront, do you cure some people? Do you get remissions that are so long [that] it’s a functional cure?
That’s why the myeloma world couldn’t be more excited right now. There is a combination out there and there are actually several discussions right now of cure protocols and cure goals.
What is the overall takeaway from CAR T-cell therapy?
Jack: Dr. Richter, what’s the overall takeaway so far on the CAR T-cell therapy front?
Dr. Richter: The CAR T front is that they work well in the later lines. If you move those further up, initially we were worried about more side effects because it’s all about the T-cells again. As you go through your therapy, those T-cells get tired. And when you give a CAR T or collect T-cells in someone who’s had a whole bunch of therapy, you’re collecting tired T-cells.
What we were worried about is if we collect early on T-cells that are more robust, maybe they’re going to give you more side effects, more CRS, [and] more neurotoxicity. That is not happening. That’s not the case. So we know that we can give these drugs early on, but some of the early data has been extremely encouraging.
The big question is: is it better than other therapies early on? Now, there’s a study called the KarMMa-3 study, which compared ide-cel versus an early regimen in relapse like dara-pom-dex. We don’t have the data just yet, but there was a press release to say that CAR T beat it. A lot of excitement about moving CAR Ts into early relapse.
Then there [are] two strategies right now about CAR Ts upfront. One strategy is comparing CAR T versus transplant and that’s a really interesting one but that’s not my favorite. My favorite is transplant followed by a CAR T with the idea of your induction [bringing] you down, your transplant [bringing] you down [further], and then immune therapy to sweep up what’s left. I’m hopeful that that might be a curative approach for some people.
How do you choose CAR T or bispecifics and in what order?
Jack: You were talking about how sequencing is going to matter but also in choosing which direction to go. For your patients, how are you going to decide or determine whether it’s going to be CAR T first and then you go to bispecifics or the other way around?
Dr. Baljević: That’s really important. We’re still learning how to recognize what the best patients are.
Personally, if I have a patient that can receive CAR T therapy and I’m in a position to give them CAR T therapy, preferentially, I probably will do that. Though we now have a first agent that’s bispecific and off the shelf by definition. We are expecting another number of agents in 2023, maybe Q2 — maybe one targeting BCMA or another one targeting GPRC5D for the first time. I think that both are associated with some of the serious side effects.
Autologous CAR Ts are associated with some requirements for generation and synthesis. Patients that are relapsing and have diseases with velocities that are pretty aggressive and whose proteins are rising rapidly, whose counts may be changing, or whose kidney functions, mineral levels, and calcium levels might be threatened, may not be the best candidates for those types of therapies. They’re better candidates for off-the-shelf therapy. That doesn’t only include BiTEs, but it may also include allo-based CAR T cells off the shelf.
Dr. Richter: It’s all in context. If you look at some of the drugs like dara [with a] 30% response rate at six months or so in heavily refractory, we use it upfront.
The MAIA regimen — dara-rev-dex — for elderly, transplant-ineligible patients, the average remission upfront is greater than five years. What does that look like with CAR T? We’re still trying to figure that out.
Let’s say the two are equivalent. Giving someone standard therapy or CAR T, there [are] risks and benefits. CAR T, you have to be admitted; standard therapy, you don’t. CAR T is a one-and-done; standard therapy, you have to continue on. CAR T is usually something that we reserve for the younger and fitter. If you’re older [or] frailer, the other direction may be the way to go. But the other question is until CAR T is a one-and-done cure, we’re trying to improve remissions. There [are] a number of studies looking into maintenance after CAR T.
Updates on CELMoDs
Jack: Were there any updates on CELMoDs?
Dr. Richter: These drugs, just like Revlimid, worked in people who had thalidomide and pomalidomide worked in people who had Revlimid. These drugs work really, really well in people who’ve had the others.
Iberdomide, for example, is one of the most potent ones and it has a lot less in terms of what we call myelotoxicity — it doesn’t lower your blood counts as much. If you wanted to strategize an optimal maintenance drug, it’d be a drug that someone’s going to tolerate very well and not lower their blood counts, especially after something like a CAR T where your counts may be lower.
These CELMoDs are really going to be a big part of our therapy. We probably have to wait till 2025 [or] 2026 for regimens like Velcade-iber-dex and dara-iber-dex. But some push to consider those drugs in earlier lines. There [are] a number of great drugs on the horizon.
What role do ‘novel therapies’ play?
Jack: What role do the more recent novel therapies play now?
Dr. Richter: Right now, if you look at CAR Ts and bispecifics, it’s patients who had at least four lines of prior therapy. If we’re giving dara-RVd upfront and you’re getting car-pom-dex in your second line, you’ve got a gap in there. Now, that gap is very important because if you’re going to collect T-cells, if you’re going to collect CAR T, you can’t give a drug that kills T-cells.
For example, bendamustine is a drug that a lot of people had been using in that line. Bendamustine is a great lymphoma drug. It kills lymphocytes. So if you give benda and then you try to collect CAR Ts, you will fail. Selinexor is an excellent drug so we’ve been using a lot of it there to help bridge the people to get them to CAR T.
Understanding what dose is best for selinexor
Jack: Dr. Baljević, speaking of selinexor, you presented additional details on using this drug weekly instead of twice a week, providing efficacy with fewer side effects. Both the STOMP and BOSTON trials used this lower selinexor dosage in combination with carfilzomib and Velcade respectively. Can you expand on this topic?
Dr. Baljević: We are shown the value of selinexor as an agent in this difficult-to-treat population. Earlier, we were talking about the outcomes of high-risk patients. Anybody who is triple-class refractory, even if they’re not harboring high-risk cytogenetic features, they are, biologically, already in a place where they have progressed on multiple good therapies. We know from previous large-scale analyses that these patients have short, medium progression-free survivals and survivals that are measured in single-digit outcome endpoints.
What we did is looked at the patients that were exposed — and some of which were actually refractory to CD38-based therapy as well — and we looked at what type of outcomes they can have with selinexor-based, importantly, weekly treatments. A lot of investigators still have angst using selinexor twice a week. I agree with that. I have never given anybody selinexor 80 mg twice a week. These are active triplets with Kyprolis and dex, with Pomalyst and dex, [and] even with Velcade and dex so BOSTON data phase III was [a] positive report. But particularly with the second-generation PIs (proteasome inhibitors), and IMiDs, Pom, and Kyprolis, these are powerful triplets that are effective in this difficult-to-treat population.
It’s going to be really important for us to try to understand: what is the best way for us to try to utilize agents with [a] different mechanism of action? How are we going to treat patients who are triple-class refractory and BCMA refractory potentially? A lot of these agents are being brought in early.
KarMMa-4 [and] CARTITUDE-5 are exploring the use of CAR T as a part of the first line. CARTITUDE-4 is going to be looking at cilta-cel versus two different standard of care options: PVd versus DPd. Some patients will potentially be treated in the second line with powerful agents. So what do you do with those patients? Well, we don’t know. We’re just generating that experience. We need agents with [a] different mechanism of action, that we can rely on that can actually treat this difficult-to-treat patient population.
How do we include more diverse populations in clinical trials?
Jack: Wonderful. We are seeing diversity, equity, and inclusion more and more, addressing the need to make sure that we are more inclusive of different populations. What can pharma, doctors, and patients do to increase diverse populations in clinical trials?
Dr. Baljević: This is such an important question. We are not doing such a good job in [the] myeloma field as myeloma specialists accruing minorities and disparities. We have data on that.
For example, [the] African-American population is still being accrued in the single digits on clinical trials so that’s a problem. And some of the other disparity populations as well. Where I practice and where I am in charge of the program, that’s really a programmatic goal for us to try to do better and increase disparity accruals on clinical trials.
In fact, we have a grant with LLS. [The Leukemia & Lymphoma Society®] is really an amazing partner in so many areas and they’re supporting [the] increase of awareness and access of patients from the community areas, especially those that are underserved geographically. We are partnering successfully with colleagues in the community, trying to bring patients, and increase access to good quality clinical trials for hematologic malignancies in general, including myeloma.
We need to do a better job. That really needs to be a goal of every single myeloma physician. Hopefully, in the future, we’re going to see more trials that have more balanced accruals in terms of different ethnicities [and] different disparity populations in particular.
Dr. Richter: When I started this and people were diagnosed, I said, “We can’t cure this disease. I’m very sorry.” Today, we cure some people. [It’s a] small number and I will admit it’s by accident. We don’t know that we did something extra special for that particular person. The next generation is intentionally curing more with the goal of intentionally curing everyone and we have the pieces to start getting closer and closer to that.
Conclusion
Jack: Thank you to Drs. Richter and Baljević for joining this discussion about the latest in myeloma treatment as we head into the new year. There was an incredible amount of myeloma information at the recent ASH meeting and you’ve helped distill it down for patients to be able to understand. Patients, thank you because all of this information comes your way and is important for your own education and enabling you to be your own best patient advocate.
Stephanie: Thank you, Jack, for leading this discussion. Thanks again to Drs. Richter and Baljević for such a rich discussion. There’s just so much to know about in the space of myeloma. Thank you again for joining us.
Follow-up questions
January 2023
We asked Dr. Richter to help answer some of the pre- and post-event questions submitted. Unfortunately, we could not address them all, especially if they were too individualized, as our specialist cannot provide you with personalized medical advice.
This is not meant to be medical advice or replace information from your own medical team. Please consult with your doctor and medical professionals before making treatment decisions.
General
Based on the ASH conference, are any changes to the NCCN guidelines in myeloma therapy likely to occur? Any new information with regards to treatment for patients with multiple myeloma with plasmacytomas?
The NCCN meets regularly to discuss and implement changes. Changes can occur from new manuscripts, trials, conferences, etc. as it’s an amalgam of all of this. I’m not sure that there are any changes planned at the moment.
Plasmacytomas can be thought of in two ways.: solitary plasmacytomas and plasmacytomas associated with myeloma. In the first one, radiation offers the potential for cure. In the second one, you can use chemotherapy and/or radiation to control them. Nothing really new about them from ASH.
Treatment response
What treatments will have the best outcomes for high-risk patients, specifically del 17p?
We don’t really know this just yet.
Why do some patients not respond at all to the gold standard of Revlimid (lenalidomide), Velcade (bortezomib), and dexamethasone?
We often don’t know this as well. There is extensive work regarding the role of cereblon in patients who do or don’t respond to Revlimid.
What is the average length of time a drug regimen works before having to switch to a new one?
This is different for everyone and highly variable. That being said, it tends to be longer in earlier lines (i.e. The first line lasts longer than 2nd line than 3rd line, etc.).
If a patient doesn’t do well on chemo and is transplant-ineligible, what is gold standard for next steps?
There is no universal answer. We decide therapies based on three main factors:
patient-related factors
disease-related factors
treatment-related factors
There is no “gold standard,” and there are oftentimes multiple options with different risks and benefits.
With all of the new developments, has the length of life increased? We were originally diagnosed 3 years ago and told the average lifespan is 7-10 years. Is it still accurate?
The length of life is certainly increasing. The most up-to-date data is listed on the SEER website.
However, as you will note, the data currently looks at 5-year survival rates for patients from 2012-2018 as it has not been 5 years since 2019. We really don’t know the rates of a patient diagnosed today. But they continue to improve. Unfortunately, those with high risk and more specifically ultra-high risk are not seeing the same degree of benefit.
Side effects
Multiple myeloma affected my kidneys to the extent that I had to begin dialysis. I had a stem cell transplant in 2018. Are there any new treatments to help with this reversal? I have the urge to urinate only.
Myeloma can affect the kidneys in a number of ways. Some are reversible, and some are far less reversible. In general, the longer one remains on dialysis, the harder it is to reverse the kidney damage.
How to overcome side effects from multiple myeloma chemotherapy? Weight, neuropathy/tingling feet, tiredness, or agitation.
Best to discuss this with your care team. There are a number of strategies, but they need to be individualized to you, your treatment, and your myeloma.
Had BMT, in remission, feeling great, but no libido. What did it? The cancer, chemo, radiation — all of it. Can’t use Viagra and mainly have no interest. I was not like this pre cancer.
Therapy can lower testosterone levels. Consider checking them in consultation with a urologist.
Transplant
My 35-year old husband was diagnosed in 8/2022 and will be undergoing an autologous cell transplant in January and an allogeneic stem cell transplant in March. Advice for recovering from transplants?
Eat well, sleep well, and exercise. Basic tenets of life will help before, during, and after transplant. The other strategies should be discussed with your care team and be individualized to you.
What are my treatment options if I can’t get another bone marrow transplant in a new relapse?
There is no universal answer. We decide therapies based on three main factors (patient-related factors, disease-related factors, treatment-related factors). There is no “gold standard,” and there are oftentimes multiple options with different risks and benefits.
CAR T
One side effect of CAR T-cell therapy is a depleted immune system and extremely low IgG. This seems much more serious than its current explanation. How serious is this?
CAR-T can lead to immune suppression in a number of ways. Many of them recover with time. IVIG is a good strategy to augment your immunoglobulins during this time.
Can the CAR T-cell therapy be repeated after, or is it a one-time treatment?
Patients can be treated with more than one CAR-T, albeit this is not a common occurrence.
What results have you seen with patients that have had a second CAR T that targets BCMA?
There is limited data looking at patients who receive a 2nd BCMA CAR T. The outcomes are extremely variable and depend on a lot of things, such as how long was it in between your CAR T’s and what is the nature of your relapse.
Bispecifics
Is teclistamab being administered out there in community hospitals and clinics yet? How is it doing?
So far the overwhelming majority of teclistamab is in academic centers as the FDA approval recommended inpatient admission to the hospital for the initial step-up dosing. It will take time to roll out in the community.
How many deaths “approximately” have there been caused by bispecific clinical trials and treatment?
There is unfortunately no way to answer this for a large number of reasons, apologies.
MRD
What would constitute MRD positive/negative in numbers, if possible? For example, M-spike = 0 for how long, abnormal plasma cell population percentage of WBC, and what else is relevant?
MRD evaluation is independent of M-spike because the M-spike measures a protein and the MRD test measures the actual cell. MRD can be assessed by a number of different methods, with the two leading methods being next-generation flow cytometry (NGF) and next-generation sequencing (NGS). The positive/negative parameters are set by the technology and the number of cells analyzed.
Second cancers
What are the prevalence and treatment considerations for patients with relapsed/refractory multiple myeloma (RRMM) that develop myelodysplastic syndromes (MDS)? Are there clinical trials in our area, and if so, how do you find out about them?
MDS is an uncommon but known entity in patients with RRMM. The treatment options are individualized for MDS, just as they are in myeloma. Options include therapies like the hypomethylating agents and even drugs like lenalidomide.
Trials for MDS in RRMM patients may be complicated as many trials exclude patients with other malignancies. Always best to discuss with your care team about the options. Clinicaltrials.gov lists all trials and oftentimes includes the inclusion and exclusion criteria, as well as a contact for the teams running the trial.
Which myeloma drugs/treatments cause increased prevalence of melanoma?
In general the answer is none. Myeloma itself can increase the risk of non-melanomatous skin cancers. Melanoma is a rare occurrence in patients with MM. That being said, drugs like lenalidomide can increase the risk of a 2nd cancer such as melanoma.