Watch an empowering patient event and discover the latest advancements in non-Hodgkin lymphoma care, including Diffuse Large B-Cell Lymphoma (DLBCL) and Follicular lymphoma.
Thank you to Genmab, AbbVie, and Incyte for their support of our patient education program! The Patient Story retains full editorial control over all content.
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Learn Through Non-Hodgkin Lymphoma Patient Stories
Stephanie Chuang, founder of The Patient Story, celebrates five years of being cancer-free. She shares a very personal video diary with the top lessons she learned since the Non-Hodgkin lymphoma diagnosis.
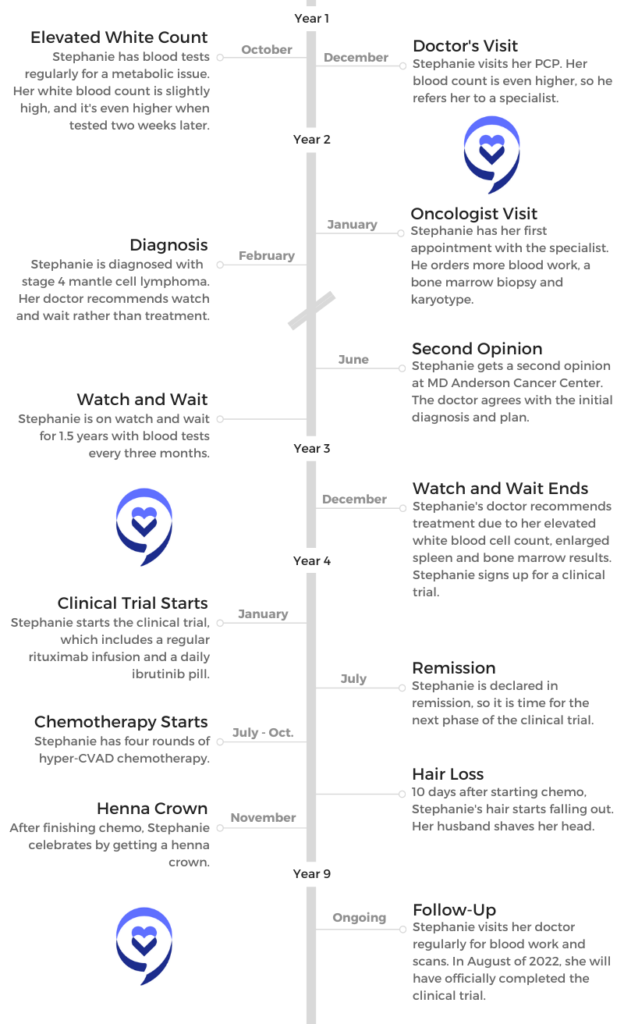
Cancer details: Characteristics of both subtypes 1st Symptoms: Lower abdominal pain, blood in stool, loss of appetite Treatment: Chemotherapy (Part A: R-CHOP, HCVAD, Part B: Methotrexate, Rituxan, Cytarabine)
Barbara’s Stage 4 DLBCL Non-Hodgkin’s Lymphoma Story
After beating breast cancer 20 years ago, Barbara was alarmed when faced with having cancer again, this time with stage 4 diffuse large B-cell lymphoma (DLBCL).
She shares her journey of first symptoms, sharing the news with her family and granddaughters, and undergoing treatment.
You can read her in-depth story below and watch our conversation on video. Thank you for sharing your story with us, Barbara!
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
VIDEO: 1st Symptoms and DLBCL Diagnosis
Introduction
Tell us about yourself
I’m 72 years old. I had breast cancer 20 years ago. I’m a really active person and avid gardener, and I sailed for 42 years. I have 2 little granddaughters, lots of friends and family, and a wonderful husband.
What were your first symptoms?
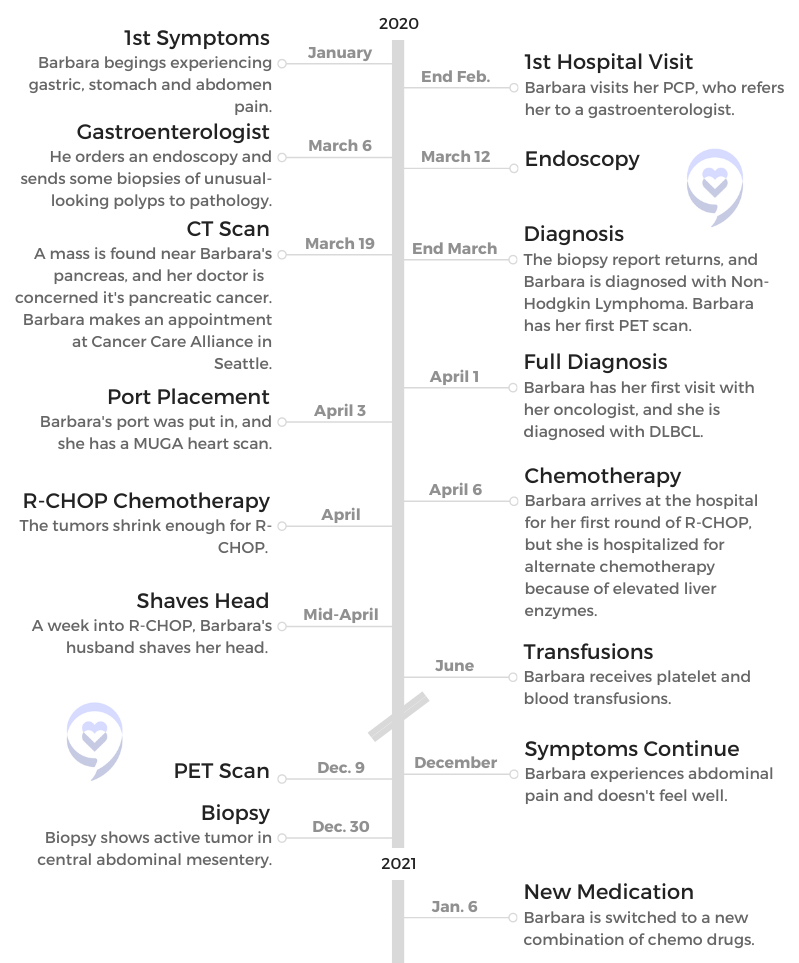
They were gastric pain, stomach pain and abdomen pain. I brushed it off. I thought, “It’s just acid stomach. Whatever I ate isn’t agreeing with me.” I had some other health issues going on at the same time, so it just got set on the back burner for probably too long.
Finally, I went to my PCP doctor, who referred me to a gastroenterologist to get to the bottom of it because it was really increasing worse and worse to the point where I couldn’t get in a comfortable position. It just went beyond a stomach ache, so I knew something was wrong.
How did your gastro specialist communicate the results of your endoscopy and biopsies?
I think it was right after the endoscopy. He said, “Everything went fine. I did see a polyp that I biopsied. It’ll take a few days, and I’ll get back to you.”
I thought, ‘Okay, I got through the other cancer. I’ll just get through this one.’ I was just sort of ready to take it on because that seemed like the only choice I had.
Apparently, it took more than a few days, but he was concerned because he ordered a CT scan after that, and there was what looked like a mass on the head of my pancreas. That was alarming enough to call me and say he suspected pancreatic cancer, which alarmed me and my family.
I decided I needed to go to a good cancer center. I called Cancer Care Alliance in Seattle, and I set up an appointment and a team for the pancreatic cancer. Then just a few days before my appointment, that gastroenterologist called and said, “Since we have the biopsy report, it’s not pancreatic cancer. You have non-Hodgkin’s lymphoma.”
The DLBCL Diagnosis
How did you process the possibility of having cancer again?
I was alarmed. I knew the severity of pancreatic cancer, and I just wanted to get into treatment right away the next day. The Cancer Care Alliance actually pushed me right into the system, and then as soon as they found out that it was a different diagnosis, they switched me to the hematology department.
I was not totally unhinged. I thought, “Okay, I got through the other cancer. I’ll just get through this one.” I was just sort of ready to take it on because that seemed like the only choice I had.
Receiving the DLBCL diagnosis
The oncologist that they set me up with at the cancer center ordered a PET scan before I even saw him. Just a couple of days later, I had my appointment with him. He went over what the cancer was.
It was stage 4, but you can treat that blood cancer at stage 4. He also went over the R-CHOP. “This is what we’re going to do first.” I just got it in my head that okay, we’ll do this.
For one thing, I knew that was probably the best cancer center in the Seattle area. My daughter-in-law had worked with them for quite a few years in the hematology department, and she was confident. She said, “This is the place you need to be,” so I didn’t really question that.
Treatment options for DLBCL
It was more or less, “R-CHOP is the way to go. This is what we do. We start here.” He didn’t say that this was the only option. He just said this is where we’re going to start.
I was just accepting the diagnosis and treatment, and I was confident I was in good hands.
Emotions From the Diagnosis and Treatment
How did you break the news to your family and friends?
My husband was with me for the appointment, and I believe my daughter-in-law was on speakerphone. She did that for my first appointment. I have a small family, just a son, his family and my husband. I have a brother, and my husband has a brother. We waited for a while to discuss that with them until we knew more about what everything entailed. I didn’t want to alarm everybody. With my friends, I didn’t go into that for a while.
There’s always fear about an invasive procedure. I’ve been through it before with my breast cancer. I’m a really calm person. I know it’s hard, but my advice is just to try not to be overly anxious.
They give you painkillers. It’s really a fairly easy procedure. It’s right under your skin and doesn’t take long, so I didn’t have a problem with it.
What was your reaction when they said R-CHOP was too dangerous because of your elevated liver enzymes?
That actually was scary to me. My husband had dropped me off. It was going to be a long day. We live about an hour away, so he was going to go home. When they told me they had to hospitalize me, it was almost a panic reaction, which I never do. But I had no car. I had no bag with anything I needed for the hospital.
I wasn’t prepared mentally for that at all, and COVID was really strong then. Nobody wanted to be in the hospital. It was scary. They assured me, “We have our own ward. There’ll be somebody right there to take you,” which all was true. They arranged for me to have a ride, but there was just that moment of panic. They were putting me in the hospital. I wasn’t mentally prepared for that at all.
How did you get through the isolation and hardest moments?
The hardest times were felt by everybody. Everybody was isolated in the beginning, so I didn’t feel like I was affected any more than anyone else. As the months went by, especially when people got their COVID vaccines, I was told that my immune system might not react well to the vaccine. Then I started feeling more isolated.
My husband did all the grocery shopping and did all the errands. Actually, to some point, it’s still that way. I have gotten a second set of COVID vaccines and Evusheld prophylactic shots, which makes me feel a lot better.
I did see my immediate family. My daughter-in-law was vaccinated right away because she worked in healthcare. I just had the few people, after they got their vaccinations, whom I would see but not in public places.
DLBCL Treatment and Side Effects
How did your first cycle of treatment go?
It was alternate drugs that they had abandoned because R-CHOP was better. But since they couldn’t do it and the side effects meant they had to watch more closely, that’s why they hospitalized me. I think I was there a week.
The one thing that bothered me more than the first time was my little granddaughters, because it’s hard to hide what is really going on with Grandma.
What were the side effects of R-CHOP?
I experienced nausea. Then I got the nausea pills down so that I knew when to take them. It just takes experimenting, and I think it’s different for everybody. That took a while. I remember getting dehydrated and having to go to the clinic for a fluid IV. There were rough spots with the nausea and vomiting.
Once that was under control, my appetite went down, but I did eat. Then I think as far as others, I had a side effect with skin flaking. I don’t know if anybody else has had that, but it was just extraordinary dry skin. I’d never experienced anything like that. I was taking oil baths, and then it just went away. I’m sure that was a side effect, too. But other than the nausea and getting that under control, I think I did okay.
It started looking dry and ugly, and then it was just hairs on your clothes and on the couch. I said, “Okay, let’s just get rid of this.” Since I had gone through it before, it wasn’t so traumatic. It was in the spring and summer, and I had a lot of really nice hats.
The one thing that bothered me more than the first time was my little granddaughters, because it’s hard to hide what is really going on with Grandma. At one point, I was taking care of them, and they had some little princess wigs.
I said, “I want to try one of your wigs.” I took my hat off, and they hadn’t seen me bald before. The little one was a little alarmed. I said, “I look pretty good in your wig, don’t I?” They started laughing and we had a good time, so we got over that.
As far as my friends and my family, I was embarrassed in front of them. The thing about losing your hair that bothers me is that it seems like it takes so long to grow back! When I was ready for it to grow back, I just wanted it to grow back. But it’s not overnight. It takes a while.
I think my daughter-in-law handled it best. If they asked a question, we would answer. They would stay all night with us once in a while. It was just kind of common to say, “Grandma’s got to lie down.”
Kids are not focused. They’re focused on themselves: when they can go play outside, if the sun’s out, what’s for dinner and can they have a treat?
We didn’t go into any details. They knew that their mother worked at a cancer center and that I was going to that same cancer center. They were 4 and 6 when I got sick, and they didn’t ask a lot of questions. We didn’t go into any details unless they did.
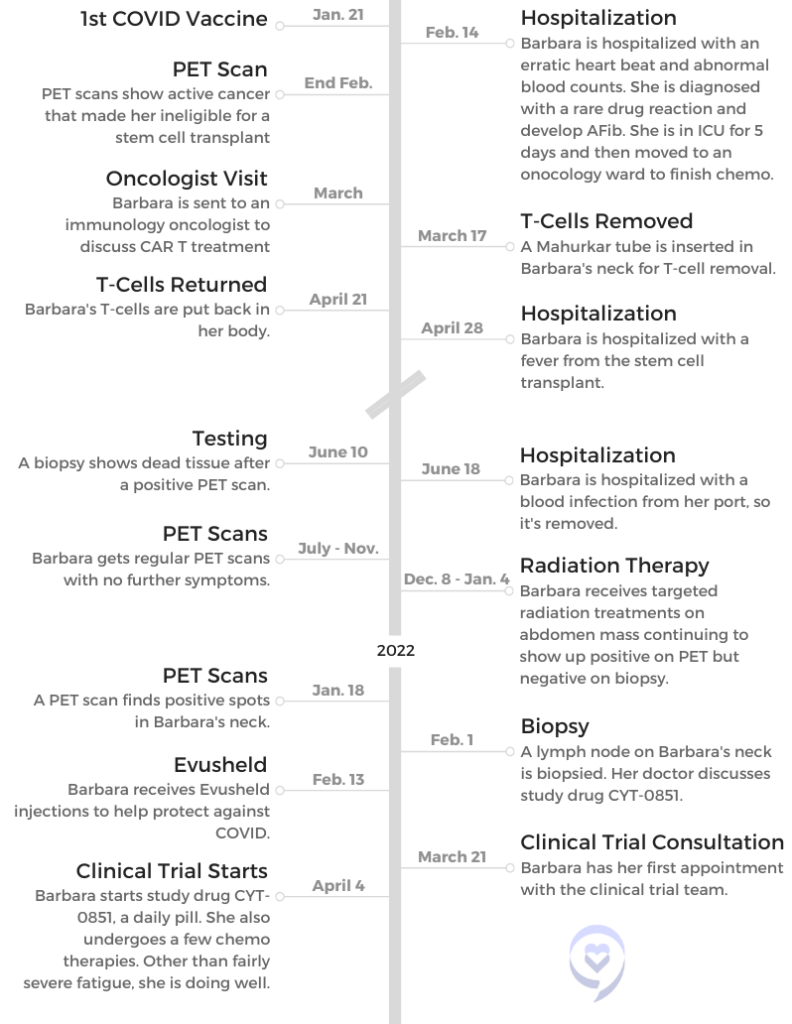
In December, a PET scan and biopsy showed an active tumor in your abdomen. How did you react and process this?
My oncologist was doing periodic PET scans. In December, I started again feeling abdominal pain. At first I thought it was just stomach cramps. I knew better. I just didn’t want to deal with it.
Then when the PET scan showed that it was positive there and that we needed to try another course of treatment, I guess my biggest reaction was disappointment. I was just really disappointed. I wasn’t losing hope, but on the other hand, the reality of things kind of hit me.
What did your hematologist-oncologist say was the next step?
They thought the next step would be stem cell transplant, and they gave me some chemotherapy. They do that before stem cell. There are protocols with getting a stem cell transplant, and you need to be actually cancer free before you do get the transplant.
I didn’t reach that goal, so they offered me the CAR T, which they were actually more enthused about. It’s just that the medical community and insurance want you to go through stem cell transplant first. Since I didn’t qualify, my doctors were excited that they could offer me the CAR T.
CAR T-Cell Therapy
How did your doctor explain CAR T to you?
He described it pretty thoroughly, and I did have some background in hematology. I was a laboratory medical technician for my career, so I understood T-cells, antibodies, the basics of blood cells.
It made sense. It seemed astronomical that they had come up with this solution, all the studies and the work that went behind it. The whole idea of it was pretty amazing.
Actually, the same cancer center has a Fred Hutchinson Research Center, and they were heavily involved in CAR T. Jeff Bezos actually donated the money for the CAR T suite and their own doctors. I sort of left the care of my regular oncologist, and I was now in the care of the CAR T research scientist oncologist.
First of all, they go over side effects very thoroughly, which is a little bit scary because there can be some life-threatening side effects. The fact that we lived more than an hour from the hospital required us to live closer, and it was quite an expense to rent an apartment in Seattle for a month.
You had to be 15 minutes from the hospital — which would have been University of Washington — because as soon as you get a fever, they want you there right away. It’s life-threatening.
I think it was like 100.3 or something. I can’t remember exactly. It was what you would consider a low temperature, but if you got that temperature, you’re in the emergency room. That happened, and I spent a week in the hospital there. They closely monitored me. Of course, that’s after I got the T-cells.
Removing cells
I need to back up a little bit to the process of removing your T-cells. They can do it with veins in your arm if you’re young, healthy and have huge veins in your arm. Unfortunately, I didn’t.
They put a tube in your neck, which again, was a procedure but not a really painful procedure. It was short. It didn’t take long. All I can say about it is it was awkward, because you’ve got this tube sticking out of your neck. You have to have it there like overnight. I just slept on the couch with pillows propping my head up and managed to get some sleep.
It’s sort of like a kidney dialysis, where they transfer your blood through a machine. They actually take your blood cells out, they go through a machine, it removes your T cells, and then it puts your blood back in. It’s an all-day process.
The nurse that does it is highly trained. It’s a complicated process. I didn’t have any problem with it. It’s just that it took a long time, and you were hooked up to this machine so you couldn’t leave. I think they did bring me a bedside commode at one point, but it’s not like you can get up and go to the bathroom or anything.
Returning cells
Then it takes quite a few weeks. They sent my cells to New Jersey, where they were processed. I think it took quite a few weeks. I can’t remember exactly, like at least 4 weeks. Then they came back. It’s just a little tiny bag, and they put the cells back in.
It’s just an easy process there. They had removed the tube in my neck. They put it in the afternoon before removing my cells, so that’s why I had to come home with it. Then the next day, they just took it out. For putting the cells in, it was like an IV drip, a little tiny bag.
It was at least 6 hours to remove the cells. Receiving the cells back was maybe half an hour. It was no time at all.
Maybe it won’t change anything. Maybe it will. So I went ahead and did it.
Aftercare
After you receive your T-cells, you need to be within 15 minutes of the center for a month. You see the CAR T team Monday through Friday during this time, and they do vital tests and COVID tests once a week.
They did a mental cognitive test and asked how I was feeling. They were short visits, but they wanted to see you in person.
For the mental cognitive test, you wrote the same thing down every day. You’d think I would remember that, but I can’t. You just wrote the same thing every day. You could see it written, and you had to write underneath the same phrase.
Hospitalization for fever
We were at our apartment, and my husband was just fanatic about checking my temperature. He said, “We’re going.” Arrangements had been made for when I got the temperature, and it all went really smoothly. They put me up in the oncology ward at the hospital.
While I was in the hospital, I had a couple of days of chills. I think my temperature probably got higher there, because I remember the chills really bad, and they subsided. They did keep me there for 7 or 8 days.
They monitor you very closely. It’s a little boring to be in the hospital for 7 or 8 days when I didn’t really feel that bad once the chills and the fever went away. It was comforting to know that they were watching me that closely.
Your PET scans were returning positive, while your biopsies were returning negative. What was going on?
The doctors were wondering what was going on. They couldn’t give me an answer. They couldn’t give themselves an answer. Apparently, the CAR T oncologist said, “Sometimes you can get a false positive with CAR T.”
It’s a fairly new cancer procedure. They don’t know everything about it, and they admit that. They were a little hesitant.
I think I had 2 biopsies. I was feeling fine, and I couldn’t even feel what was still positive. At one point, my doctor said, “Let’s just see in 6 months.” I was thinking that’s great, but then he called just before Christmas and said he just couldn’t get it out of his mind.
He was a little concerned and thought, “What if I’m not doing the right thing?” He and his colleagues had spent a lot of time thinking about it, and they decided that I should go through radiation therapy for the month of December, which kind of ruined my Christmas plans.
I was disappointed again, and he gave me a choice. “This is just how we feel about it. It’s up to you.” I kind of don’t like when they do that because those are hard decisions.
My husband and I talked about it. We thought if they are wondering and worried, then it kind of makes me feel the same way. Like he said, maybe it won’t change anything. Maybe it will. So I went ahead and did it.
He didn’t have any answers because they were confused about the biopsy report compared to the PET scan report. They were just trying to cover all the bases.
What went into your decision to get radiation therapy?
I just wanted to get on with my life. On the other hand, I thought, “I don’t want to just shorten my life. How do I know?” We just don’t know. I tend to be more cautious. We did discuss it. I think my husband and I made the decision that night.
He was getting worn out driving me to Seattle every day, because we needed to get in the commuter lane and it was winter weather. Oh my gosh, we just didn’t want to do that. We just knew the possible consequences versus maybe no consequences. It was hard to do.
How was your experience with radiation?
The worst part was actually getting there. Like I said, it was winter, and traffic in Seattle is not pleasant. We’re north of Seattle. As far as the radiation, you just get on a table, they line you up, and it doesn’t take long at all. Because it was in my abdomen, I had side effects like diarrhea. Again, I dealt with that with the anti-diarrheal medicines, but that was a little unpredictable and unpleasant. I also got fatigue from that.
How did you deal with the anxiety of waiting for results?
I think it was harder on my husband, to tell you the truth. You just kind of picture yourself where things are fine. And then all of a sudden, you’re picturing yourself like, “This is it.” It’s like a teeter totter. You’re down, you’re up, you’re down, you’re up. It’s like you just can’t seem to be in the middle.
I’m a realist. Tell me everything. I can handle it. If it’s going to be this way, it’ll be that way. But I do set myself up for the worst. My husband says I need to be more of an optimist. I always have a plan B, but C-D-F plan — how many plans can you have?
I wasn’t too surprised. I just thought, “I’ve been through all these things.” Then I got the impression this is at a simmer. Let’s just try to keep everything at a simmer. It’s the whole attitude of my oncologist and my daughter-in-law, who’s an oncology nurse. It’s the realization that possibly that’s all they can do. That’s okay. We’ll just see.
They did a PET scan after the biopsy. Actually, I got that PET scan result from my radiation oncologist because I had a Zoom meeting set up with her for a month after my radiation. We had both gotten the report at the same time. It was on my MyChart.
She had just seen it. She told me that actually there were multiple spots all through my abdomen of positive lymph. That’s when my oncologist gave me some options for further treatment, and one of them was a study drug.
What options did your oncologist offer?
One of the options was a repeat CAR T. He says it’s not like the original CAR T. Then he offered me the study drug that he did. I think there was one other. I can’t even remember it.
With the CAR T, I just didn’t feel like my husband and I had the strength to go through all that again and rent another apartment. We decided together that we’ll try the study drug, and my oncologist said he was guardedly optimistic. That’s better than, “I’m sorry. I can’t offer you anything.”
The study required another biopsy, which I just had yesterday on the lymph gland. I imagine it’s going to be the same as the one I had in February, and then I think that they’ll do a PET scan in June.
Clinical Trial
Clinical trial process
There are 7 chemotherapies once a month. I’m going to have my second one on Monday. There’s lots of blood drawing for the study, like timed blood draws. There are a lot of things that aren’t really the therapeutic side of the treatment, but more the study side, which I’m willing to do.
I’m having a hard time with that because I just feel like I’m a shell of myself.
The blood draws are tests that the study needs to do after the chemotherapies. That sort of thing. I do get blood tests where they monitor my red cells that my oncologist sees — my chemistry test, my kidney, liver function, all that. My doctor keeps tabs on that. The rest of the blood tests go to the study.
There’s once-a-month chemotherapy, and then you take a pill every day. You have to fast 2 hours before the pill and 1 hour after.
How do CAR T and the clinical trial compare? Do you wish you would have done CAR T again?
I don’t really wish I had done CAR T again. This gives me more freedom: the pill every day, the once-a-month chemotherapy. It’ll be 6 months or 7 months, so I need freedom in my life right now. I just need to not be so tied down to cancer.
I feel like hopefully it could work, but if it doesn’t, at least I got some freedom to live a life. It’s really hard when you’re just tied to a cancer center constantly. It takes a toll on my husband with all the driving and the waiting.
We’re in our 70s. I’d have a completely different attitude if I was 20 to 30s. I feel like whatever happens, happens. It’s been kind of a long haul, but I’m just hoping that maybe my experience is like a handbook to somebody else.
None of the procedures they do are really painful. I got a blood infection from the port, and when they took that out, that was painful, but it was because it was so infected in that area. But all the other procedures I had, I really didn’t have a problem. I had to have one therapy for weeks and IVs and all that. But you just get through that kind of side effect.
Continuing to Live Life
Dealing with extreme fatigue
I’m having a hard time with that because I just feel like I’m a shell of myself. I have a greenhouse. I walk out there. I’ve planted seeds. I have a chair out there I sit in. It’s just not who I am. That’s the problem. It’s not who I am. I’m just trying to cope with the fatigue.
You just want to make the best out of everything, no matter what it is. At some point, we all have to face an inevitable. But just that the life you led is the best one you could have done, even if you were sick at the end.
My red blood cell count’s low from the chemotherapy, they said. I’m hoping they can help some way to get me a little more energy. I push myself. I really do. Otherwise, I think if you didn’t push yourself, you would just be in bed all day. I can’t do that. I feel better when I push myself, and then I take a nap.
It’s springtime here. That helps. Everything’s blooming and growing, so the garden helps my spirit. Even though I can’t take a walk like I used to, even if I walk around the yard, it’s like I’ve done something. I’ve looked at something that made me feel good.
We did hire a housekeeper because you can’t keep your own house up, and my husband’s doing everything. We decided that there are things we need to do to make our lives easier.
You just want to make the best out of everything, no matter what it is. At some point, we all have to face an inevitable. But just that the life you led is the best one you could have done, even if you were sick at the end. I have a lot of inspiration, my grandkids and my husband, but there are sad times. There are really sad times.
My husband tells me to quit crying, and there’s always humor in life. That’s what gets you through — laughing or looking at something that seems silly. I think I’m going to get a cat now. We haven’t had a cat for a while, and I decided I wanted one again.
Stephanie Chuang, founder of The Patient Story, celebrates five years of being cancer-free. She shares a very personal video diary with the top lessons she learned since the Non-Hodgkin lymphoma diagnosis.
Cancer details: Characteristics of both subtypes 1st Symptoms: Lower abdominal pain, blood in stool, loss of appetite Treatment: Chemotherapy (Part A: R-CHOP, HCVAD, Part B: Methotrexate, Rituxan, Cytarabine)
Robyn’s Stage 2E Relapsed Diffuse Large B-Cell Lymphoma Story
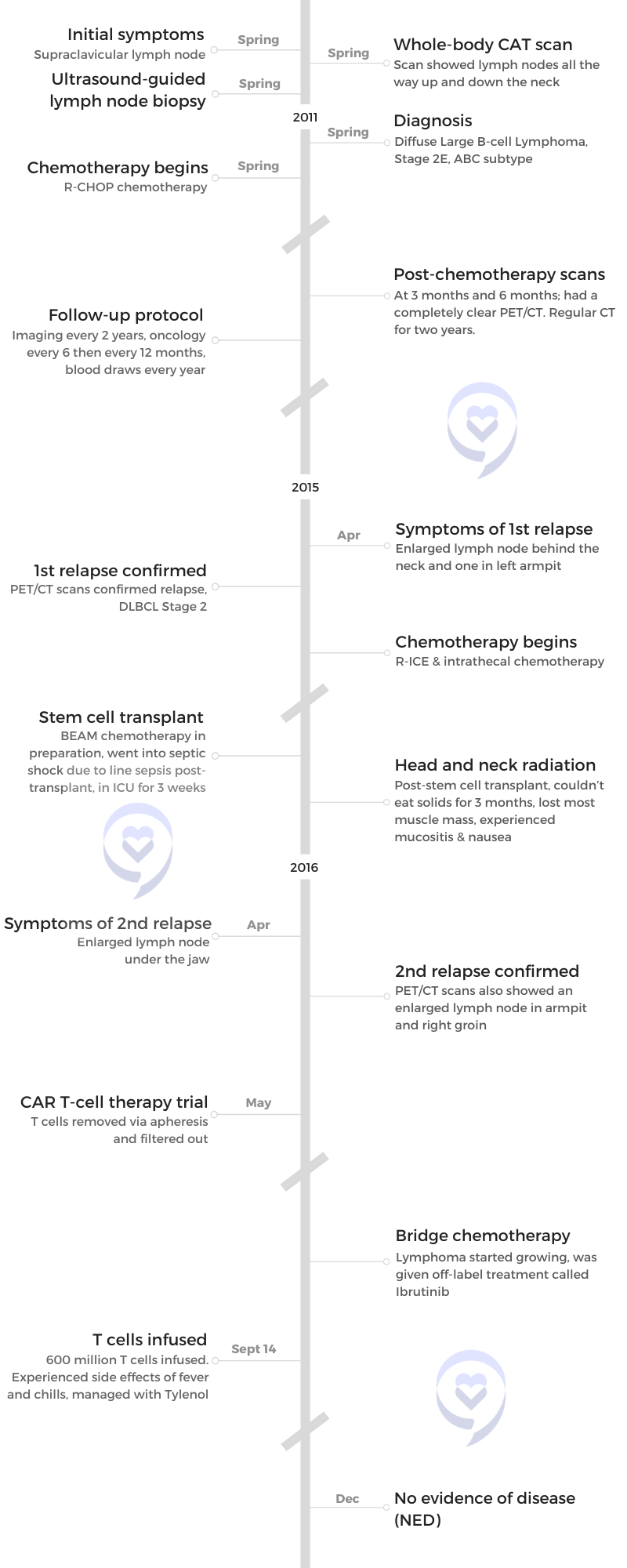
Robyn was diagnosed with Stage 2E Diffuse Large B-Cell Lymphoma, ABC subtype. Four years after going through R-CHOP chemotherapy, she relapsed and went through more chemotherapy, a stem cell transplant, and radiation. She relapsed a second time only 9 months after therapy. This time, she joined a clinical trial for CAR T-cell therapy.
She shares her experience with different treatment modalities and advice on looking for clinical trials.
Name: Robyn S.
Initial Diagnosis:
Diffuse Large B-Cell Lymphoma
Stage 2E, ABC subtype
Initial Symptom: Supraclavicular lymph nodes
Initial Treatment:
R-CHOP chemotherapy
First Relapse:
4 years later
Lymph node at the back of the neck
Treatment:
Chemotherapy: R-ICE, Intrathecal, BEAM
Autologous stem cell transplant
Head and neck radiation
Second Relapse:
9 months after therapy
Treatment:
CAR T-cell therapy trial
Bridge chemotherapy: Ibrutinib
Remission:
Lymph nodes gone within 1 week of getting CAR T-cell therapy
My biggest contribution to medicine is probably not as a physician but as a patient and that’s okay. I’m good with that.
I have been given a second chance at life and it’s an unusual experience for everyone. I cherish it and I enjoy every minute.
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
I’m really nervous I have cancer. Right [on the collar bone], it’s pretty much never benign.
Pre-Diagnosis
Tell us about yourself
Until 2011, I was a very healthy practicing physician with three young kids. I exercised every day, ate right… I probably worked too much. As a mother with three kids, [with] soccer practice and swim lessons, I was probably a little tired but other than that, very, very normal.
Initial symptoms
In the spring of 2011, I was watching TV and I realized that I had a supraclavicular lymph node, which is a lymph node above your collarbone. Given that I’m a physician and a radiologist, [I know] that is always abnormal. It’s usually a sign of some type of cancer — most likely ovarian cancer or lung cancer. That was a really startling realization with no other symptoms — no weight loss, no fevers, no nausea, nothing. Just an enlarged lymph node.
I turned [to] my husband [as] we were watching TV with the kids and said, “I have this supraclavicular lymph node. It’s always abnormal. I’m really nervous I have cancer because it’s always abnormal.” He looks at me [and said], “It’s nothing. You just see too many people with cancer,” because that’s what I do for a living. I do a lot of oncologic imaging, mammography, and PET/CT.
It was one of those situations where I just [turned] my neck and I realized, “Oh my, I have a node.” In the axilla, sometimes the neck, they could be benign. But right [on the collar bone], it’s pretty much never benign.
The next day, I went to work, went to see a friend of mine who is a surgeon, and he’s like, “You have a lymph node so you need whole body CAT scans.”
The minute I looked at [them], I knew I had lymphoma. It was really stunning to actually see your own CAT scan and see that pathology.
Being a physician-patient
It was weird. I’m a radiologist. I read CT scans for a living.
I went to a surgeon who ordered these CAT scans and I had the CAT scans done. He started it from [the collar bone] all the way down to my pelvis because most likely it was an ovarian, stomach or lung cancer. I looked at the images and I didn’t see any cancer there but I saw all these lymph nodes in my neck.
I got back on the scanner and had them scanned a little bit higher up. Sure enough, I had lymph nodes all the way up and down my neck. They weren’t palpable but the minute I looked at [them], I knew I had lymphoma. It was really stunning to actually see your own CAT scan and see that pathology.
I was sitting there healthy. I had no symptoms, no significant family history, nothing. The only thing I had was one palpable lymph node, which was 14 millimeters. It wasn’t that big. It’s just that I do this for a living.
I have probably hundreds of lymph nodes in my neck. There [were] a bunch of lymph nodes behind my nose. I have allergies and at that time, I had some allergy symptoms — probably the symptoms were really from the lymphoma that year — but it was nothing unusual for me.
But to realize that I had cancer then it’s, “Okay, I have cancer. I wonder what kind of lymphoma it is. I hope it’s a Hodgkin’s versus a non-Hodgkin’s because Hodgkin’s has a better response rate.”
I told one of my partners and [literally] the next day, I had a lymph node biopsy performed at work. One of my partners did an ultrasound-guided lymph node biopsy, which I do all the time. Knowing that it’s in the neck, you put a needle and you take some cells out.
I looked at them with a pathologist under the microscope and I asked him if there were Reed-Sternberg cells, which are what you see with Hodgkin’s lymphoma. He said, “No. I just see B cells. I think you have B-cell lymphoma.”
It was tough because this is somebody I work with all day. My partners are doing my biopsy. One of the pathologists is looking at this and says, “You have lymphoma.” Then on Monday, he called me and gave me the subtype.
Because I was diagnosed with something called diffuse large B-cell lymphoma, which is a very aggressive lymphoma, I saw an oncologist that week. I had a port put in and the week after that, I started standard chemotherapy, which is called R-CHOP.
Waiting for more answers
Tom Petty said it the best. The waiting is the hardest part and that’s what I [say] to all patients who are going through this now. You’re sitting there, you’re new at this. I’m a radiologist. I’m not an oncologist. I know a lot but I did not at that point [know] that much about diffuse large B-cell lymphoma.
You’re waiting, your oncologist gives you statistics, and you don’t even hear them and try not to focus on [them]. How do you tell your kids? How do you think chemo is going to go? It’s very daunting, even though I’m in the business, so to speak. The thought of having chemotherapy and having all these procedures done.
One of the chemotherapy agents is called Adriamycin, which is called the Red Devil. Most people have heard about this one and dread that. You wonder, how am I going to do with this? Am I going to be able to function? Am I going to be sick? Of course, you do lose your hair, that was 100% told to me, but it’s scary. Then you’re going to do all these chemos and are they going to work or not? Are you going to survive? You don’t know. You just don’t.
Getting the full diagnosis
With the staging, I had to have all the CAT scans in a PET/CT [and] a bone marrow biopsy, which is unpleasant. I was a stage two, technically stage 2E because I had some lymph nodes behind my nose and something called Waldeyer’s ring — E being extranodal. It makes the diagnosis worse.
Then I had a subtype and that’s sort of controversial. The typing of lymphoma has changed. Back then, I was diagnosed as a germinal cell, but later, I was diagnosed as an ABC subtype. I think it was a mixed subtype. It doesn’t really matter that much. They all suck.
The oncologists do tell you what your percentages are, that’s really part of their job. You need to have some expectations. I’m an optimistic person, so I was, “Okay, fine, I’m healthy. I’m going to do great.”
There are certain types of lymphoma that are worse than others and it’s a process to go through. I remember my oncologist telling me, “If this chemo doesn’t work, we’re going to do something called salvage chemotherapy.” I remember looking at him and saying, “Nope, we’re not going to do salvage. I’m not going to need salvage, not doing it.” He just smiled and shrugged his shoulders, “Well, I just have to tell you that.”
You’re going to do all these chemos and are they going to work or not? Are you going to survive? You don’t know. You just don’t.
That was the hardest part. My husband, I remember talking to him the Monday when the pathology came back. My biopsy was the Friday before Mother’s Day — Mother’s Day traditionally is not a great day for me. I’ve had three Mother’s Days where I was diagnosed with cancer.
On Monday, I got the final results and I remember talking to my husband [while] walking around the neighborhood. We were both just crying. People were looking at us thinking [that] we’re getting a divorce or something. Then to have to tell the kids.
The kids were, at that point, 18, 17, and 13. My youngest child actually has a physical disability. He’s fine but he had just finished a major surgery for leg lengthening. My daughter has anxiety. My middle son is very academic, intense, [and] scientific. When I told all the kids, he was immediately on the computer looking everything up. My daughter was in denial. My son was very upset. It was just hard.
‘Hang in there with me and I think everything’s going to be okay.’
I had two going to college at that point and one was in middle school. They’re older but they’re still babies.
I said, “Mom has a bad diagnosis. I have cancer but that doesn’t mean that it’s going to kill me. I’m going to take therapy, lose my hair, [and] potentially going to be very sick. Just hang in there with me and I think everything’s going to be okay.”
I think for the younger kids, it’s harder with the hair loss in the way your appearance changes and there’s nothing you can do about it. [With] the chemo I had or anybody who has intense chemo, you lose your hair, your eyebrows, and your eyelashes, but the kids were very supportive. I just think they were nervous.
I don’t know if there [are] any good ways to do it. There are some books out there for younger children like mom has cancer or dad has cancer. I think that might be a good way to do it with younger people, but being optimistic is what we did, what we’ve always done.
We did a family vacation. We didn’t let it stop us.
Treatment
Living with cancer
I had six rounds of CHOP. It’s very intense chemo. I would have the chemo on Friday [then] I would go to work on Tuesday in the middle of CHOP.
We actually took a family vacation to Alaska. I booked a vacation. My counts were okay. I talked to my oncologist [and] I found an oncologist in Anchorage that could cover any emergencies. We still took our family vacation. I have pictures of me out there, halibut fishing with my head wrap on, and we still did all this family stuff.
I was careful. Obviously, it’s Alaska. You weren’t around a lot of people so I wasn’t that worried about infection. I was a little tired [so] I would take some naps. We didn’t let it stop us.
Anybody who’s going through therapy, I’m telling you, that was amazing, to have some food, especially for kids.
R-CHOP regimen
Think about chemotherapy now versus when I was in medical school. They actually gave you a lot of antiemetics [or] anti-vomiting medicines ahead of time, which makes you feel weird but it keeps you from throwing up. We had all of that.
They give you either Neulasta or Neupogen shots after chemotherapy that keep your blood counts up so you don’t get as anemic and you hopefully don’t need any blood products. Some people need some transfusions; I didn’t. It’s just a lot of shots.
The infusion itself would take all day. I would have friends come in about every 2 hours in shifts to talk to me.
The other thing that people did is bring food. People brought meals two or three times a week, which was really nice for the family. Anybody who’s going through therapy, I’m telling you, that was amazing, to have some food, especially for kids.
I felt nauseous all the time. I compare it to morning sickness but I never was violently ill. Now, everyone is different. I think I tolerated it pretty well.
The other thing about it is they give you a lot of steroids. A lot of people get all puffy. You gain weight and then you’re nauseous [so] you’re not eating then you lose weight. It’s up, down, up, down. One week, you look puffy and moon face, the next week, you look skinny.
Overall, though, I did well but I had really good physicians. I had friends to help. I didn’t feel great, but I didn’t feel totally awful, so that was a good thing.
I followed everything I was supposed to do.
Side effects from R-CHOP chemotherapy
It always gets worse, mainly because your blood counts keep going lower. You become more and more anemic no matter how many Neupogen or Neulasta shots you get because there’s a cumulative effect on your bone marrow.
I followed all my doctor’s directions. I took certain supplements when they told me to and I followed everything I was supposed to do.
As far as the shots, I think that’s also key for people. I took all the anti-nausea medicines. They would say to stay on a schedule of anti-nausea medicines. I don’t like to take pills [but] I followed everything they said. I think that’s part of the key too.
You also have a more bland diet. They have a nutritionist that meets with you and I think all those things are helpful.
Integrative medicine
My advice to patients is that when you’re at a cancer center and if they have nutritionists or psychotherapy, that’s great. Sometimes centers have things like meditation and massage. There are all these things that cancer centers are doing as part of their integrative treatments and I highly recommend [them]. When I went through R-CHOP 11 years ago, this was pretty new. Now, at least where I work, it’s a standard of care at the center but patients have to take advantage of it.
No one should be embarrassed to ask. I was very happy to see an oncology therapist because to face a life-threatening disease is difficult for most everyone, I would think. It’s a nice service that a lot of these folks offer. I think it’s very important.
Follow-up protocol
The follow-ups were done once you had a clear PET. [For me], it was after three months of therapy and six months of therapy. I had a completely clear PET/CT. After that, they followed me for two years with just regular CT.
I had actually gotten beyond any type of imaging because at two years, they stopped imaging. Theoretically, if you make it to two years [of] complete remission for diffuse large B-cell, there’s a high likelihood you’re cured.
I would actually go see my oncologist first. It was every six months for a while and then it was every year until three and a half years [to] four years. That was the standard follow-up.
[I also had] yearly blood draws. If you go see an internist, a lot of times, they do blood draws. I followed the standard two years of imaging then every six months oncology, every year oncology, and yearly blood draws until I relapsed four years later.
Sure enough, I relapsed.
First relapse
Unfortunately, I relapsed at four years and that was on [a] clinical basis, not based on scans.
Sort of the same thing happened to me. We were in the spring of 2015, April 2015, we were walking around a yard and I realized I had an enlarged lymph node. This one was behind my neck and that’s not a typical area to have inflammation from infection. I didn’t have any cuts or anything. I had no reason to have a prominent lymph node. I went to see my doctor and they ended up doing a CAT scan.
It’s funny how you remember these things exactly. My husband and I were walking around our backyard, looking at the garden. I realized I had a large lymph node again in [the] back of my neck and I wasn’t sick. I immediately thought about lymphoma. Once again, my husband goes, “You’re working too much. You see this all the time. It’s probably nothing.”
I made an appointment to see my oncologist because I felt this node had not been there before. Sure enough, CAT scans, PET scans, I relapsed and this time, it was still stage two. Once again, all the lymph nodes were in my neck and I had one lymph node in my left armpit but it wasn’t big.
I’ll always tell people who have a life-threatening condition, particularly like mine: it is totally reasonable to get more than one opinion.
Getting a second opinion
I actually got several consults from where I live because I live at a major tertiary care center and I called my medical school, which is another tertiary care center. Then I went to MD Anderson for a year. I got three different consults and even a fourth.
A consultant was sent to Nebraska, which is an area of lymphoma. I had been out four years and it was unusual for me to relapse. I wanted to know what else I could have.
At the time, I was just trying to stay alive. I was going to take my best odds. Now, in retrospect, I wish I hadn’t had the radiation, but at the time, I had talked to the specialist. At some point, you actually have to go ahead, have faith, and believe in who you’ve consulted.
I actually had consulted more than one doctor and one thing I’ll always tell people who have a life-threatening condition, particularly like mine: it is totally reasonable to get more than one opinion. That actually helped me because I had several institutions saying the same thing and that I think was helpful. If it’s just one institution, I don’t know if I would have been as comfortable.
Treatment
R-ICE chemotherapy
Back then, I asked about natural killer cells because it had been in the news, but there was nothing available. Everyone convinced me I needed to have a stem cell transplant. I had two rounds of R-ICE, which is much more intensive chemotherapy. It requires you to be in the hospital.
The “I” part of it makes you feel really lousy. During the middle of the night, you have to eat ice cubes to prevent your mouth from getting all ulcerated.
Intrathecal chemotherapy
I actually had to have two rounds of intrathecal chemotherapy, where they do a spinal tap, put chemo into your spinal canal, and have it go up to your brain. Because I’d had the extranodal site initially, they thought I should prevent from getting CNS lymphoma, which was a good recommendation.
Once that was complete, I went into remission.
Side effects of chemotherapy
R-ICE chemotherapy
R-ICE is very difficult chemotherapy for most people. It results in a lot of severe nausea [and] a lot of mouth ulcers. The majority of people end up needing blood transfusions afterward. I did not. I was unusual. You have to take the Neulasta [and] Neupogen shots.
I was also able to work some during that. But I’m really unusual.
When you have pain, you take pain medicine.
Intrathecal chemotherapy
The intrathecal chemo was uncomfortable, but it wasn’t any worse than R-ICE. The thing that was unusual for me was getting the huge catheter that they had to use for the transplant, which is a tri-lumen catheter that goes in your neck. It’s really, really big. I have a bigger scar from that than I do my port scars. I’ve had ports every single time. I’ve had two and then I had this huge catheter.
With this, the only way you could shower is to put plastic all over yourself so you don’t get this catheter wet. It required some medical knowledge or at least to be instructed with directions on how to take care [of] a patient who has these things.
If you have a family member that’s going through this, you’re going to have to have somebody that either has some medical knowledge to start with, is a nurse, or is willing to undergo training and is not squeamish. I can only do so much by myself.
Just like with the R-ICE, because it’s a hospitalized chemo and a lot of people have blood transfusions and they’re very, very sick afterward, they’re [unable] to eat. It’s just very difficult for the caregivers as well as the patients.
Fast forward to the stem cell transplant, most people feel pretty lousy — not initially, but once your white count’s low. In my case, I had a fever and everything. A lot of people have mouth ulcers. They can’t swallow very well. It’s very difficult for the family members to watch that.
The nurses and the staff might give the patient pain meds. I know I had some narcotics when I was in the hospital, so some stuff I don’t remember. I’m glad I had narcotics. I had no problem. When you have pain, you take pain medicine. I don’t remember some of the stuff. I know it was very difficult for my husband and my older son who were there at the hospital. Very traumatic for them.
BEAM chemotherapy
BEAM chemotherapy is just miserable. The worst thing is the Melphalan (the last part of it) causes, quite frankly, really bad diarrhea, like dysentery diarrhea. It’s just the way it is. Everyone survives it. It wasn’t pleasant.
The side effect of Melphalan is tough. A lot of my friends were in the Peace Corps in Africa and they said you haven’t really been to the Peace Corps unless you’ve had diarrhea where you couldn’t make it to the bathroom. I always said I feel like I’m in a Peace Corps. Honorary member.
Managing side effects
When I was there, they have a thing where you would walk the halls. I’m a big exercise proponent and when you walk, it actually helps the stem cells engraft. I really cannot reiterate. I did follow all my directions. The nurses say you need to walk and even if you feel like total garbage, I’d be there with my little IV pole walking around.
Before I had the BEAM, I was even on an exercise bike. But then once you’ve had the BEAM and you’re really, really sick, it’s very hard to do anything.
They actually took my stem cells out, which they do via something called apheresis. They hook you up and they take cells from one arm, filter them through a machine, take them out, and freeze them. Then you get admitted to the hospital for your actual stem cell transplant. They do myeloablation, where they basically blast your bone marrow.
There [are] different ways to do it. I had something called BEAM. You can do it with total bodily radiation. There are some other protocols, but it’s just horrible chemo. It totally obliterates your bone marrow. It leaves you with no white cell count and also a very high risk of infection.
I got an infection so I ended up with septic shock.
At the point, when you have had all your chemo, they give you your stem cells back. It’s really a stem cell rescue and then they wait for your stem cells to engraft in your bone marrow and start making new bone marrow cells, like blood cells and platelets. Until then, they give you transfusions and you hope you don’t get an infection because you don’t have any white cell count.
Going into septic shock
I got an infection so I ended up with septic shock. I was in the intensive care unit and I had a fever [and] septic shock. My blood pressure was zero. I was on something called pressors just to keep my blood pressure up.
I actually still have an aneurysm in my radial artery from having an [arterial] line. There’s nothing you really can do about it. You can just feel it. It’s not that it was done poorly. It just happens.
[Septic shock], it’s pretty common. People get sick. Sometimes they don’t get as sick as I did, but I wasn’t intubated. I had [a] high fever and a positive blood culture. What had happened is the line I had, even though they were using all aseptic techniques, had gotten infected.
They took the [central] line out, gave me all these antibiotics, and I got better pretty quickly. Then my cells engrafted, I started making my own red blood cells [and] my own white blood cells. I got out of the hospital in three weeks, which was pretty quickly. But I was sick. I was really sick.
I don’t remember some of it. My husband and people came to check on me. I was out of it. Evidently, I argued with the ICU doctor about which pressor to use, which I think is pretty funny. I was totally out of it and I’m arguing with the person who’s an expert. I’m a radiologist and I’m telling him which pressor I want. They must have thought I was really obnoxious.
They probably aren’t used to the bone marrow transplant patient arguing about the pressors, which, now I look back, is sort of funny. But the bottom line is they took great care of me and I’m here and I’m alive. Then I went home.
Post-stem cell transplant
You have to be very careful after a bone marrow transplant because even though I had a few white cells, you’re likely to get an infection. You’re not allowed to be around anybody.
The worst was you can’t eat berries — I love berries, like blueberries, strawberries, all that kind of stuff — because of the skins. You couldn’t have anything with skins. You had to be very careful. No salads that weren’t triple washed. All of that for 100 days.
At MD Anderson — even some people from Sloan Kettering because I had relapsed late but had pretty much all been in my neck and even in my nasopharynx — they want to do something called consolidate the bone marrow transplant. Because I was young and healthy, they treated me extremely aggressively. Not everyone would be treated like this, but they wanted to save my life and I agreed.
They said that if I had the head and neck radiation, it would increase my chance of survival up to 5%. My chance of remission after [a] bone marrow transplant was only about 35%. With the head and neck radiation, they said it might increase to 37 or 40. It was our decision to proceed. I followed the recommendation of all of the physicians.
Head and neck radiation is two thumbs down. It’s not fun but you just do what you have to do. I have a lot of friends who’ve had head and neck cancer and they’ve had to experience this.
Most just choose to have something called IMRT, which is a focused radiation therapy, where they actually, in my case, were focusing on where I’d relapsed on the side of my neck and my nasopharynx. They can control the beams to a certain extent, but there is something called scatter radiation. No matter what, even though it’s controlled beams, you’re going to get some scatter and some other side effects.
They make a mold of your head. It looks unbelievable. You lay on the table, they literally screw you down to the table so you won’t move, then they do the radiation. For lymphoma, they usually use a dose of about 30 to 35 gray. Meanwhile, with head and neck cancer, they use double that dose, 70, 75 gray.
I literally survived on smoothies for about four months after [radiation].
Side effects of radiation
Head and neck radiation is very difficult. From my radiation, I was supposed to have very few side effects because it was only over [the neck area]. But unfortunately, I had a lot of side effects.
I had mouth ulcers. I couldn’t swallow solid food for almost five months after having had radiation.
It affected my salivary glands. I just couldn’t swallow. It was very difficult to eat anything.
I literally survived on smoothies for about four months after that and I was supposed to get 36 treatments. I ended up getting 30. They just titrated it down because I had so many symptoms.
The other thing is because of the scatter radiation, it got part of the base of my brain and I developed worse nausea than I’d had through any chemo. Vomited all the time. It was terrible. But again, I did what was recommended. I got the minimum dose for consolidation and I just thought I could take it. I tried to be positive and I made a real effort.
This is the other thing: to eat protein and try to keep my weight up the best I could. To give you an example, I started with a BMI of 22. By the end of radiation, I think I was down to 15, 14, about 103 pounds. That’s really skinny for me.
I think [the intense side effects were] an outlier situation. Medicine is difficult. The people doing my therapy were also my friends and they actually wanted me to get this treatment. I wonder sometimes in the nicest way whether they didn’t tell me about everything or maybe I didn’t hear. I only heard what I wanted to hear, which sometimes happens as a patient. But I know some of the things, especially nausea, was an unusual side effect.
I went back to work three months after my bone marrow transplant, just a week after radiation. I would go [get a smoothie] in the morning. I’d get one of these massive things with protein powder and I would just take it to work.
I don’t think it’s the most healthy thing and there’s going to be someone [going], “Oh, there’s too much sugar.” At this point, I needed calories. I would have some protein, and I could drink that all day long.
Managing the side effects of radiation
I did get an alternative therapy. I had acupuncture. [There have] been some studies [where] if you have acupuncture in your salivary gland, it helps promote the return of your salivary gland function. I think it helped. It didn’t hurt. It was uncomfortable but I was willing to do whatever I could to return to a normal life.
I also kept walking. I wasn’t able to do much physically at first, but I would walk around one block, then I would walk a mile. I’d walk two miles, three miles. I gradually worked up to that to try to maintain my muscle mass and my functionality. It was a determination for sure.
I had relapsed. Lymphoma was back nine months after therapy and I really didn’t have that many choices.
Second relapse
I went on a vacation with my youngest child as he was graduating from high school. While we were on that vacation, I felt another enlarged lymph node. It was actually under [the jaw]. I knew I had relapsed.
I immediately went to my oncologist up at the center where I had the bone marrow transplant. My husband was with me. I had a PET/CT. I stepped off the table, looked at the PET/CT, and knew I’d relapsed. Not only was this hot, [but] I [also] had something in my armpit and now I had something in my right groin, a big lymph node.
I had relapsed. Lymphoma was back nine months after therapy and I really didn’t have that many choices. I would say three times is not a charm for lymphoma.
The interesting thing is my oncologist looked at me and goes, “Hey, you’ll have an allogeneic transplant. You’re Caucasian, it’s not going to be a problem. You’re going to have a match.”
As it turns out, I’m actually multi-ethnic — given my heritage and how you just don’t know by looking at somebody — and, of course, I had no matches. No one [is] even close and I have no siblings.
I didn’t want to have an allogeneic transplant anyway. I had been doing some research online and I initially wanted to have some killer T cells or something instead of stem cell, but there was nothing available.
Differing treatment recommendations
My bone marrow transplant guy wanted me to have a bone marrow transplant and I don’t want to do that. CAR T is so new. This transplant physician, who’s actually very famous, said, “Look, you’re young, you’re healthy, you survived. You’ll do fine.” I said, “This was the worst experience. I don’t know if I’m going to survive. I don’t want to do this again.”
I had another friend who was very experienced say you shouldn’t do this. I have a friend who’s an oncologist, he’s about 15 years younger than I am, [who] said, “Hey, this is pretty good stuff. I think you’ll do well with this.”
Treatment
CAR T-cell therapy trial
Now there was something called CAR T-cell therapy and I had seen that online. I went on www.clinicaltrials.gov and we started researching trials for CAR T. I found one phase, one trial with something called the JULIET trial, phase one, where they had 25 patients and 12 had survived and got into remission. That was probably the best odds that I would ever have. I wouldn’t have [that] kind of odds with an allogeneic transplant.
We started looking for phase two trials for the JULIET trial, but also for the Kite trial, and for Juno. There were two other products and we started searching for those trials.
I had to do all the research myself and this is [what] I want to really stress. I had no advantage here, no connections. All we did was get online. My husband and I went on this clinicaltrials.gov site. We emailed every single center that was doing CAR T. We called them and we started looking. We’re trying to find a space.
I had a little blurb. I put my history in about three paragraphs because I knew I qualified for everything. I had no comorbidities. I just had lymphoma and nothing else wrong with me, so that’s perfect for a clinical trial. They don’t want to have any of the mitigating factors. They want to see just how the trial works, which is what they want for these trials. That’s why people are excluded from trials because they don’t want to muddy up all of the info when you have so many other conditions.
To make a long story short, a space opened up literally. We found out about the space on a Wednesday, I flew to the center — which was actually in Ohio, I live in North Carolina — on Monday. We signed paperwork to agree to do the trial. I was accepted.
Within the next week, I came over and they did something called apheresis where they filtered out my T cells, just like you’d filter out stem cells. They put a catheter in one arm then they put it through this machine. They filter out T cells and return the cells back to your body. Then they sent the T cells out to be modified.
The cool thing about CAR T-cell therapy is it’s your own immune system… This way, you actually modify someone’s own immune system to fight cancer, which is really brilliant.
How CAR T-cell therapy works
CAR T is really amazing. The patient’s T cells are removed from the patient with apheresis. They’re filtered out. Think of these little T cells as little Pac-Man and in these little cells, you take a viral vector — it’s like a deactivated virus — you insert a protein onto the top of that cell. That little Pac-Man binds to whatever that protein is on another cell and gobbles it up or blows it up, whichever way you want to look at it.
When you have lymphoma, the protein is called CD19 but then other lymphomas have a CD30. There are some leukemias and lymphomas that have a CD20 or 22. Now there are trials for solid tumors, like HER2-positive breast cancer. HER2 is a certain protein that these breast cancer cells carry and so they can make a CAR T to fight HER2-positive breast cancer.
The cool thing about CAR T-cell therapy is it’s your own immune system. Right now, our standard chemo treatment for cancer is actually really barbaric. You either poison it, you cut it, or you burn it — that’s the way we treat cancer. This way, you actually modify someone’s own immune system to fight cancer, which is really brilliant.
The T cells can cross the blood-brain barrier. What’s so important is that there are certain tumors that have brain metastases, like lymphoma. A lot of people get lymphoma and it spreads to the brain. This can actually cross that and treat it in the brain. It can treat metastatic breast cancer [in] the brain. They’re using it for all sorts of other things.
Clinical trial paperwork
I did not read every single paper. We went over some of the guidelines. We went over the requirements and this is actually standard for T-cell. I had to be within 30 minutes of the institution. I had to go back for follow-ups. This was a series of things I had to do and I agreed with that.
I knew the results of the phase one clinical trial and this was the phase two trial. The investigator shared phase one. We went over side effects and a lot of that was just one on one.
This investigator, who is a very young investigator, she’s very pro-CAR T. I remember her looking at me and saying, “You are the perfect candidate for this. You’re healthy, your bone marrow is good. You just happen to have lymphoma.”
Costs of joining a clinical trial
Each trial is different. My trial covered the actual drugs and any medical treatment related to my therapy but did not cover the cost to get into the trial, which meant another bone marrow biopsy, some other CT scans, lodging, any kind of lost work, or the caregiver.
My husband, at that point, was not working so he was able to go up with me. We got a VRBO flat and we stayed there. It was very economical that way. People bring that up and some of the trials will pay for that, some of them won’t. Insurance companies will usually pay for lodging for a family member and the patient around a bone marrow transplant, but not for a clinical trial, in my experience.
A lot of this is based on some type of your own financing. With us, we had to finance the car, the VRBO, the caregiver, my food, and then my insurance company covered some of the initial testing, which would have had to be done anyway if I was going to have an allogeneic transplant.
Bridge chemotherapy
The problem was I was in a clinical trial and so there was a delay for those cells. Then my lymphoma started growing. They did something called bridge chemotherapy.
I had an off-label treatment for lymphoma called Ibrutinib, which had shown effectiveness in diffuse large B-cell ABC subtype. Turned out, that worked beautifully. It put me in remission. These are chemo pills you take. It was so much easier than anything I’d done.
Waiting for the T cells
We waited for my cells to be ready. There was a little glitch because I made too many cells. The FDA didn’t like that I had too many cells, so they wouldn’t filter them off. I had to get FDA-approved just to have my own cells back. I had my cells out in May and then I was scheduled to have them infused in September of 2016.
Cytokine release syndrome
Once these T cells are altered, they’re cultured in the lab, and then they’re infused in the patient. The T cells go around, bind to the tumor, and blow all these little tumor balls up but that actually can cause a response by your immune system called cytokine release syndrome.
It’s similar to some of the people’s reactions to COVID. We’ve actually seen people with COVID pneumonia that get these horrible infiltrates in their lungs. It’s more of a reaction to the virus and the cytokine reaction as opposed to the infection. It’s very similar. They were trying some of the same treatments for COVID that they use in cytokine release syndrome for CAR T.
With CAR T cytokine release syndrome, some people get it, some people don’t. [For] most people, it’s very mild and transitory. It’s not permanent. It just is an immediate reaction and then it goes away.
My T cells were infused in September of 2016. The infusion lasted 10 minutes. I had 600 million cells in this big bag. Everyone clapped when they were infused and then they waited. What’s going to happen?
Within 24 hours, I started getting a fever. I was told if I was going to [have a] fever [to] go back to the hospital. It got up to over 104 [degrees]. I had low blood pressure, shaking chills, [and] felt terrible for three days.
Because it was a trial, they didn’t give me anything for it. I only got Tylenol. They give you things for this now that I didn’t get, but it went away.
I would have six months to live, without therapy. Here I am, almost six years out. It’s amazing.
Remission
By the time I was discharged from the hospital, my lymph nodes had gone. They’d melted like ice cubes. They were completely gone. I was in remission — clinically, not with a PET scan — within one week of getting CAR T. Just amazing.
I felt fine. I was just tired [and] a little nauseous. The fatigue was there but nothing like [a] bone marrow transplant. It was nothing. I’m enjoying the gym two weeks into it. It was great. I went back to work four weeks after CAR T-cell therapy. I only went part-time at first and then I gradually went up to full-time.
Here I am, almost six years out. It’s amazing.
I would have six months to live. Without therapy, on average, you have six months to live. Now, if I’d taken some steroids or had an allogeneic, I might have had another chance to live. But the problem with [the] allogeneic transplant, again, I had no match, which means I’m not going to do well. Now some people do okay, but without a match, people don’t do as well.
When you get to the point where you’re getting CAR T, you don’t really have a whole lot of other choices.
Post-CAR T-cell therapy
When you compare it to how sick I was after [the] stem cell transplant, I just couldn’t eat for so long. I felt terrible. I felt fine after CAR T.
One thing after CAR T is I’m immunodeficient because the T cells destroy all my B cells — the cancer B cells and my normal B cells.
I’ve had to be very careful about infections like MRSA or CRE. All of these antibiotic-resistant organisms are the ones I stay away from. I had to change my practice because I was doing a lot of hospital care. Now I’m all doing outpatient just to be careful.
CAR T works in lymphoma about 40% of the time but not 100% of the time. They’re working on improving it. [For] those people who fail CAR T, a lot of them would go on to an allogeneic transplant. Hopefully, not me now.
I have been given a second chance at life and it’s an unusual experience for everyone. I cherish it and I enjoy every minute. I’m very, very grateful for medical research and all the doctors, caregivers, my friends, and everyone who’s really helped us along with this. It’s just really special.
It’s interesting because CAR T’s a new therapy. Everyone’s very nervous about cytokine release syndrome [and] all these side effects, but they don’t really think about the side effects [of a] stem cell transplant, which are much worse.
Stem cell transplant, [an] allogeneic transplant, has a 10 to 20% mortality rate just from having the transplant. CAR T almost has a 0% mortality rate. A lot of people can get neurotoxicity with this where you’re confused for days. [The] majority of people get totally better. I really don’t know of any other ones that haven’t gotten better.
When you get to the point where you’re getting CAR T, you don’t really have a whole lot of other choices. Right now, CAR T is being used as a second-line therapy ahead of stem cell transplant, which I think is awesome. Some people are very nervous about that but they need to really research what the stem cell transplant side effects are as well as CAR T because it’s a new treatment. Everyone gets very nervous about that. I get it.
Words of advice
Looking for clinical trials
I still think the [ClinicalTrials.gov] website is pretty straightforward because you put your diagnosis in and you just have to look at trial after trial.
Right now, they have CAR T-cell trials for solid tumors, for immunologic deficiencies, and some of those organizations have their own nurse navigators or people who can help with advice. I just think you have to be your own advocate and start calling everywhere.
Bone marrow registry
Everyone should get on the bone marrow registry, that’s my big plug because there [are] a lot of us out there that are multiethnic, so we need a lot of people on the registry. I just didn’t really have a chance.
Any time you have a life-threatening situation, whether it’s cancer or any other disease, you need to use any ancillary help you can. I’m a big believer in integrative medicine as well as standard Western medicine.
[With] integrative medicine, there’s a role for psychotherapy. It’s really important [for] anybody who’s gone through a life-threatening event. People in the military who’ve almost died, a lot of them get PTSD. I think all cancer patients get a form of PTSD. It’s important for a lot of patients to talk to therapists. I’m all for that. I certainly did that after my bone marrow transplant. It was very traumatic for a while, but luckily, it was helpful.
I also recommend talking to nutritionists. I’m against any type of major extreme diet. They’re not necessarily helpful for you. It’s amazing when you talk to nutritionists [about] how you can improve the way you feel.
I’m also a big believer in exercise. A lot of that you can do on your own. Just walking and being outside is really important and it’s amazing what the health benefits of that are. I think it’s really true. Eat right and exercise. There is a lot of role for that. It’s simple but true.
Role as a physician-patient
My biggest contribution to medicine is probably not as a physician but as a patient and that’s okay. I’m good with that.
I’m so happy to be able to help others. This is what I’ve done my whole life. I wanted to become a doctor since I was five. I’ve spent my life as a physician trying to help patients and here I am able to help them in a different kind of way. I think it’s been a lot more impactful and it’s going to affect the way that cancer is treated from now on.
This is the future. The immunotherapies are the future of cancer therapy and, as it turns out, even some therapies for autoimmune diseases. It’s a whole new world out there and I’m very optimistic.
Before I had cancer, I was pretty empathetic. Now, I am even more empathetic. My practice right now does involve a lot of [mammographies] where I see patients every day. I diagnose breast cancer every day. I see patients who’ve had breast cancer.
I see patients who are in the middle of chemotherapy and I can really chat with them. In some cases, I give them advice about going to tertiary care centers [or] integrative cancer therapy centers. They may not have heard of that. They may have just been moved here. I’m always happy to offer that because it is a service the hospital offers.
I also just hold their hand and talk to them about losing their hair, having it grow back in, how weird that is, and can joke about some things. It’s nice. We have a special bond, some of the cancer patients and myself. I think it’s great for them and it certainly helps me. It’s a win-win situation.
Stephanie Chuang, founder of The Patient Story, celebrates five years of being cancer-free. She shares a very personal video diary with the top lessons she learned since the Non-Hodgkin lymphoma diagnosis.
Cancer details: Characteristics of both subtypes 1st Symptoms: Lower abdominal pain, blood in stool, loss of appetite Treatment: Chemotherapy (Part A: R-CHOP, HCVAD, Part B: Methotrexate, Rituxan, Cytarabine)
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
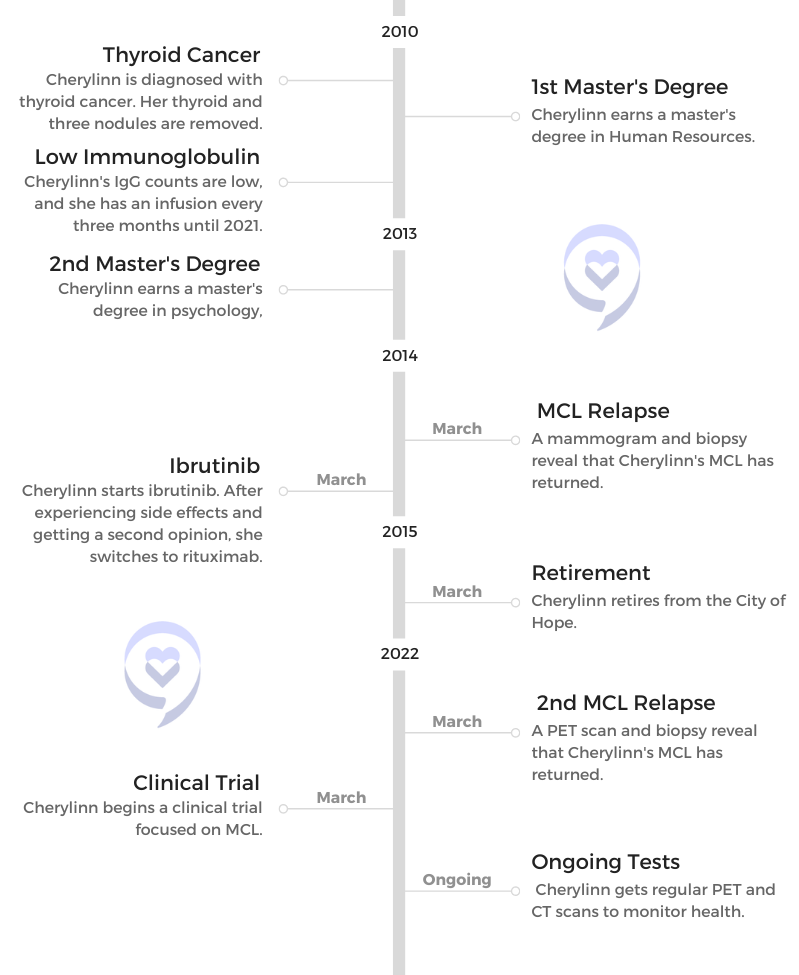
1st Symptoms and MCL Diagnosis
Introduction
Tell me about yourself
I’m retired from City of Hope. Now I’m just at home. I have a Great Dane who’s my partner, and she and I do a lot of things. We go walking and try to get healthy, and I love to read. I used to have a lot of books, and then I found that I had tons of Rubbermaid containers with books. I got into the Kindle, and so now I have hundreds of books in my Kindle, but that’s what I like to enjoy.
There are some mountains in Los Angeles, where I live. It’s nice sometimes to sit on the deck when it’s really nice and just have my Kindle or maybe a glass of wine, some music and just enjoy reading.
I volunteer for the Leukemia & Lymphoma Society (LLS), and I enjoy doing that. I talk to people who call in that are newly diagnosed with cancer and just give them some insight. My philosophy is that if I can make one person not fear cancer as a death sentence — that it’s something that you can get past — then I’ve done my job. I try to help people to withstand cancer. I tell them all the educational and financial programs. There’s a lot to LLS, and that’s why I’ve been volunteering with them since 2007.
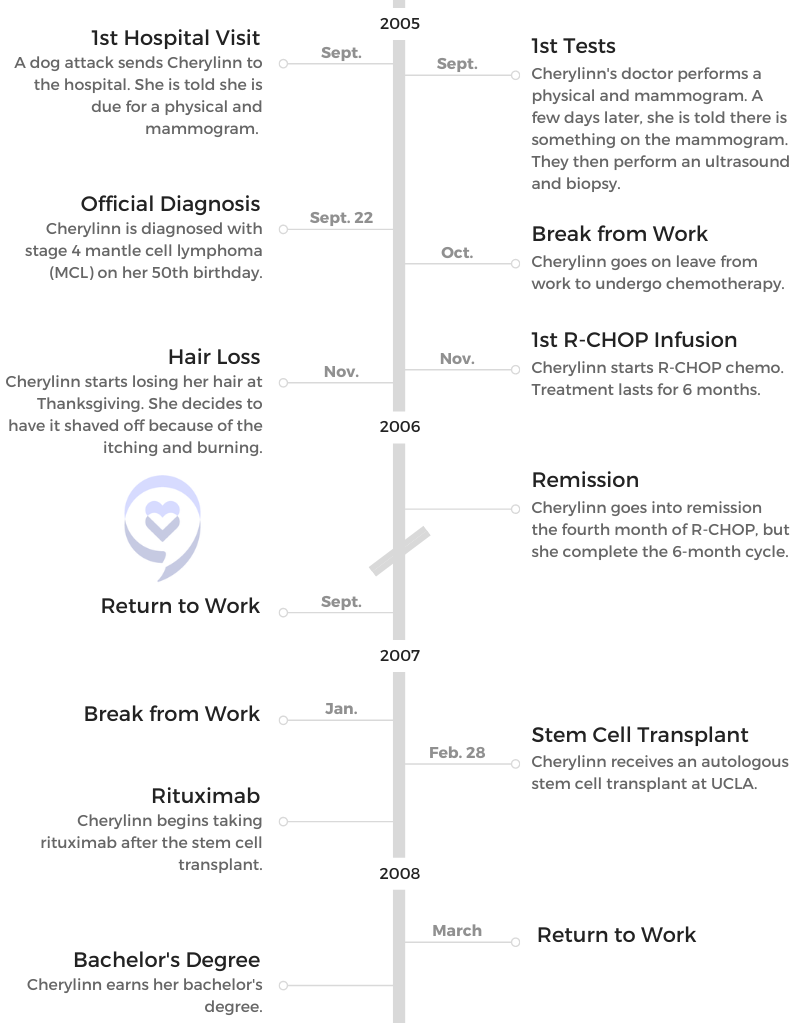
After a freak accident sent you to the hospital, what happened and what tests were run?
The paramedics and the hospital said, “Go see your primary doctor afterward.” It was when I saw my primary doctor that she said, “You haven’t had a physical or a mammogram.” I had a sister who had passed away from breast cancer, so she said, “You are due for a mammogram.”
Now that I’ve gone through this, what am I going to do to cure it?
“Okay, fine,” I thought. I didn’t think anything of it. I felt healthy. I’m overweight, but that’s pretty much the only symptom that I had. They did the physical when they did the mammogram. A couple of days later, she said there was something on the mammogram.
They did an ultrasound. I assumed it was breast cancer. They were doing the ultrasound but under my armpit. I was kind of worried about that. Then within that same week, they said, “No, we’re going to do a biopsy.” It was during that biopsy that they discovered that it was mantle cell lymphoma.
At what point did you realize something serious was happening?
It was so fast. One day I’m having the ultrasound. Two days later I’m having a biopsy. Then all of a sudden, it’s like, “By the way, you have cancer.” But again, I was assuming that I had breast cancer, and my sister was such a strong person that she always made me feel like you can get through this. That’s why she was my role model.
I was like, “Okay, I have cancer. I will see the doctor, and I’ll deal with it. I’ll do whatever I need to do and then go from there.” I had the “Why me?” and the crying and the anger, but it was more of, “Okay, now that I’ve gone through this, what am I going to do to cure it?”
MCL Diagnosis
Testing and waiting for results
They put me under because they did the biopsy on both sides and took out lymph nodes. They just said it was a biopsy. That’s why all along I thought it was breast cancer.
Cherylinn’s sister, Pat.
I received the results probably within a week. I was close to my 50th birthday. Ironically, the day that they did the biopsy, my kids were giving me a surprise birthday party with family and friends. I’m the kind of person that when I have to go to chemo and stuff, I just go by myself. I don’t bother anybody.
I thought the biopsy was just go in, get the biopsy and go home, and so my kids had planned that party for that night. I was in the hospital, and they were like, “You can’t have this.”
I was like, “Well, it’s okay. I’ll be fine.” It worked out okay. Then the following week is when they actually told me that it was cancer. When I saw the oncologist, that’s when he told me that it was mantle cell.
Then he said it was stage 4 and I was terminal. For me, terminal was my sister, who was maybe 80 pounds. You look like a living skeleton. That was terminal. I was looking at myself and saying, “How could I be terminal?”
He just said, “You’re terminal. We’re just going to make you comfortable.” I had been newly divorced after 26 years of marriage, and I had 2 children at home. My daughter was 14, and my son was 17.
How did you break the news to your children?
I made dinner. I have 3 children, 2 boys and a girl. My eldest son was married. He’s actually a paramedic. I had them all come to the house, and I just told them. I said they found cancer and that I’m going to try to go through treatment.
My daughter was 9 years old when my sister died, and she and I were very, very close. I didn’t realize that she had a memory of seeing my sister like that. When I said it was cancer, the first thing my daughter asked was if I going to look like my sister, like Auntie Pat. Like I said, my sister and I had talked a lot. I decided I was going to be very truthful, and I just said I didn’t know but that we would get through it.
There was an incident where the paramedics took my uncle to the hospital. My daughter had asked a paramedic, “Are you going to bring him back?” The paramedic said, “He’ll come back.” He died in the hospital.
When the paramedics came for my aunt, it turned out it was the same paramedic, and it was like 2 years later. My daughter said, “Are you going to make her come back?” He said, “Oh, yeah, she’ll come back.” S he told him, “You’re a liar because you took my uncle, and he didn’t come back.”
I told him, and then he realized it was the same house. I said, “You have to be very careful what you tell children, because they remember.” I didn’t want to tell my daughter, “Yes, I’m going to be fine,” and then what if I passed away?
When did you find out it was mantle cell lymphoma?
He was an older doctor. When I went back in after they had done all the PET scans, the bone marrow and all the tests, they told me that he had left. He had to leave on emergency medical leave.
He said, ‘Do you want to fight?’ I said, ‘Yes, I’m going to fight.’
They had this young doctor from UCLA who was going to see me. I saw him, and I asked him, “How long do I have? 3 months? 6 months? What do I have?”
He looked at me and said, “Lift up your left leg.”
“What?”
“Lift up your left leg.” So I lifted my leg. Of course, if your doctor tells you to do something, you do it. He said, “I don’t see an expiration date.”
“What?”
He said, “I don’t see an expiration.”
I said, “Really, doc?”
He said, “I don’t believe in it. When it’s your time, it’s your time.”
Then the doctor said, “Now, I will tell you, the person in this chart is as bad as it gets. You’re stage 4. It’s in your entire body, and it’s also in your bones. But I’m looking at you, and I can’t see it.” With that, he said, “Do you want to fight?”
I said, “Yes, I’m going to fight.”
He said, “I want to treat both cancers at the same time. Normally we would take care of the mantle cell first and then the bone cancer, but if the bone cancer goes to your brain, all bets are off.”
Like I said, I had no symptoms. The only symptom I had is I was always tired. I decided that I wanted to fight. When I started the aggressive chemo, the second day, they would go to radiology.
They would take the spinal fluid out of my spine and then inject the chemo directly into my spine. I did both chemos at the same time. It was really painful because I had to stand up and hold on while they drew the fluid and then put the chemo in.
What were the side effects from R-CHOP?
It was the typical side effects: you lose your hair, you can’t eat, you throw up. I had some butterscotch hard candy. For some reason, my body accepted the butterscotch candies. My son was at the market, and he found some butterscotch pudding.
He bought it just to see, and it turned out that my body could accept it and wouldn’t throw it back up. When I was in the hospital, I would always have my butterscotch pudding. If you can find that one thing that your body can tolerate, maybe that’s just what you need to help you.
At Thanksgiving, I was cooking, and all of a sudden a whole chunk of my hair came out. It was like my realization. My head used to itch a lot and burn. When that happened, I actually put a shower cap on because I didn’t want it to go in the food. Then I went to a barber.
It was kind of strange because this was 2005. Women being bald was not usual. I said, “I need you to shave me.”
He said, “Oh, you want your hair really short?”
“No, I need you to shave it,” I said. He questioned it, and then I just pulled my hair. Then he saw, so he shaved my head. It itched really bad, so it was easier just to shave my head at that point.
I was okay with being bald. My daughter was going into high school. I had a wig, but I would only wear it in front of people or her friends and stuff like that when I had to go out. Most of the time, I would just stay bald.
I’ve been bald 3 times. This last time that I got the cancer, I asked the doctor about the chemo. I asked her, “Will I be bald again?”
She said, “Cherylinn, it’s just hair.”
What you don’t understand is for a woman, hair is important. For me, even though I’m okay with being bald, being part of a woman is having hair. She said she didn’t know, and luckily I didn’t lose my hair.
If there’s dishes in the sink, just let there be dishes in the sink. As women, we want to just do supermom things. When you’re going through treatment, you can’t.
I’ve been bald 3 times, so I understand. That’s why sometimes when I see ladies that are bald, I wonder if they are going through treatment or if it is now because women are bald. You see it all the time, so it’s not that big of a thing.
Sometimes when you know somebody is going through treatment, it’s like a sisterhood. Sometimes I wish I could just put my arm around them and say, “I understand.” I don’t want to go into their space, but I understand what they’re going through.
I went into remission about the fourth month of R-CHOP. It was like, “Okay, good, we can stop this.”
My doctor said, “No, you have to do the whole 6 months.” So I did, and I was okay. It was just standard. I was sick.
Being a single parent, when I would come home from the hospital, I’d see dishes and laundry. The first 1 or 2 times, I started going back to mom mode where I was cleaning the kitchen, wanting to go to the market, do washing and all that.
I ended up in the hospital because my counts went really low. I had to learn that I have to accept that I can’t be supermom. If there’s dishes in the sink, just let there be dishes in the sink. As women, we want to just do supermom things. When you’re going through treatment, you can’t.
I had an endocrinologist as well because I had Hashimoto. When they did the CT scan, they found that I had thyroid cancer. That was in 2010. They just took out my thyroid and 3 of my nodules, and that was it.
Relapse in 2014
An MRI scan showed that I had nerve damage on my right arm. It turned out my neck was degenerating, and I wondered if it was related to the bone cancer. The doctor said he didn’t know. He didn’t think it was. It was just my neck degenerating.
They ended up putting a titanium rod in my neck. Unfortunately, there were some complications during the surgery because it was a 2-part surgery, and they weren’t able to do the second part. I just had the titanium rods put in my neck, and that helped.
I was able to get all the feeling back in my right hand, with the exception of my thumb. My thumb still feels like it’s numb, like it’s asleep, but it’s there.
They did a mammogram. At first, when the radiologist had said there was a spot on my right breast, she didn’t want them to do a biopsy because she said, “Mantle cell doesn’t go in the breast.” But he was really adamant about wanting to do the biopsy.
We did the biopsy, and then it turned out to be the mantle cell. It was a surprise for me. I’ve been told that it was an aggressive cancer. I always knew in the back of my mind that it was going to come back sometime.
Of course, I went to see what my options were. At that time is when she told me that FDA approved a pill chemo, which was the ibrutinib. She wanted to put me on that, and so I did that.
Choosing a treatment option you can still work while taking
We were looking at all the different options. Rituxan had always had a really positive effect on me in regards to my treatment. She recommended this new drug that was available.
With my history, she was confident that would be the route to go, and it would also allow me to continue to work. That was one of the things, too. I wanted something that I might be able to still work on. She said that was a good one and that I would be able to. It was a pill. I could take it in the morning, and then I would be able to go to work.
Because I’m a single parent, it’s very important for me to continue to work to provide for my children. My daughter was still going to private school, and my son was still living at home because he was helping to take care of me. He was going to junior college, and I wanted him to be able to go to college. Being able to provide and work was very important for me.
I knew with the Rituxan, I would be able to maybe continue working, but it would mean that 1 day a week I would have to go get treatment. Normally, the next day you’re usually tired, so it’d be like 2 days a week I would be out. When she said that ibrutinib was an option where I could take pills and that I would be able to continue to work, that was a factor.
I worked for City of Hope, and I’m a patient with City of Hope. Because I worked for chairmen, I knew a lot of the doctors. One of the doctors, the provost, is Dr. Rosen. He’s also on the board of directors for the Leukemia & Lymphoma Society.
One of the things is making sure that if people don’t feel comfortable, get a second opinion and don’t feel bad getting a second opinion.
I asked the secretary if I could talk to him as a second opinion. I went to go talk to him, and I explained to him about my side effects. I was concerned about working and having the side effects, and he was the one that recommended maybe I should change drugs. He’s the one that said he would talk to my oncologist. He asked me what I had taken before, and I told him that Rituxan had worked.
Getting a second opinion
When he went to talk to my oncologist, that scared me, too. One of the things is making sure that if people don’t feel comfortable, get a second opinion and don’t feel bad getting a second opinion. When I asked him and he went to go talk to my oncologist, I felt like she was going to be really offended that I got a second opinion.
She told me something that was very interesting. She said, “If they’re a good doctor, if they’re conscious of their patient, they shouldn’t be offended that you want a second opinion.”
I said, “I’m so sorry. I didn’t mean to go over.”
She said, “No, no, no, it’s okay, Cherylinn, because if you’re not doing well and this works, let’s go ahead and put you back on it.”
That’s one of the things that I liked about City of Hope and my doctors. We talked. They listened to you. We ended up changing treatment, taking me off that and putting me back on Rituxan. By the third treatment, I was back on Rituxan.
Discussing potential side effects of ibrutinib
I don’t remember too much. I know we discussed potential side effects, but I think at the time, it was more of, “Let’s just give it a month or 2 and see if it’s maybe just initially in your body, and that’s why your body is reacting to it.” By the second month, I was having the same symptoms, and that’s when I was concerned.
Low immunoglobulin (IgG) counts
I always call Rituxan my go-to chemo medicine, because for some reason I was able to tolerate it, and it seemed to work for me. I just have a low IgG.
It seemed like every 3 months, I would know my counts. I knew my counts were low when I would get a cold sore either on my top lip or inside my mouth, or I’d find bruising where I knew I hadn’t hit myself. I would know my counts were low, and I would just call my doctor and say, “Hey, I think my counts are low. I need to have a blood test.” Sure enough, they were low, and then she would schedule me.
My counts were low every 3 months, it seemed. It got to be where we just knew to set me up for an infusion. It just seemed like for as long as I can remember, like maybe 2010, every 3 months I would have to go to get the immune globulin intravenous (IGIV).
I called it my tune-up. It’s just like your car. You have to go in and have your tune-up. You make the car run well. It’s like I go in, and they plug me in.
Like I said, I was lucky enough that I worked for City of Hope. I would work in the morning, and then I’d go that afternoon to have the treatment, and then I’d be back to work the next day. I was fortunate enough that I worked for City of Hope, so I was able to do that.
Remaining Positive Through Relapse
The importance of positive thinking
Honestly, from the get go, I always thought it’s your attitude. I’ve read that with cancer or any illness, you accept it. Your attitude toward it is, “Okay, I have this, I’m going to fight it,” or “I’m going to deal with it or my treatment.”
Sometimes I think maybe it was like a guardian angel.
I think when you talk to people that are diabetics, it becomes part of their lives. Then it’s just your attitude. If you think, “Oh my God, I have to do this again,” then you’ve already put yourself in that position where you’re dreading it.
I don’t. It’s like, “Okay, I got to do this.” It’s like getting up to go to work every day. I got to get up. Okay, 3 hours I’m going to have to be plugged into this machine. I can look at the TV. I can read my Kindle. There are options. I can relax.
Relapse in 2022
It was in my right leg and my left groin. That was ironic because when they did the PET scan, that was only supposed to be from my neck to my torso. For some reason, it went past into my legs. Sometimes I think maybe it was like a guardian angel where they were like, “Let’s just go a little bit further,” and they found it.
At the time, she was like, “I’ve never really seen it there.” The doctor was like, “We don’t know if it’s mantle or not.” I just had to assume that I had something in my body that shouldn’t be there, and we were going to have to deal with it.
They did a biopsy in the right, but they had found that there was a spot on the left. Because originally I had it in my right breast, they concentrated on that. They also did a biopsy on the lymph nodes as well. It was in the lymph nodes.
Then I had a different oncologist because it turned out my original oncologist wasn’t a specialist in mantle cell. She was a myeloma doctor, so she had referred me to a mantle cell or non-Hodgkin’s specialist.
Meeting with the oncologist
When I saw her, we luckily Zoomed, because my son, the paramedic, lives in Lancaster. His fiancée is also a nurse, and she’s actually an oncologist nurse. They were on the phone with me and the doctor. I wanted them there because I figured if there’s any questions that I might not think of, they would know. Of course, my future daughter-in-law was able to ask questions about my options, which was really good.
What I liked is that my oncologist was very open and took the time to talk to the 3 of us and answer questions. I’m a layman. Even though I worked for City of Hope, I was a secretary. Then she wrote on a piece of paper and was able to show them because they could relate, and they knew more of the medical terms. I was just thinking chemo, and she was talking about immunotherapies and CAR T-cells and all this stuff. That’s why she gave me options.
When my oncologist was explaining, she said that there was the standard Rituxan. She said that those drugs had advanced so much since the time before. There are so many different improvements. Rituxan has improved a lot, and even the ibrutinib had improved.
I was leery about that one because of the side effects, but she said they had worked out some of those side effects. The chemo brain was one of those that was like one in 1,000, and of course I happen to be one of those in the 1,000 that had that one. I had it really bad.
Chemo brain
Chemo brain is something for some reason some cancer patients have, and I unfortunately was one of those that had it. I’m talking to you, and then it feels like somebody just put up like a black sheet of paper in front of me, and I have no memory.
You can say, “Cherylinn, we were talking about X, Y and Z,” and I won’t remember. I won’t remember at all, and you’ll have to just talk. Sometimes it can be really scary. Working, especially working for a chairman, that was not a function that I could do. I couldn’t be talking to a patient or somebody on the phone and then all of a sudden be clueless. That was one of my concerns now.
Clinical Trial and Stem Cell Transplant
Clinical Trial Options and Requirements
Treatment options
She mentioned the Rituxan, and then she also mentioned CAR T-cell. I knew a little bit about it. The CAR T-cell, even though it’s a really good therapy, is kind of like the one that you use as your last resort because it’s so potent. You want to really keep that until when you’ve exhausted everything else.
CAR T-cell therapy
My son or future daughter-in-law had asked, “What about the CAR T-cell?”
“That one is a good one,” she said, but she wanted to try other options first and save that one. Like I said, mantle cell is a cancer that’s going to come back. That’s reality. I’d rather keep that one in the back burner. At that point, when the Rituxan doesn’t work anymore or this doesn’t work anymore or there’s nothing out there, then we have that as an option.
There were 2 clinical trials that she had talked about. She said there was one clinical trial where it was an immunotherapy plus a chemo drug combination. Then there was another clinical trial that was just an immunotherapy that was specifically made for mantle cell. When my son and Melissa and I were talking about it, I seemed to gear toward trying the clinical trial.
With anything, we have a chemo drug like Rituxan. It kills everything. It kills the good cells and the bad cells. I’m older, so I want to make sure that if I have good cells, I want to keep those good cells. The clinical trial was made specifically for mantle cell. For me, it seemed like a logical choice to try the clinical trial.
With clinical trials, a lot of people think that some people get placebos and some people get the drug. No. What people have to understand with clinical trials is that everybody is going to get the drug.
It’s just to see how well it works and how it affects people. That’s why it’s always good for people to understand that clinical trials are not where some people get placebos. Everybody gets the drug to see how it’s going to affect you.
She was really good at explaining the clinical trial, the one that had the drug and the chemo. If I had done the Rituxan, it was going to be the same thing. It was just a general non-Hodgkin’s chemo. It was the immunotherapy plus the chemo.
I have a daughter, and I have a granddaughter. Will this affect them down the road?
It had really good results, but then when she said they had the clinical trial that was specifically made for mantle cell, it just seemed like a no-brainer that I would want something that was specifically for MCL. I asked, “Okay, if you had to choose between the 2?”
She mentioned the one that was specifically for mantle cell. She said, “That one is more toward just for your type of cancer, but they all work. Any one that you want will work, but if you want the one that’s going to be specifically for the mantle cell, this is the clinical trial. That would be the best bet if you’re going that route.”
Requirements to get into the clinical trial
They did a barrage of tests. The EKG, the stress test, tons of blood work, tons of paperwork. Be prepared that you’re going to do a lot of paperwork. What’s good is that wherever you go, if you’re in a clinical trial, you have a clinical trial staff specifically outside of your oncologist who will walk you through it. They will literally sit there and walk you through all the paperwork.
One of the things that they had mentioned to me when I was sitting with them was genetic testing. I thought, “Well, wait a second. At my age, what good is genetic testing going to do?” They explained to me genetic testing would help future generations, especially within my family. I have a daughter, and I have a granddaughter. Will this affect them down the road?
With breast cancer, my sister had told me it may not affect her children — she had 2 daughters — but it might affect her grandchildren. I thought, “You know what? Yeah, maybe a genetic test, which I am going to have done, might help.”
Then you do the clinical trial. For that, your first round of chemo or the drug, you’re in the hospital environment. Like anything, the first time you take it, your body reacts.
That’s reality. I did have a reaction, but they were aware of it. They were able to help me. You had the typical throwing up and the fatigue. In my case, my liver enlarged, but they knew. That’s one of the reasons why you’re in the hospital. They’re aware of these, but it’s good for them in the clinical trial to note those things. The next phase they go into, they’ll know this might be something that happens. They may be aware of it all the time.
Reading through the informed consent document
They did sit with me and go through the pages, but it was like scanning. It’s like anything where you just scan it. They show you the important parts of the paperwork. I actually did sit and read, and there were a couple of places I highlighted. Luckily, I was through the portal of City of Hope. I emailed my doctor and said, “I saw this and this and this. Should I be concerned about this?” Then she responded to me with an answer that made me feel better. I thought it was good.
Financial obligations
Because it’s a clinical trial, I haven’t had any costs for myself. It might also be the type of insurance. Because of my age, I’m on Medicare. Also, because I want to continue to go to the City of Hope, I have a Blue Cross supplement. I haven’t had to pay for anything, but I think it’s part of the clinical trial that the lab work and everything is covered.
Reporting symptoms
For any symptoms that you have, anything that is out of the norm, they ask you to call them and let them know. This way they can say, “Okay, yeah, maybe this might be related,” or “No.”
For some reason, I had really bad headaches. I could take Tylenol, so once I took the Tylenol, the headache went away. I made sure that they knew that I was having headaches.
For some reason, I was always hungry. I was on a weight management program. I had lost 40 pounds, and I was so excited about losing the 40 pounds. I’m on this chemo, and I’m thinking, “I’m not going to be eating.” Then all of a sudden I’m eating, and I’m hungry. I put on like 6 pounds.
They told me to be concerned about my weight, but not to dwell on the fact that I was gaining weight with it. That was one of my side effects, so I don’t know if being hungry is a positive or a negative thing.
Reporting and treating side effects
I would journal my symptoms, and I would email my oncologist. I would say, “This is what’s going on.” I woke up one day, and I couldn’t stand on my left leg. It wasn’t related. I have neuropathy. It was one of those things where I talked to her about it, and then I talked to my pain management doctor. We were able to get me a medication that relaxed the muscle.
I had the chills and the high fevers the day after treatment, and I ended up in the the triage and emergency.
I sat at home thinking, “Is this related to the chemo, or is this just my body?” I let them know that that was what was happening, that I was having pain in my left leg. It was resolved within a few days by just taking medication.
That’s one of the things with the clinical trials. You have to let them know, because what if it was a symptom, and you didn’t tell them? Don’t feel like you’re bugging them. If you say, “Hey, you know what, I have tingling in my right arm,” let them know it because then they can note it.
Then they can work with you to find out what the tingling is. Is it related to your treatment, or is it just something happens to people, especially when you’re older?
Cytokine release syndrome (CRS)
I had the chills and the high fevers the day after treatment, and I ended up in the the triage and emergency. I ended up in the emergency room, but it turned out that my PICC line was infected. They had to take that out, but I think it was a combination of both.
Then again, I had the chills. I thought, “Oh, I could just deal with it at home,” but then I called. I live alone, so I had to call my son, and he lives like 10 minutes away. He took me in because I was running a fever, like 101, and I had the chills really bad. They just kept me, they hydrated me, and then I was able to go home later on that day with antibiotics.
That’s the whole point of a clinical trial. If I call them and I’m telling them all these different symptoms, it might help the next phase and the next group of people, and they might be able to find out what is causing the chills and what’s causing the headaches. That’s what they do. They tweak it so that they know that for the next phase. They already are aware that these people have had those symptoms.
No question is a stupid question.
Usually within a day or 2, I’m back to normal. I walk my dog. I live in the mountains. I’m back to walking her again. Now I’m on the next phase, where I now get the chemo every third week. For 2 weeks, I’m pretty much back to normal, where I can exercise. I can maintain my weight program and just do the normal things that I’d normally do. Next week I’ll have my treatment. I know the reality is for a couple of days I’m going to be tired, and then I’ll be back to normal.
What guidance do you have for others about clinical trials?
Trust your group. Trust that they will keep you informed. I’m always a person that believes in gut. You’ve had those doctors that you go in, they don’t even look at you, and then they walk out, and you’re sitting there thinking, “What happened?”
I like the clinical trial group that I’m in. She will answer my questions, and if she can’t answer it, my oncologist and her physician’s assistant always will respond to me with whatever questions or concerns that I have and let me know, “This is what we’re going to do.”
Now I want to have a port put in my chest because I don’t have a PICC line. I said, “What are my options of having a port put in?” If you have those kind of questions, no question is a stupid question. Ask the question, and they’re going to give you an answer, one way or the other. It may not be the answer that you want, but they’ll answer.
I can prove to somebody else that it’s not a death sentence. If you have goals in your life, keep your goals.
For instance, they said, “You can’t drink alcohol while you’re in the clinical trial.” I’m not a drinker, but it’s funny. It’s like telling a kid they can’t have a cookie. When they tell you you can’t have alcohol, all of a sudden you’re like, “Today’s really hot. I would love to have a beer.”
You just understand that during the clinical trials there are certain things that they ask of you, and there’s a reason for it. I understand that they’re not asking you not to drink alcohol because they don’t want you to drink it. It’s because there has to be a reason. That’s why for me, it’s okay.
Going back to school and reaching goals
I was going to school, and I could have just said, “What’s the point?” I didn’t. It was a goal that I had put for myself, and I didn’t want the cancer to stop me from doing what I wanted to do. I got my bachelor’s, and then I wanted to pursue it. I wanted to get a master’s in a field that I knew at the time there would still be positions open.
I got my master’s in HR. Because of my work with cancer patients, I thought about getting a master’s in psychology. Maybe it would give me some little bit of insight into what’s going on with people, and maybe it might help me with talking to people.
It was hard because there were times when I had to take a leave of absence from school. By then, it was online. My bachelor’s was going to a classroom, but both master’s degrees were online, so that was easier. I still had to take medical leave.
One time one of the doctors at City of Hope asked me, “What’s the point?”
I said, “I didn’t want to give up just because I had a disease.”
I wanted to prove to myself that I could do it. I can prove to somebody else that it’s not a death sentence. If you have goals in your life, keep your goals. Do them, because you feel so much better to succeed. I also wanted to show my kids that you could go to college. You could go on with your life. You don’t have to let that hold you back. That’s one of the reasons why I got my degrees.
Cherylinn receiving her master’s degree in 2008.
Stem Cell Transplant
Autologous stem cell transplant
I got a stem cell transplant back in 2007. Ironically, I got that through UCLA. I used my own cells, so that’s autologous.
The doctor that I was working for at City of Hope, Dr. John Zaia, is a virologist. One day we just sat and talked about my disease. He’s the one who told me, “Your cancer is really aggressive. Why don’t you get a stem cell transplant?” I didn’t even know it was.
I called up my oncologist, and I said, “I have a bone to pick with you. Why didn’t you do this?” He said I did so well he didn’t think about it. Then he thought maybe this should be an option. Because of my insurance, he sent me to UCLA, and they did the test.
It was already 6 months after I had finished R-CHOP, and they were like, “Well, maybe we shouldn’t do this.” Dr. Pinter-Brown is just awesome. She said, “Let’s just do the test and see if you’re a good candidate.” It turned out I was, and that’s when they decided to go ahead and do the stem cell transplant.
[Testing] was blood work and an MRI to show that the cancer wasn’t back. They wanted to make sure that I was still in remission to do it, because normally a stem cell transplant is done within a month of when you finish chemo. This was like 6 months later, so that’s why it was like, “Let’s see if you’re still a good candidate.”
Stem cell transplant experience
It’s changed so much since 2007. In 2007, I was in the hospital in isolation for like 6 weeks. It was horrendous, because you get like 3 or 4 times the dose of chemo, so you have no immune system. I had told nobody to visit me because I didn’t want to take a chance. They said even if somebody sneezed and I was to get an infection, it’s life and death.
For me, it was really hard because I did have a lot of the symptoms. I had the cold sores in my mouth and a rash. At one point, it was so bad that I actually was put into a coma because the pain was just too bad.
It’s changed now because now people are doing outpatient. It’s changed so much since when I was in, because you had to be in isolation for like 6 weeks.
1st Symptoms: Lump on left-side of neck that grew bigger over a couple years, new lump on right side Treatment: 6 cycles Nordic chemo protocol, alternating cycles of R-CHOP and rituximab + high-dose cytarabine, autologous stem cell transplant
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
MCL Diagnosis and Watch & Wait
Introduction
Tell us about yourself
I’m a scientist by training. I’m a molecular biologist. I work in the biotechnology industry, in the patient advocacy space at the moment. I’ve done research for a number of years, and then I worked for a patient advocacy organization for about 10 years before joining the company I’m at right now. I’m married. I have a fur baby — no children, but a cat I love dearly. I live in Texas.
I’ve been in cancer research, so I’ve been in hospitals, I’ve been in cancer wards, and I’ve walked with cancer patients through their journey. But I was going in for me, and as I walked in and it was for me, it hit me in the face that they think I have cancer.
How did you discover you had cancer?
I have a metabolic issue that requires that I get blood work done periodically. At this point, it’s about twice a year. I was going in for a regular checkup, and they took blood. It came back with a high white blood count, which isn’t necessarily anything to worry about, but it was unusual.
They recommended I get it checked in a couple of weeks, so I did. It could have been an infection or something. I went back in a couple of weeks, and it was up a little higher still. Then they recommended that I get it tested again, and it was a little higher still.
By that point, I had followed up with my primary care physician, who let me know he was concerned about that and recommended that I see a specialist.
I was a little concerned because I had seen the white blood count go up, and the first one was a little bit high. The next one was just a little bit higher still. That third one was definitely high, and it was still going up, not coming back down.
He said, “This doesn’t look like a normal infection. You might have some sort of viral infection that you’re just taking a long time to get rid of, or there’s a number of other things it could be. I just would feel better if you would see a specialist.”
He did not at any point say, “Cancer.” It wasn’t in my head that he was thinking cancer, but I was a little concerned. I thought something was going on.
Realizing it might be cancer
He said, “This is the office I’m going to refer you to. They’ll set you up with an appointment, and you’ll go in.” I looked, and it occurred to me that it was an oncology office, but it didn’t really sink in that it was an oncology office until I was walking into the oncology office.
I think my background got me because I’ve been in cancer research, so I’ve been in hospitals, I’ve been in cancer wards, and I’ve walked with cancer patients through their journey. But I was going in for me, and as I walked in and it was for me, it hit me in the face that they think I have cancer.
I was a little surprised that it hadn’t occurred to me until that moment that this is what was happening. I was thinking it was some sort of an infection. It’s a high white blood count. It’s really not that big of a deal.
I didn’t really know much about blood cancers, but I knew a little bit about CML and some of the more common ones, so I was starting to think maybe it was something like that.
I knew I was doing what I needed to do, so I just moved forward even though I was quite nervous that day. At the point that it hit me, it really kind of threw me off my game. I was not going in in a good headspace.
Stephanie and her husband at Machu Picchu in November 2018.
Waiting for an appointment
All this happened toward the end of 2014. The holidays got in the way. By the time they made the referral, we had to get through the holidays and the new year and get in. It was a good about 6 weeks between when he said, “You need to see a specialist,” and when I actually got in to see the specialist, which is probably why I was not all that worried about it.
They didn’t seem all that worried about needing to see me very quickly. Once I saw him for the initial consultation, there were follow-up appointments, and those took a while for the same reason. It began to wear on me, I would say.
Once it occurred to me that they thought I had cancer, I was in a hurry for them to figure out what it was, and they weren’t in such a hurry. We need to figure this out because I need to do something. Why are you not in more of a hurry?
Undergoing scans and tests
Up until the point I saw the specialist, it had just been blood tests. They were looking at my white blood count. He did more blood tests, but he did significantly more blood tests. I felt like perhaps they were draining me of all my blood.
But he also ordered a bone marrow biopsy and a CT scan, just to see what was going on. He didn’t order the CT scan on that first visit. That was a follow-up visit. There were quite a few tests.
Then it turns out they were drawing all the blood because not only were they doing blood tests, but they were doing what’s called the karyotype to look at my genetic markers, because that’s eventually how I was diagnosed. I had a translocation. Two of my chromosomes had flipped, and that’s how they determined I had MCL.
CT Scans
The CT scan is just a long day. I don’t find it particularly difficult, and every one I’ve ever had has been in sort of an open unit. You do have to be alone in a room. They give you either something to drink or sometimes an IV infusion or sometimes both, depending on what they’re using as markers. It’s a radioactive marker.
You’re alone in a room because you’re suddenly radioactive, and they give you some guidance about when you go home. It sheds pretty quickly, but you have to be careful for a little while around your family.
Then you have to wait for like an hour while it works its way through your body, and then they take you in for the scan. The scan itself takes like 20 minutes. Usually you lay on a bed. They move you through and sort of coach you through the whole thing.
I don’t find that part particularly difficult, but some people don’t love being in the machine. I don’t like the waiting part. That’s the part that gets me. The first one was a CT scan. I’ve had several PET scans since then.
Bone marrow biopsy
The bone marrow biopsy is not fun. Basically they are taking a giant needle and putting it into the middle of your hip bone to take some of the marrow out. The marrow is what’s in the middle part of your bone.
It’s painful. I’m not going to lie. They will give you things to help you through it. Keep moving afterwards, because if you get still, you get really stiff and sore. I learned that the hard way.
They will often tell you things like Claritin or an antihistamine will help with the pain. I’ve heard people say that it did. It didn’t for me, so just know that. Not everybody reacts the same. I found Tylenol or Advil to be sufficient, but talk to them about that because it can affect other things that you might be on.
The Diagnosis
How did they use the tests to figure out you had cancer?
The tracer that you drink for your CT scan, certain cells in your body will absorb it faster than other cells. Those are rapidly growing cells. If you have a cancer, it will absorb it, and it will show up on the scan more than your typical organs.
There are a few other things that can show up, but they know what those are. They can look at them as background noise. That will tell them if you have, in my case, cancer in any of your lymph nodes or maybe in your spleen or wherever it might show up.
I didn’t on that first scan. Nothing showed up on the CT scan. But it’s one of the things they did to try to identify exactly what was going on and how much it had spread or how much it was through my body.
Stephanie and her husband in the Gulf Shores in July 2018.
The bone marrow biopsy was the same thing. They were looking at my bone marrow to see if it was infected with any sort of cancer cells. My bone marrow was showing some lymphoma cells in it.
That’s how I was originally staged with stage 4 non-Hodgkin’s mantle cell lymphoma. At first they thought it could be CML, which is chronic myelogenous leukemia, or a couple of other more common things just because of the way it presented with me.
I was still in denial. Maybe I was still thinking, ‘It’s probably nothing there. They’re just being careful.’
Translocation
In the blood test that they ran, they did a karyotype, and they looked at my chromosomes. Everybody has 23 pairs of chromosomes. You probably know X and Y. That determines your sex. You have 22 other pairs as well.
With mantle cell lymphoma, 2 of them trade places, and it’s a specific 2. They were looking at that, and with chronic myelogenous leukemia, a different 2 trade places. I ended up being diagnosed with mantle cell lymphoma.
That’s called a translocation when they move, and I had the one that’s typical for mantle cell lymphoma. Other than that, all I had was the high white blood count, and then it did show up in my bone marrow.
It was the first time when I went back for the results from all these tests. I was still in denial. Maybe I was still thinking, “There’s probably nothing there. They’re just being careful.” Then when he sat me down, he showed me. I ask a lot of questions, so he showed me all the results and explained everything to me really well.
All I could think about is, ‘I am not telling my mom on her birthday, and I can’t do this at the baby shower. So I guess I have to tell them on Wednesday.’
I would advise you to take somebody with you to any of these appointments, and I’ll get to that in a minute. Your brain will stop working, and you need somebody there that can ask questions. When he was like, “These results tell me that you have mantle cell lymphoma,” my brain clicked off.
The only other thing I could tell you that he told me was, “Do not go online and look this up.” So of course, what’s the first thing I did? It was to go online and look it up. He told me I had mantle cell lymphoma. My brain clicked off. I remember thinking, “I don’t want to die.”
He explained to me what some treatment options and things were. I couldn’t tell you what he said. I had to go back for a follow-up to sort of decide what course we were going to take. That’s the point at which I started paying attention to what the options were.
I’m married. The first thing I thought is, “Oh, dear God, I have to tell my husband.” Then the next part of that was, “And I’m going to have to explain it to him, because he doesn’t know cancer like I know cancer.” We have a very healthy, good relationship, and he’s very strong and supportive.
It took me a minute to be like, “Oh, I have to say this out loud, and I have to tell him.” When he got home from work that night, he knew I had a doctor’s appointment. He asked how it went, and I told him. He just sort of listened to me download how I was feeling about all of it.
Then he was like, “When are you going to tell your family?” Meaning my mom and my brothers and my sisters-in-law. This was in February, and it was the week of my mom’s birthday and the baby shower we were having for my sister. All I could think about is, “I am not telling my mom on her birthday, and I can’t do this at the baby shower. So I guess I have to tell them on Wednesday.”
He did recommend watch and wait. We talked about it more at that second appointment, when I actually could hear what he was telling me. I honestly hadn’t ever paid attention to watch and wait. It was something that was recommended for certain cancers, but in the world I worked in, it wasn’t really an option.
I asked a lot of questions. I was like, “What? Why are we not going to do something? You just told me I have stage 4 lymphoma. I feel like we should do something.” He did a great job of explaining to me that, yes, it was stage 4. I worked in breast cancer at the time.
He literally sat down and looked me in the face and was like, “This is not breast cancer. You have to trust me. Ask your questions. This isn’t the same thing. Just because you have stage 4 doesn’t mean you’re actively dying in the next short period of time. At the moment, it looks like you have a not-aggressive form that’s not spreading very rapidly. It will be better if we can watch and wait for a while, because once we start treatment, we’re down a path that we have to continue until you go to remission. We can’t just keep switching treatments forever.”
Processing not being in treatment
I understood that, but I didn’t like it all that much. We know that there’s something big wrong with me, and we’re not doing anything about it. I have to figure out how to just walk around knowing that I have cancer growing inside of me. But I understood why he made the recommendation.
I asked enough questions to get comfortable with that. He was saying the first choice would probably be chemotherapy. I was like, “I don’t really want to go through chemotherapy if I don’t need to go through chemotherapy. You can tolerate this.”
He was also really good and would check in with me and be like, “Some people just can’t cope with this, so if you really can’t cope with this, let me know and we’ll figure out a different path.” Just the fact that he would check on me and ask made me able to do it a little bit longer.
What questions do you recommend asking your doctor?
I think people worry about different things. I wanted to know what were the other choices? What does treatment look like? How long are people on watch and wait? How will we know if it’s progressing? I needed to do something. Those were the things that were bothering me, and so that’s what I asked about.
I did get a second opinion just to make sure that was the right approach, but they did also recommend watching and waiting between the 2 oncologists. They both had patients that were on watch and wait for significant amounts of time. I asked about that.
That also really helped me because I realized I didn’t know how long I would be on watch and wait, but it could be like 5 or 10 years. That was significant because, again, the other choice at the time was chemotherapy. If I could postpone that for 5 or 10 years, why wouldn’t I?
Finding an MCL specialist
He was local to me and at a good cancer clinic. It was certainly in a community setting, not an academic research institution. I live not close, but a reasonable distance from an excellent academic medical center, MD Anderson.
It’s super important for you to advocate for yourself. You know yourself.
I drove down to MD Anderson and got a second opinion there, and I picked MD Anderson because they have a lymphoma clinic. They have a couple of specialists there that literally focus on lymphoma.
The importance of advocating for yourself
It’s super important for you to advocate for yourself. You know yourself. You know if you feel comfortable with the decision or if you have any questions that are sort of lingering with you.
I would say you should always get a second opinion. Some doctors may give you a vibe, or you may feel like you’re getting a vibe that they don’t want you to. But by and large, they appreciate your involvement and your engagement.
Most oncologists at least will welcome a second opinion because they know that your life is in their hands, too. If somebody else sees something different, then they can collaborate and figure out what’s the best approach. If it’s the same recommendation, then that’s confirmation.
I’ve heard a few stories of patients that felt uncomfortable about getting a second opinion. I’ve never known a doctor to be like, “I hate it when a patient gets a second opinion.”
You’re making big decisions. I worked in the field, but this was not my area of expertise, and I was making decisions I didn’t have a lot of information about. More information is better, and if you can get a little bit more information, it just gives you a little bit more confidence about what decisions you’re making.
I did end up being treated at MD Anderson when I was eventually treated. I was very open with my local oncologist about it, and MD Anderson was very good at working with him. It’s not like I live in Houston. It’s a few hours away. They worked together. When I would get tests done at one place, they would send them to the other. I don’t know that it would always work like that.
In general, most academic medical centers (if you’re traveling to get there) are very willing to work with you locally and make it easier on you because the travel is not easy. I just felt more comfortable being treated at an institution that saw a good number of patients with what I had and had some experience.
It was blood tests every 3 months and CT scans every 6. I did both at my local center, and then MD Anderson recommended that I come back in a year just to get checked there again. I did a year of follow-up with my local oncologist, and then I went back to Houston and got that second CT scan done there.
Being on watch and wait for 1.5 years
When we talked about it originally, I asked a lot of questions and got comfortable with the decision, because I understood that we were trying to delay chemotherapy, but it was a hard year and a half.
This is not actually a normal symptom of MCL. I just happened to have this symptom: my white blood count continued to go up every single time. It went up a little bit sometimes, and it went up a lot sometimes.
Every time I was like, “Is this the day that they’re going to tell me I need treatment? Is this the day that they’re going to tell me?” I would wake up, and if I had a sore throat or I felt like maybe something was kind of swollen, I would be very worried. I would call and ask if we needed to have that checked out.
While I was comfortable with the decision, it was not a peaceful time at all. I was maybe a little hypervigilant compared to most, because I literally was worried about everything. They probably got tired of me calling and asking them if they need to check this out or what was going on.
Helpful tips for dealing with the wait
I would fall back on, “I’ve gotten the opinion of 2 doctors. They have experience with this. Other people have gone through this.”
I wasn’t really part of a support group or anything at the time. In hindsight, I probably maybe should have found a group to talk to, but I didn’t have one.
I would just sort of rely on all those reasons I had made that decision: that they were monitoring me, that they were seeing the same things I was seeing, and they still thought it was okay. I would talk myself down basically.
Healthy distractions
I did pick up my exercise routine a little bit, and I changed up my diet. “I’m going to give myself the best chance I can to prolong this as long as I can,” I thought. I went on an anti-inflammatory diet and was actually in pretty good shape. I have no idea if it did anything for the MCL or not, but it was good for me. It made me feel like I was doing what I could.
While I was on watch and wait, I was being seen by my local oncologist, and they were doing regular blood tests and then periodic CT scans. I had had the 2 CT scans locally and then realized it was time that I needed to go back to MD Anderson to check in with them.
I made an appointment with them, and my most recent blood test from my local oncologist was quite high. My white blood count was 125. I was a little worried about that. I really felt like even though it absolutely was time for me to go back to MD Anderson, I was sort of prompted to go because I wanted to just get the second opinion again.
This time they did the same workup. They drew the blood again. They did another CT scan, and they did another bone marrow biopsy. Not only was my white blood count quite high, but my spleen was significantly enlarged and showed up on the CT scan, which hadn’t showed up locally. My bone marrow was significantly more affected.
We had the conversation about treatment because they were most worried about my spleen. I’ll admit it. Having now seen the picture, it was quite enlarged. I didn’t really notice anything. I just felt a little full when I would eat, unusually full. That’s because it slowly got larger, and I didn’t really notice until they saw it on the scan.
How did you react to the idea of starting treatment?
As I had mentioned previously, every time I sneezed, I basically was like, “Is this it? Is this when I need to go for treatment?” My first reaction was, “This is what it’s like. Now it’s time. We’re here.” I had also told you that when I was first diagnosed, the option had been watch and wait or chemo.
My immediate thought was, “Now it’s time. Oh, crap. I need chemo.” I was quite scared about that. I knew we needed to treat the cancer, but I also know what chemo can do to you. I was not very happy about it. Plus, then what about my job and all this other stuff I have to do?
Exploring a clinical trial as a treatment option
This was at MD Anderson with my oncologist there. He’s a research specialist, and he explained what the treatment choices were. He also explained that there was a clinical trial. He had started it as a smaller trial, and he had just gotten approval to expand it to double the number of patients. It was originally 50 patients, and he got approval to double it to 100.
Of course, I was interested because I have a research background, and that’s what I do. The beauty of this clinical trial was testing a combination of 2 targeted therapies, or drugs that we call biologic drugs.
It’s not chemotherapy or chemicals that kill basically anything that’s growing. It’s kind of like carpet bombing your body, but it kills the cancer. Biologics are more targeted. They find something specific about the cancer cell and attack that. They can occasionally have some side effects, but it’s not the mass toxicity that you get from chemotherapy.
This was a combination of 2 of them that I asked a million questions about. The data looked like it was a good combination that would be effective. After you responded to those drugs — assuming you responded to those drugs — then they would follow with just a couple rounds of chemotherapy, because they have to offer you the standard of treatment.
Something that a lot of people don’t necessarily understand about cancer clinical trials is that you have to get at least whatever the standard of treatment is, and you usually get more. It’s more screening, it’s more follow-up, and it’s an additional drug. There’s no placebo.
There are 8 drugs in the chemotherapy, yet it’s an A/B cycle. Cycle 1, you get the A drugs, which there’s 4 of. Then cycle B, you get the other 4 drugs. Then you go back to A, and then you go back to B.
Hyper-CVAD will take the disease down, but it won’t knock it out. It was unheard of to get to full remission with hyper-CVAD.
It’s an infusion. It’s a 4- to 6-day infusion, depending on which cycle it is. Then you have 3 weeks off, and then you go back for the next cycle. It’s the more aggressive of the chemotherapy treatments for MCL, but because I was younger and pretty healthy otherwise, that was what they were recommending for me.
If I had been an older patient, they probably would have picked a different regimen because hyper-CVAD’s tough. It’s the same regimen they give you if they’re doing a bone marrow transplant.
First of all, when you’re considering a clinical trial, keep in mind that yes, it is experimental, but in the cancer world, they believe it’s better than the current standard of treatment.
I would ask why they think that? What are the data? You may not care about that. I did, so I asked a lot of questions about, “How’d they come up with this combination, and why do they think this is better, and what are the outcomes with just the hyper-CVAD?”
For a lot of other people, they just want to know why they’re recommending this clinical trial. “How many other people are in the clinical trial? Are there people like me in the clinical trial?”
I was a young woman with what is most commonly an old man disease. He was quite excited to possibly have a woman in the trial, and then he asked me to help recruit other women into the trial after I had joined.
I really wanted to know why they thought this would be better than what the current treatment was. What he told me at the time was hyper-CVAD will take the disease down, but it won’t knock it out. It was unheard of to get to full remission with hyper-CVAD.
Enough people in that first 50 reached complete remission. They really thought that they could at least get you to complete remission. They didn’t know how sustainable it would be, and he was very honest with me about that.
For me, that was it. If you can’t get me there with this, but you might be able to get me there with that, I’m going to try it because that’s better. You also need to be comfortable with the fact that it’s research.
Resources
The Leukemia & Lymphoma Society has a great resource for learning about clinical trials and even has prepackaged questions you can print off and ask your doctor. The Lymphoma Research Foundation also does. Theirs is a little more specific for lymphoma because that’s what they focus on. These are great resources.
Don’t hesitate to ask questions. Everybody has questions about clinical trials. I asked so many questions that he actually took me into his office and pulled up a presentation he had just done at a scientific meeting and basically gave it to me to answer my question.
Stephanie with her MCL group.
Treatment options after hyper-CVAD
He did explain that he would start with the hyper-CVAD chemotherapy. It would knock it down. We would go back to the watch and wait pattern. He was like, “I don’t know. It could come back quickly. It could come back slowly like it did before. You can have another 2 or 3 years between now and needing your next round of treatment.”
He’s like, “We could try hyper-CVAD the next time, but odds are if it grew back after we gave that to you the first time, it’s not going to work so well. We usually go to a second kind of chemotherapy the second time, and then that knocks it down. Then you go back to watching and waiting.”
At that point, it’s a game of, “Can the chemotherapy regimens keep you going long enough to have a full life?” But you’re also building up all the different treatments and toxicities, so that’s not pleasant.
Stem cell transplant was an option. He was like, “At some point after the chemotherapy, we’ll talk about the stem cell transplant.” They could harvest my own stem cells and put them back in, or it could be from somebody else. We would talk about that then.
Really, those were the choices. It was sort of this life of going through chemo, watching and waiting, going through the next treatment, watching and waiting, hoping something was sustainable or at least sustainable enough that I could make it to my 80s.
Clinical Trial
Choosing the clinical trial
Realizing it was experimental, you could not say for sure what was going to happen in my case, but there was enough data from these previous people who had participated in a trial to suggest that they could at least get me to complete remission.
Stephanie starting clinical trial treatment for her MCL.
We wouldn’t know how long that would last, so it might end up being a very similar cycle. When you’re starting from nothing, it feels at least like you have further to go until that next treatment than if you’re starting halfway there, for lack of better terminology.
Rituximab and ibrutinib process and side effects
The rituximab is an infusion, so I had to go in. They have to ramp you up to it. They checked me into the hospital. They started me on basically an IV slow drip of Rituxan. I had a pretty classic but pretty aggressive reaction to it at first.
It can trigger something called the rigors in you, which affects basically your whole body. It’s like you have a really bad fever and the chills that you get with a really bad fever. You’re just balled up and shaking. They clocked that right away, buried me in warm blankets and gave me something to counteract that. My husband tells me it was only like a minute or so that I was going through the rigors. It felt like half an hour to me.
Then they slowed the drip down. That first one, to get the whole dose in, took actually 2 days for me. That’s pretty unusual. They had to slow it down quite a bit. Beyond that, they then would speed it up. Eventually, it got to the point where the infusion would be like 4 hours.
I would just go in at first every 2 weeks, and then it was once a month for the Rituxan infusion. For that first month, I was only on the Rituxan. Then they added the ibrutinib. The ibrutinib was a pill, and it was just a pill that I took every day. One pill once a day.
I could go about my life other than having to go for this infusion once a month that, like I said, did only take 4 hours most of the time. I was able to work through the whole thing. I had enough leave time that I could take days off to go get the infusion, and my company was really good about it. I would hope they would be; they’re a cancer organization.
I sort of proactively talked to HR about what it would look like if I needed to take leave, because I didn’t know how I was going to feel at all or how much I was going to need to be in and out of the hospital with this treatment. Early on, we walked through what work would look like.
I just declared this day the celebration day, and then the next day I worried about chemotherapy.
She gave me the paperwork and told me at whatever point I wanted to go that route, just to fill the paperwork out and give her a call, and she’d help me get it filed and stuff. Super supportive there. I’m probably jumping ahead, but I ended up doing intermittent family leave for the chemo portion of my treatment because I was in the hospital for a week at a time.
Every month when I would go for my infusion, they would do blood work. At first they just did the blood work to see how I was responding. They would look at my white blood count. They would look at a few other things to see how I was responding to the test.
Then 3 months in, they did another bone marrow biopsy to check if my bone marrow was responding to these biologic drugs. My white blood count was significantly down and my spleen was down back to normal size, but my bone marrow was still showing some mantle cell lymphoma. I kept going on the biologic.
Then at 6 months, they tested again, and I had had a complete response. My white blood count was below normal now, and my bone marrow was completely clean. Nothing showed up on the scan — my spleen, no lymph nodes, no anything. I had had a complete response. They declared me in remission.
Now it was time for phase 2 of the trial, which was the chemotherapy. Because I had reached complete remission, I only needed 4 months or 2 full rounds of the chemotherapy. It could have been that or 8 or 16, depending on what your response had been to the first part. I got lucky. I only needed the short version.
I was ecstatic. I had a party when they declared me in remission, literally. I just declared this day the celebration day, and then the next day I worried about chemotherapy.
Chemotherapy
Undergoing hyper-CVAD
I knew what I was doing when I signed up for the trial, but I had maybe underestimated the significance of knowing that I didn’t have cancer in my body but still going to go through chemotherapy.
I am glad I only had 4 rounds. It was tough. It got progressively worse. The first month with the A cycle, I handled it pretty well. I had sort of my contingency plan in place, because I wasn’t sure when I got out of the hospital if I was going to feel like going to work or if I was not. I was able to work. I went back to work the very next day and mostly was fine.
Stephanie starting chemotherapy in July 2017.
The B round, I suffered more in general. It left me feeling pretty sick. Most people, it’s the other way around, but I got nailed with the B round. I still worked the whole time unless I was in the hospital. Frankly, I could have worked when I was in the hospital getting an infusion. My company didn’t want me to, so I took that time off.
For A round, I would go in 5 days pretty steadily. It’s 5 days. They sequence the drugs. They start you on 1, and then they add in the next. You’re hooked to an IV the whole 5 days.
Taking walks
You can move around. I knew the guards at the hospital, and I’d go down to the coffee shop to get a coffee and see what was going on. I could walk. My husband made me walk. He was like, “You’re not going to lie in this bed and just waste away. You’re going to get up and walk.” We mapped out a route with the crosswalks and things that was 2 miles. I walked at least 2 miles every day with my pole, who I named Fred. He was my dance partner. I was okay.
The B round, like I said, I got sicker with that one. That’s when I learned about anti-nausea drugs and all the things that they’ll give you to help with side effects. I weathered through that pretty well, too. I kind of felt like I had the flu with the B round, but I still would get up and walk and do everything I could.
Then the second A round was a little bit worse. The B round was a little less predictable. It was actually 4 days of an infusion, but you had to clear 1 of the drugs out of your kidneys before they would let you go home, because it could damage your kidneys. That can take anywhere from 24 to 72 hours. It could be 5 days. It could be 6 days. It could be 7 days.
I was pretty lucky. It cleared out of my system pretty well. The first time I was in, it was 5 days, and they let me go home. I had trouble clearing it the second time, so I think it was 7 days before I could go home the second time.
Treating side effects
Zofran was my best friend. I discovered coconut oil for mouth sores. They’ll tell you baking soda, which kind of works. But if you swish coconut oil around your mouth, it takes them right away. It’s amazing.
At that point, they give you drugs. They give you the drugs, and then they give you the drugs to counter the side effects of the drugs, and then they give you the drugs to help you sleep.Just embrace it, because you need to manage what’s going on in your body, for sure.
The hair loss was a side effect of 2 of the drugs in the A regimen. I got through my first A regimen, and then 10 days after I went home, my hair started falling out. What they didn’t tell me was it would hurt. The hair pulling on my follicles, I guess. It hurt. I actually wanted it to go away because it was not a comfortable thing.
When you’re going through this journey, you have to celebrate even some small things. You just still need to find that joy and some way to bring it out.
My husband actually shaved my head for me. I didn’t go to a hairdresser. I just had my husband shave my head. He couldn’t do it the first time. We had to try again the second night. I wasn’t bothered at all. It bothered him a lot. But we got through it. He did a great job.
Turns out I have a really good head. I did not opt for a wig. I was bald or used head wraps the whole time.
Then my “you got through chemotherapy” gift to myself was that I got a henna crown after my last round. It was something I wanted to do. I had seen them. I thought they were beautiful, and it was a celebration for me. I happened to finish chemo at the end of October, and my birthday’s in early November, so that was my celebratory gift to myself.
I have a couple of friends who did henna pretty regularly. They’re of Middle Eastern descent. I called to see if they knew anybody that would do a crown for me. They knew somebody that would do the crown for me, and they came with me. We just had this very special, meaningful night.
It took about an hour for the woman to do my head. I didn’t really have any specific guidance for her. I just wanted something beautiful. I showed her a couple of pictures of things I liked, and she free-handed the whole thing. Then my friends got their hands done, and we have a couple of pictures of us together afterwards.
Then my husband picked all of us up, and we got some food at a local Middle Eastern place. I walked in, and immediately they knew. They just were like, “What a beautiful crown.” I just started crying because they were celebrating with me.
Celebrating the small things
For me, it was bringing some beauty out of some tragedy. You don’t have a completely bald head all that often in life, so I might as well make the best of it. That’s my favorite thing. It really was very healing for me to do that.
People think it’s odd, but it’s one of my favorite pictures of me. There’s one I’m kind of looking down, and you can just see the head. There’s a big flower right on the crown of my head. That’s sort of the crown part of the crown, if that makes sense. For me, it just is really a sign of life. Life came out of everything I had just gone through.
I believe in celebrating things. I told you I had a party after I finished round 1, and I believe in celebrating things. When you’re going through this journey, you have to celebrate even some small things. You just still need to find that joy and some way to bring it out.
Follow-Up and Lessons Learned
Follow-up after treatment and chemotherapy
Once I completed the chemotherapy, I had to go back a month later. I went back in November just so they could check how I was recovering from the chemotherapy and how everything was going. They did another set of blood tests to make sure I was still in remission and it wasn’t boomeranging — or whatever it’s called when you stop treatment, and then it comes back. I wasn’t.
Then after that, every 3 months I would go back for blood tests and a PET-CT scan. I haven’t had to do another bone marrow biopsy since the one was clear, and I’m very grateful for that. Then I did every 3 months for a couple of years, and then they pushed it to every 6 months.
This fall I will be 5 years out, so I haven’t been since last August. I’ll go back this August, and then I will officially have completed the trial. I will still go back for tests to follow-up for another 5 years, but the trial itself will be completed, and my data will count.
What does it feel like looking back?
That was a hard year. I don’t want to in any way say that wasn’t a hard year, but I learned so much about myself. I’m very grateful for that year. It sounds a little weird to say that, but I learned about myself.
This is your life. You know what you want to do. You know what you need to do.
I learned about other people. People came and showed up in ways I never would have expected — to help and support and help me get through that, to help my husband help me get through that.
I am very grateful to be on this side of it. I’m 5 years out, and I haven’t had any signs of any kind of recurrence. I feel like I made a really good decision about joining that trial.
Dealing with scanxiety
Scanxiety is very real. I think knowing that it’s real and acknowledging that helps, but it’s still real. I’m cranky for a couple of days before a scan. I don’t necessarily always recognize it, but I’m just definitely on edge, because I’ve already gotten that bad news once. In the back of your head is, “What if it happens again?”
The way I cope with that is just, “You made it through once. If you have to do it again, you will get through it again. You can do this. It’s okay.” It doesn’t make it less hard to cope with. The days after counterbalance it because you know you’re clean. You know there’s no more sign of cancer in you. You can relax as much as you were anxious for the days before. It all balances out.
I hope what you heard me say is just don’t be afraid to ask questions. Don’t be afraid to advocate for yourself. This is your life. You know what you want to do. You know what you need to do. You know how you make decisions. You make sure you get what you need to do that. That’s what I believe.
1st Symptoms: Lump on left-side of neck that grew bigger over a couple years, new lump on right side Treatment: 6 cycles Nordic chemo protocol, alternating cycles of R-CHOP and rituximab + high-dose cytarabine, autologous stem cell transplant
Jason is a New York entrepreneur, tennis player, theater-goer and traveler who says he loves the lights of Las Vegas.
Things shifted in 2019 when Jason, at only 39 years old, was diagnosed with stage 4 mantle cell lymphoma, a rare blood cancer that is more common in men over 60 years old. His diagnosis almost turned his world upside down, and he was thankful he had become an entrepreneur prior to his own treatment.
In this video series, Jason shares his story of diagnosis, clinical trial, treatment and how cancer changed his life. His story is such an inspiring example of patient self-advocacy.
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
VIDEO: The Mantle Cell Lymphoma Diagnosis
His blood work and everything seemed normal. Except for the increasing itch and pain from hives and inflamed arms, Jason and his primary doctor thought it was nothing serious.
Specialists couldn’t find anything until he was referred to a hematologist. A bone marrow biopsy and PET CT later confirmed cancer. Jason was diagnosed with mantle cell lymphoma at a very early age of 39.
About me
I’m in New York City, and pre-cancer diagnosis, I was an entrepreneur. I guess I still am, and I have a small business. I’m a tennis player, a theater-goer. I like to travel. I like to gamble. I go to Las Vegas pretty regularly. I’m most passionate about my business, which is a production supply and walkie-talkie production services company in New York City and Greenpoint, Brooklyn, which is a great neighborhood in New York City.
I’ve been in video production services for over 20 years. In 2017, I started my own company after being a freelancer for many years. That was actually kind of a magical experience because if I didn’t start my company, I don’t know how I would have fared this storm.
If I was still in the freelance world, producing shoots or working for somebody 40 hours a week, I think that I would have some pretty significant challenges dealing with the cancer diagnosis and the treatment and the ongoing treatment. Being an entrepreneur has been very lucky and fortunate for me.
It was about 2.5 years ago, the summer of 2019, and the very first symptom was on my arms. I was getting a rash. It was very red and bumpy and itchy. It started on my forearms, and I really didn’t think much of it for the first 2 or 3 weeks. I really didn’t think much of it at all.
I was out to dinner with a very close friend of mine, Adrian, who happens to be a doctor himself. He’s a hospitalist at Weill Cornell, and he’s a really great doctor and a really great friend of mine. We were meeting up for dinner, and he said, “What’s on your arms?” I said, “I don’t know,” and he’s like, “you should have it looked at.” I said, “Yeah, I don’t think it’s anything to worry about.”
Another couple of weeks went by, and it was still there. His comment was sort of in my head, so I made an appointment with my primary care physician. I’m probably going 5 weeks after the first sign. I go into the primary care office, and at this point, there’s hives on other places than my forearms.
Mantle cell lymphoma diagnosis
The primary care physician says, “It looks like hives to me. Hives are really common. We get a lot of people in here with hives, and we run all sorts of tests and are looking into it. Most of the time, they just go away, and we never really figured out what it was.”
We talked a lot about it, like “Did you change your detergent, or did you change your soap?” Then he took a lot of blood and ran my blood work.
He’s a wonderful doctor. I love my primary care doctor. I still have him today.
He called the next day. “We got your blood results back. Everything looks perfect. Hopefully, this just goes away.”
I said, “Oh, great, blood work came back great. Hopefully, this will just go away.”
Time went by, and it started getting worse. It started spreading to other parts of my body. It started becoming more itchy, more inflamed. It went from just being on my forearms to being all over my chest and all over my stomach and down my thighs. It just sort of progressed.
I went back to see him again. He said, “I’m not quite sure with your blood work being right what it could be. Why don’t we look into going to an allergist, immunologist, rheumatologist-type person and a dermatologist?”
I went to somebody who had a specialty in all of those categories —allergy, immunologist, rheumatologist. We ran blood work like I’ve never experienced. The number of vials of blood that I gave and the number of tests that I did over the course of 2 months with this person was just over the number. The bill was also over the top. The only thing that came back was an elevated IgM. That was it. That was the only thing that came back irregular in my blood work.
The dermatologist initially said, “I don’t think these are hives. I think it could be something else.” While everybody thought it was hives, he said, “There’s a chance it could be this. It’s a rare thing. Let’s biopsy a few in a couple of different places on your body.” He biopsied, I think, 4 areas.
We ran blood work like I’ve never experienced… The only thing that came back was an elevated IgM.
Describe the biopsy
It’s like a punch biopsy, where they basically think you have one hive that’s sticking up. They just take the whole thing and then send them to a lab.
They took 4 — took 2 off my back and 2 on my stomach, or something like that. Those came back as urticaria vasculitis, so that is hives. The vasculitis meant there were hives not only on top of my skin, which are traditional hives, but also under, in the derma.
I was getting hives basically on both sides of my skin, the exterior and the interior. We’re 4 or 5 months into this with me having hives, and they’re just progressively getting worse. There were some sleepless nights. It was unbearable not to itch them, and then it would create scabbing and blood. My sheets were tinted with blood spots.
It was painful. There were a few nights when the pain level was an 8 or 9. Looking back, I can’t believe I didn’t just go into the emergency room.
Looking back at what I was doing — laying in a bathtub and trying to throw ice all over me, doing all of these things to try and come at it — I should have just gone to the emergency room.
This young girl comes in and tells me that we’re doing a bone marrow biopsy. She explained it to me, and I literally started crying.
Understanding pain tolerance level
The dermatologist gave me steroid cream, which was helpful. I put that all over, and it was really helpful.
As we were going through the diagnosis process, eventually I landed at a hematologist. The allergist-immunologist said, “I have to send you to a hematologist because you have an elevated IgM, but there’s nothing wrong with you. I assure you your blood work looks so great. But we have to do it. It’s called a rule out.”
I went to the hematologist, and I’m there for a rule out.
What’s a rule out? I don’t know what a rule out is. I went into the office, and they put me in a room. The PA (physician assistant) to the hematologist that I had an appointment with comes in and is very cheerful and says, “Do you know we’re doing a bone marrow biopsy today?
I was like, “What? What is that? I’m going in there for a rule out. I don’t even know what that word means.” Then this young girl comes in and tells me that we’re doing a bone marrow biopsy. She explained it to me, and I literally started crying.
What in the world is going on here? Then the doctor came in (the hematologist), and I’m crying, and she’s trying to talk me down. I said, “Look, you guys didn’t tell me that this is what’s happening. I could have mentally prepared for this. I could have brought my friend. I am not doing this today.”
How did the bone marrow biopsy feel?
For me, the gravity was maybe more extreme than most people.
I watched my mom die of cancer. She died when I was 19 years old. When I was in that room, I didn’t think I had cancer. I thought I was going to a hematologist for a rule out.
I’m sitting there crying and upset, thinking, “Is this person thinking that I have cancer? Now I have cancer?” This hematologist is saying, “This isn’t that.” That was what she kept repeating. “What your mom went through — this isn’t that.”
They hadn’t diagnosed me, and it was supposed to be a rule out. I don’t think at that point anybody thought I had cancer, and that’s what I found along the way.
It was like, “I’m sure you’re fine. Don’t worry about it for like 5 or 6 months.” But actually, there was something very big to worry about.
For me, the emotion that was coming from there was, “I’ve seen people battle cancer. I’ve seen people die from cancer.” My mom wasn’t the only family member that succumbed to the disease. I have many aunts and uncles that have passed away from cancer.
I was very close to my mom. I was young and in high school during all of her treatments, witnessing all that. That was in the 90s. A lot has changed between now and then. I have to say, it was probably a lot worse to have cancer in the 90s than it is in the 2020s, based on what I witnessed when I was a younger person.
At that moment, the tears and the emotion that were happening in that room were like, “I’m in a hematologist office with this person who thinks I have cancer because they want to do a bone marrow biopsy. Here begins the torture.”
I had always said after witnessing my mom go through all that that I would never do chemotherapy. After I saw that, I said, “I’m never doing that.”
I haven’t done traditional chemotherapy, and it was a big part of my decision-making. To avoid it was probably historical.
My mom battled breast cancer for a long time. She had the initial cancer reoccurrence twice. Then I think she was battling it for that third time, but it had spread to her sternum. Then, from there, it went up to her brain. That’s ultimately how she went from cancer.
Guidance on people on PET-CT scan
They had basically said, “Okay. When can you come back?” I said I’ll come back in one week, and they said, “Okay, well, we also want you to get a PET-CT.”
I don’t know anything about a PET-CT. I don’t know what it is. Nobody tells me. I go, and I’m by myself.
There’s a nurse, and he’s very nice. I’m asking a lot of questions. He’s got to put an IV in me. I’ve never had an IV before in my entire life. He was asking me if I’ve ever had this done before, and I said no. Then he starts explaining what he’s going to inject in me. I said, “Is this dangerous? This sounds dangerous. Is this bad for my health?” It’s not something you should do. It is radiation and radioactive material.
He said, “If your doctor has ordered the test, then it’s probably really important that you do it.”
I said, “Okay, that makes sense.” But I had no idea what was going into it.
There was a lot of that — the first time going to the doctor’s office, going to the infusion center, getting a PET scan and getting a bone marrow biopsy. It’s really scary that first time. The buildings look so different the first time I go from the second time I go.
The first time I go, I just have this scary memory of them. Then as I go back over and over again, it fades, and they seem like normal places to me. But I can always remember the first time I go to a building and get that first thing I’ve never done before. It’s just like a very sterile, scary kind of situation, but it seems to fade away after you do it the first time.
Describe the PET-CT scan
They set the IV and inject you with something that I still don’t 100% understand.
I’ve asked a lot of questions about it, but it’s like I get a piece of paper here in New York City that I have to carry around with me because they have monitors in the subways looking for dirty bombs, like radiation bombs. If you get a PET-CT, there’s a chance you can set one of those off, so I get a piece of paper walking around New York City.
They tell you don’t hug children for the first few hours when you’re done with it and drink a ton of water. You sit there for an hour in an isolated room. From the looks of it, the room is meant to keep whatever you’re radiating from your body from other people.
It’s a very lonely hour. You’re not allowed to bring a friend because you’re emitting something. When they’re guiding you in, they almost put some space in between them and you. Nobody’s getting close to you during that process and for a little bit after. Then, after the hour, they call you in.
They also will have you drink a substance while you’re waiting. I can’t remember what it is exactly. It starts with a G, but it’s basically sugar water.
It’s a very lonely hour. You’re not allowed to bring a friend because you’re emitting something. When they’re guiding you in, they almost put some space in between them and you.
You’re getting the injection of something going into your veins that helps them see imaging of your organs and lymph nodes. Then you’re drinking something that’s probably insulin or glucose-type base that’s going throughout your whole body. That’s sort of the magic for making the imaging.
You do that for an hour. You sit there, get an injected, drink all the juice. Then they bring you in, and you go lay down on a long, little table. Then they send you through a tube.
For me, because I’m stage 4, my lymph nodes are from my groin to neck. My scan probably takes longer than most people’s, depending on the type of cancer you have. For me, they start on my thighs, and then they go up to my ears. It probably takes about 28 minutes to do that scan.
You just sit there and don’t move for 28 minutes. Then they let you go with your piece of paper to get out of jail if you set off a New York City MTA radiation monitor.
Dealing with scanxiety
It’s not just about scans. It’s just that waiting period, essentially for any results or even before the procedure.
I’m not a fan of bone marrow biopsies. I don’t like them, and I will definitely be kicking and screaming if I have ever to do another one. We’ll need to work on some other ways of either medicating me more or making the experience better for me, because I don’t know if people know exactly what it is.
Still, they’re essentially taking a very long needle and jamming it into your lower back and going straight into the bone to the core of it and removing some marrow. At the same time, going back in where they went in and taking what’s called an aspiration, which is a small amount or a tiny piece of the bone as well. Sometimes they’ll even get marrow from 2 different spots.
I can’t imagine anybody would want to do that. I don’t like the experience at all. I’ve done 2 of them. I’ve done the Ativan (lorazepam) stuff. It wasn’t enough for me.
I always say I’m done collecting bad memories of bone marrow biopsies. If they want to do another one, we’re going to have to work something out. I don’t want to do it under the circumstances I’ve done the last 2.
I had a long wait to get into actually meeting my oncologists who I have now.
The hematologist who did the bone marrow biopsy — the first one who was doing the rule out with the PET scan — had sent my bone marrow out to the lab to see what it was. Before it went out, she said she took a smear of it, put it on a slide and looked at it under a microscope.
She said, “I can tell for sure you have B-cell cancer just by looking at it. I’m a myeloma doctor. I’m referring you to the Lymphoma Center. The bone marrow from the biopsy is being sent out to the lab. Your PET scans are still going through, but you need to call the Lymphoma Center. I referred you to somebody because I don’t do that. I do myeloma.”
Hearing and processing the news of cancer
It was literally on the phone with a doctor. I didn’t have a relationship with the same one who said, “This isn’t that.” It was a hematologist that I was sent to do a rule out.
It all happened very fast, and it was very shocking. I had no idea, and I would have never guessed that I had cancer.
It was hard doing the rule out. I thought I had to do all these horrible things just to appease the rule out. I was still in the belief that all these other doctors telling me, “Look, your blood work’s perfect. I’m sure you’re fine.” I had so many doctors tell me that, from the dermatologist to the immunologist allergist, my primary care.
So many people were like, “I’m sure it’s probably just something immune, autoimmune.” In my mind, I just think, “Oh my God, I have to do these 2 horrible tests to help figure this out, but I do not think I have cancer.” That wasn’t what I was thinking at all.
When she said it, it couldn’t have been more of a shock. I was completely in shock. There wasn’t a lot of conversation. After that, it was just 1 or 2 questions. Her responses were like, “I’m not a lymphoma doctor. You have to call the Lymphoma Center.”
I got information that I had cancer, but then I didn’t really have anybody to ask follow-up questions. There’s a lot of B-cell cancers.
My friend who was a doctor, I called him. He’s such a great friend. He came over immediately within an hour, and we were able to talk, like, “Well, there’s some ones that aren’t that bad.”
We were going through the list. He was trying to talk me down a little bit. When I called the Lymphoma Center, they said, “We’re not seeing you until you have a lymph node removed. We’re going to need one in order to diagnose this formally.”
That period was 4.5 to 5 weeks from, “You have cancer,” to “What is this?” I had to find a surgeon, schedule an appointment with a surgeon to meet before surgery, then schedule a surgery. Then it goes out to a lab. They couldn’t have told me more times, “It literally takes a week. It takes 5 full days. It’s not going to come back any sooner. We assure you, 5 days is the earliest.” Then from there, then I have to get an appointment with the doctor to get the results.
It was a good 4.5 to 5 weeks of just complete anxiety. Those were definitely the worst weeks. The not knowing what my outlook is, what my prognosis is, what is going to happen in terms of treatment. Those were the worst.
The terrible part of it was the anxiety part that you sort of hinted at it when you’re waiting to get the scan results. That’s what made it so terrible.
The meeting with the surgeon and the appointments — all of that wasn’t a bad experience. I felt like I navigated it as fast as I could within the system. You call to make a prelim appointment with a surgeon on a Monday, and you get in on the next available — might be Thursday. You meet Thursday.
Then you got to get on the surgery calendar, which could be 1 day or 2 days a week because they’re meeting with so many people for pre-op and post-op. The surgeon just might schedule surgeries 1 day a week or 2 days max.
I understand the idea of just checking to the emergency room, but how much faster could it have been? I don’t know if that would set it up for me.
Describe the moment you got the results
The worst day was getting a phone call from the hematologist saying, “You have some B-cell cancer. I don’t know what it is.”
That was the worst day. I was crying and thinking, ‘This is it.’
Going in to get the formal diagnosis and meeting my doctor for the first time was a very long visit. I brought 2 friends with me. One of them was the doctor, which I’m very grateful for. We were there for a good 3 hours, and I had a ton of questions, collected over the 3 or 4 weeks that I was waiting.
My doctor, who’s at Weill Cornell, Dr. (Jia) Ruan said, “You have mantle cell lymphoma.” She explained it, and I immediately felt very lucky because the hematologist had referred me to the Lymphoma Center at Weill Cornell, and there’s a handful of doctors there.
The one that I just randomly ended up being assigned to happens to be the one specializing in mantle cell lymphoma. That was like a miracle in a way, because of the options there. I didn’t really pick. They just referred me to somebody. I just accepted the referral. That seemed magical. I got the exact right doctor that I should be seeing.
VIDEO: Treatment & Clinical Trial Experience
Jason used to be afraid of needles and procedures. Watching his mom go through breast cancer treatment through chemo, he was determined to try a different course of treatment.
Luckily, Jason got into a clinical trial introduced to him by his oncologist that turned out to be effective for him.
Treatment decision
My doctor said the traditional path to treat mantle cell lymphoma would include R-CHOP chemotherapy and then, depending on the result, could potentially be followed with a stem cell transplant. She said that she had another option for me, which was a clinical trial that she happened to be heading up for mantle cell lymphoma.
This felt very magical to me. I landed with this doctor who specializes in it, and now she’s also heading up a Phase 2 clinical trial.
She had presented both options. I knew instantly I wasn’t going to do the R-CHOP chemotherapy, because I told you I wasn’t going to do what I saw my mom did at that moment.
My friend who was a doctor was there with me. We asked a lot of questions. He asked a lot of questions as well about the clinical trial. She left the room, and I turned to him and said, “What do you think?” I just wanted his opinion. But in my mind, I already knew I was not doing that R-CHOP stuff.
He said, “I think you should do the traditional route. There’s just more data. They’ve been using it more. We know it works.”
I said, “I think I’m going to go the other way.”
She came back in, and I asked a lot more questions. They presented me with a stack of papers, like a contract. I read through it all.
I sat there for like another hour, just contemplating which one to do. Then before I left, I signed all the paperwork for the clinical trial. She said, “All right, come back in a week from today, and you start.”
So that’s how I started.
Describe the cycles
For the first 4 weeks, you get Rituxan every week, and then after those first 4 weeks, you will get it every 56 days after that. The other 2 medications are both oral, but the Rituxan is infused. You go to the hospital, to an infusion center, and do that.
The first 4 weeks were back to back, 4 weeks in a row. Ever since then, I just go in every 56 days. I take acalabrutinib every morning and every night, every single day, and I have for over 2 years now.
For the lenalidomide, I take it like birth control. 21 days on, 7 days rest. I’ve been doing that for over 2 years now as well. The first year, I took 20 milligrams of lenalidomide, and then for the second year, they let me reduce the dose to 15 milligrams. Basically a 25% reduction of that drug to give a little break and hopefully reduce the side effects by 25%.
Describe the difference in side effects
It’s so hard to measure them. But I do remember that the first year was way harder.
I remember in the beginning — the first 6 months — were way harder, and I don’t know if that’s you just get used to it, or your body gets used to it, or you adapt. I do remember that the side effects were worse in the beginning, and maybe it has to do with just managing it better now.
I can tell you that acalabrutinib causes headaches for me personally. It just straight up causes headaches. They resolve from caffeine; if you get a headache and drink a coffee or take an Excedrin that has caffeine in it, it’s pretty quick. It goes away.
Dr. Ron, who’s been at Phase 2 clinical trial, it was her tip on that, and it worked. If I ever got a headache, sometimes I’d wake up in the morning and just be like, “Oh, my head is killing me.” One cup of coffee, and it would start to fizzle out.
Luckily, I like coffee. I drink black coffee every morning. If I didn’t drink coffee and had to take Excedrin every day, I might feel differently about that.
How long would the coffee last in terms of helping?
I was a 3-cups-of-coffee drinker every morning to begin with before all of this. The headache is every day, but it subsides every single day from caffeine. Normally, if I wake up in the morning with the headache and drink, it goes away.
I normally don’t get a headache, maybe not get one for the rest of the day. If I get one in the afternoon or evening, I can pop an Excedrin; it’s not every day that you get a second round of headaches. It seems like waking up with a headache, as was my experience.
Any other side effects that were really tough?
It’s hard to tell which ones are doing which ones, so these are just my opinions.
I really think Excalibur is causing the headaches. Then with lenalidomide, I feel like it causes a ton of fatigue.
The pills are causing all my fatigue. That’s my number 1 side effect. That’s my biggest problem. It’s like tired, but fatigued isn’t tired, and I want to say weak, and fatigue isn’t weak. It’s like putting those 2 in a blender, and it’s something else let a little light that hits me pretty hard.
If I go to work and I’m moderately active throughout the day, I’ll come home, and that’s it for the day. I’ll be on YouTube in bed for the rest of the evening.
Fatigue is the biggest side effect of lenalidomide.
What does a normal day and fatigue look like?
Even when I was having symptoms with those hives, I was out to dinner. I was meeting friends.
I don’t do that anymore. If I do a workday, that’s it for me. I don’t have anything after work. There is nothing left for me to give.
I had a doctor’s appointment at 2 o’clock yesterday, and the thought of having to get up and go into Manhattan and come back, the level of exhaustion is just like, “I don’t want to do that.”
For people who’ve never been on treatment or cancer or if you’ve ever been so tired where you don’t want to take public transportation, and you just pay for that car, that lift — that’s fatigue.
I can’t deal with getting on a train right now. I can’t deal with getting on a bus right now. I’m so lethargic. I’m paying for a Lyft or an Uber. Maybe that’s a New York City analogy, but that’s how I feel about a lot of things.
Like walking the dog. I just don’t want to do it. I used to play tennis. I used to go meet up with friends all the time after work. I don’t meet up with anybody after work. I don’t play tennis anymore.
The amount of hours I have to dedicate to the day is a lot less. I’m not what I used to be during those hours.
What helped you through the fatigue?
I’m still working on it. I met with an integrative health doctor yesterday. We talked, and the soup of the day was fatigue.
This doctor is at Weill Cornell, a real doctor, a board-certified doctor. We were talking about solutions for it, and one of the things we talked about was potentially doing some weight training and some cardio, even though that sounds totally counterproductive and the exact opposite of what you would want to do if you’re so tired.
We talked about strengthening, building muscle mass and strengthening the heart to potentially alleviate the fatigue a little bit or improve my quality of life. It’s a long process. We talked about starting really small and building up to maybe 150 minutes a week combination, maybe like 5 days a week. Then maybe year 2, punching up to 300 minutes, but in very small increments.
That may be a solution. I’m going to try, but it’s not like, “Boom, that’s fixed.” It’s going to be a path and a journey. I have to do the work to have a little bit better quality of life hopefully. Because for me, my protocol is I’m going to keep doing this therapy for as long as it continues to manage my disease or until I can’t handle it anymore.
Investing in this idea may be worthwhile for me, considering I’m going to keep taking these medications.
What’s the follow-up procedure for monitoring MCL?
I’m incredibly fortunate because the clinical trial was trying to get FDA approval, and there are people that are analyzing data, and there’s research.
I received MRD tests regularly during the clinical trial for the formal 2 years. I got one before I even started and then at different intervals throughout the trial.
From what I understand, even though they aren’t FDA approved for mantle cell lymphoma, the researchers can identify if there are any cancer cells in my blood down to 1 in 2 million or something like that. From what I understand, it’s a very sophisticated science and test.
We know from my last test 3 months ago that there’s still a minimum amount of cancer cells in my blood. But if I wasn’t getting the MRD test and I was just getting R-CHOP or whatever and not on this clinical trial, they’ll just send me to get a PET scan, and they would tell me that I’m in remission. That’s what my doctor said.
She goes, “I can’t say that to you because I have this other test over here that tells me the truth, in a way.” She said, “Let’s call it metabolic remission.”
All of my lymph nodes are now the same. They’ve shrunk down to a size that fits into the normal zone. None of them are like lighting up like a Christmas tree as they used to. From a PET scan point of view, I look good. But from the MRD test, we know that it’s still present.
Again, they use the word “minute.” There’s a very small amount. At the second anniversary, which was last month, they pulled blood for another MRD test. I don’t have those results back because in a clinical trial, they do it in batches. I’m in a batch of a pod of people.
Those results get released once the whole pod completes and finishes. I’m hoping that when that result comes back, I don’t know if it can be better than minute, but I would love to hear complete remission, which would mean there’s nothing.
But again, my doctor says, “Don’t get hung up on the name of complete remission because there really isn’t a cure for mantle cell lymphoma.”
I believe there are some doctors who think they’ve cured some people, but they’ll say, “I don’t know,” until they get another 20 or 30 years down the road and die of something else.
I think it was in the 90s that it was even really discovered. For the first decade and a half, they didn’t even know what to do with it. They didn’t have treatments and therapies that were specific for mantle cell lymphoma. They were just giving what they were giving to another disease until they did their research.
It’s new in terms of medical error. It’s a newer cancer that they’re trying to understand and treat.
How is MRD different?
I go in every 28 days for standard blood work because all these pills drop my white blood cell count. Before they give me the next bottle, I have to be at a certain level, or no meds for you. When they do the research tubes, when they’re already taking my blood, there’ll be another pouch with 2 vials that are basically in a special bag. Then those two vials get sent to another specialty lab on them, and it goes to an outside lab outside of my hospital.
That is where the clinical trial is crunching the numbers or whatever they do.
Describe the clinical trial process
It was like a stack of papers this thick, and you’re supposed to sit there and read through the whole thing. It seems like a contract. If you die of a heart attack, you can’t sue us. There’s a lot of stuff like that — 8 pages of potential side effects. “If these happened, sorry, we’re not responsible.”
They outline a lot of the financial things, like your insurance is still going to be billed for Rituxan because that’s standard care. You’d be getting that anyway. It seems very legal.
No, there weren’t any issues in terms of my insurance with a clinical trial. The way the clinical trial was set up is like they knew what was standard care and what wasn’t.
They know MRD tests and standard care, so they’re footing the bill for that. They know rituximab is standard care, so they tell them, “Bill that through the insurance.”
Anything that was going to be provided for me anyways is getting billed through the insurance. Anything that is above and beyond is being paid for by the clinical trial.
Also, I had a lot of questions about what happens after: “Are you going to kick me to the curb?” I was told no. If this works for me and I complete the 2-year clinical trial, they will continue to give me the medications as long as it’s working for me and my doctor. We, together, decide that.
I finished the clinical trial formally 2 years, and my doctor and I decided together to keep going. The clinical trial has continued to give me these 2 medications, and they’re not billing it through my insurance.
They’re the same process as to how I was getting them before. Because they’re not FDA approved, they come from a specialty pharmacy, especially lenalidomide coming to a mantle cell patient. It comes from a research pharmacy.
They call me, and I have to answer a whole bunch of survey questions. Then I get transferred to somebody else, and I get all these yes and no questions because lenalidomide causes birth defects.
There’s like, “Have you had sex with a female who may become pregnant? Yes or no?” It’s a lot of surveys like that.
You will have to complete a survey every 28 days. They will say your next survey is available on this date. That’s kind of the process, and then you get a shipping confirmation from the pharmacy. They’ll say, “We’ve shipped your pills to your doctor. You will get them on your next visit.” That’s how one comes.
Then the other one, I think, just comes from the pharmacy internally. But it’s grants from the clinical team for these pills to get there. They’re continuing to pay for them for me to continue on, which I appreciate, but they’re also going to be getting more data and more information.
I think they’re just as excited that I’m continuing as I am as excited to continue, which is great. This is the ultimate perfect match, right? It’s working for you, and it’s also information for them that will hopefully help future patients down the road.
They call me. The doctor calls in the prescriptions, the specialty pharmacy, and then calls me. They do a security check to ensure it’s me. They ask a whole bunch of standard questions. They say, “OK, great, we’re going to ship.”
You need to complete your monthly survey, and then I get transferred somewhere else and have to do yes/no questions. Have you donated blood? Have you donated sperm? All of these. I believe it’s because of something to do with the FDA.
I take the survey, and then I show up at the hospital. They take my blood. They send it to a lab right down the hall, and I sit there for about 45 minutes waiting for the results to come back. Then if the white blood cell count and the new drill fill or something like that is good, then they hand me the pills. But I don’t get to leave until I get the blood work back.
What happens when your counts are not good?
I’ve never not gotten my pills. They’ve always been like, “Your counts are good.” I haven’t had that bad news yet, which I feel really fortunate about. My white blood cell count just sits out of 3 like right across the board, like a piece of paper. It’s low, but it’s still right at the bottom of the acceptable mark, but it just stays there.
I don’t know anybody else, any other clinical trials, or any other place where mantle cell patients are receiving lenalidomide, at least not in the U.S. I don’t know. I think this clinical trial is the first to combine lenalidomide and acalabrutinib.
Those of us in the clinical trial are like the guinea pigs for that combination for mantle cell lymphoma. What happens to us is kind of what they’re looking for. Hopefully, nothing bad. I’ve been here for 2 years doing it, and I’m still here.
What’s your response compared to the typical response on the traditional route?
I’ve never asked, “How do I compare to that?” She’s never brought it up to me, but she’s been very excited about the response in general. Like everybody seeing a response, we have people in complete remission on the clinical trial.
“I’m very excited that you responded, and at the level that you responded, I think we should be happy.” She seems to be thrilled with just in general, how everybody’s doing.
I think everybody got a response. There wasn’t one person that it just didn’t work for. I think that there’s some excitement around that. For me, I’m glad I didn’t do the R-CHOP, and I don’t know what’s next for me.
It’s one of these games of chess with mantle cell lymphoma. I’m going to keep doing this for as long as I can do it and manage the disease. Then, we probably all assume at some point this is going to relapse and come back, and then I’ll need to try another therapy.
I think, if that’s the case, I will hold out to do a traditional type of chemotherapy that would be like going into a stem cell transplant or CAR T-cell therapy or something like that.
It’s one of these games of chess with mantle cell lymphoma. I’m going to keep doing this for as long as I can do it and manage the disease.
But to do straight-up R-CHOP or chemo as a treatment is not appealing to me unless we’re going for a home run on this.
We’re going for the stem cell transplant. We’re going to do CAR T-cell therapy.
I’m in a lot of cancer support groups. There’s anxiety between the chemotherapy and going off and scanning again in 3 months and seeing every 6 months. That sounds anxiety-driven.
I love the fact that I go to see the doctor every 28 days and this treatment continues. I feel like I’m doing something by taking the pills every day. When you talk about managing the disease, I feel like a management thing is happening here. If I just did R-CHOP, we feel like, “Let’s whack it. Now you go over here, and we’ll see how long that lasts.”
This process feels a little bit more like we’re staying on top of it.
Long-term care and attention
I know most lymphoma patients are getting PET-CTs, if they’re lucky, every 3 or 6 months. I’ve been getting MRD tests every 3 months. They’re giving me another one in 4 months. Then they said, “If you stay after that, every 6 months,” so twice a year for free for being in a clinical trial. I’m going to have information that they shouldn’t be getting.
MRDs aren’t approved for mantle cell lymphoma, but there’s no insurance company in the world that’s going to just start doling out MRD tests for mantle cell patients.
This feels like I’m really being watched and managed at a level way beyond what is even futuristic. It’s beyond what is even possible if I wasn’t in a clinical trial.
What do you have to do every day?
I can show you one. I have one right here. It basically just says study drug diary. You have to log the date, time and the number of pills you take every single day.
I’m taking acalabrutinib every morning and every night, and then I’m taking lenalidomide, 3 pills every day. Then I take it for 21 days and then 7 days off. Even the diary will remind me, “Do not take on those days.”
It’s very important that I bring all the pill bottles back. They have a freak-out if you don’t. They’ll have to write a report if you lost the bottle or something. In one instance, they know that my cycle is 28 days, so I should have 4 pills left or something like that. They’re opening it up, making sure that there are 4 pills in there that I bring back.
If it isn’t there, they’ll ask, “Where are they? Did you miss any doses?” Randomly, every other time or every 3 months, they’ll give me a whole bunch of questionnaires.
The questions are like on a scale from 1 to 5 — do you feel close to your family, etc. Then you meet with a clinical trial nurse every time, and you report every single symptom that happened during the 28 days and make notes next to the date, like, “I had diarrhea on that day. I had a really bad headache. I had chemo brain on that day or whatever.” Whatever side effect you had.
Every 28 days, you turn over all the side effects of what you did. That’s pretty much it for paperwork. It’s the drug diary.
I thought there were 28 people all starting at the same time, and I thought that I got into the second-to-the-last spot, but it turned out I got the second-to-last spot of Pod 2. I guess when I started 2 years ago, they only started 12 people for the first year.
We were like the guinea pigs, and then after about 11 months, they started more pods. But the goal is 28 people roughly for this clinical trial.
I believe there is now a waiting list. It’s sort of caught attention, and there are people that want to join. I’ve heard that there’s even a hospital in Florida that is asking to potentially start offering the clinical trial at their hospital and then enrolling more people.
I think eventually, as it goes down the road, maybe they’ll enroll even more people in Phase 3, like 100 or 200 people across the country. But right now, it’s just at Cornell in New York City.
VIDEO: Life After Cancer (Quality of Life)
For more than 2 years now, Jason diligently writes in his clinical trial journal every single day. Staying on his course of treatment outside of the formal trial gives him hope of full remission from mantle cell lymphoma.
Jason’s story is also an inspiring example of patient self-advocacy — making informed decisions for a better quality of life.
What has been the impact to your life?
I’m really grateful that I have this option. It’s been 2 years, and it feels like it was the right decision for me. Maybe it was not a good idea to make decisions based on those emotions, but it turned out this was the best choice for me. Those were things I probably should have worked through with a therapist, or whatever, those feelings and emotions about cancer treatment.
Regardless, I can look back now and say I still made the right choice. This was the right choice for me. I was the type of person before, like I said, when I went to that PET scan, that was the first time I got an IV. I didn’t really like needles. I was like the person who’s closing their eyes when you get a flu shot.
I’m such a different person now. I can literally watch them put an IV in now.
I’m really grateful that I have this option. It’s been 2 years, and it feels like it was the right decision for me. Maybe it was not a good idea to make decisions based on those emotions, but it turned out this was the best choice for me.
I’ve had so many IVs. I’ve given so much blood, even to the point where I shock myself. I will volunteer to give my blood for things, and I’m the type of person before who would be scared to get a flu shot.
I’ve surprised myself with my self-evolution with all of this stuff. I really didn’t like doctors and going to the hospitals. I just had a lot of bad memories. I’ve been to an infusion center with my mom in the 90s. I’ve shocked myself with what I was willing to do.
When I get Rituxan infusions, I feel really good about it. Even though I’m in an infusion center, I’m like, “This is a good drug; this is helping me.” So I feel really good about that.
I’ve surprised myself with my self-evolution with all of this stuff. I really didn’t like doctors and going to the hospitals. I just had a lot of bad memories.
Dealing with the logistics of follow-up treatment
There’s pros and cons in both.
For the first 4 weeks, I was there every week, and then I went back every 28 days for the blood work, to meet with the clinical trial nurse, to get the medication and then every other business.
With the clinical trial, it’s very rigid. I know my schedule a year out. I know every 28 days on a Wednesday, I have to be there.
During the clinical trial, you can’t really say, “Oh, I’m going to Hawaii. Can we push this a week?” It’s normally a no. There’s a little bit of grace, like 1 or 2 days, maybe here and there and make a special exception. But then it changes the whole schedule. If you change 2 days, then your whole year changes. It’s that serious.
There’s pros and cons, I guess, to everything. I see what you were saying, but with a clinical trial, there’s just a lot of accountability and many appointments. It’s not like I go to Walgreens and get these pills. They’re just not approved for the frontline treatment. I have to pass all these tests to get them. I have to fill out paperwork, turn in diaries.
There’s pros and cons, I guess, to everything. I see what you were saying, but with a clinical trial, there’s just a lot of accountability and many appointments.
Do you have any guidance for MCL patients?
I wish I did have good guidance, because I’m in support groups.
In support groups, I’ve heard horror stories, especially of Phase 1 clinical trials. I feel very fortunate and grateful, and maybe I got some dumb luck, hopefully, getting into this clinical trial because it seems to be working. It seems I can only speak to mantle cell lymphoma because that’s what I have, and that’s what I’ve been researching, and that’s what I’m doing.
Mantle cell lymphoma is a newer cancer, historically speaking, and they’re just in the past 10 years starting to create individual therapies designed just for mantle cell. It doesn’t really get a lot of attention because it is the rarest of all the B-cell cancers. It’s the least amount of diagnoses per year when you’re talking non-Hodgkin’s B-cell lymphoma.
I think clinical trials may be worthwhile looking at if you have mantle cell, because that’s where a lot of new stuff is happening. For a long time, you were just getting a lot of the old stuff or repurposed stuff. It almost felt like you were like the youngest child and getting all the used [stuff] — just give them what we gave all the other B-cell cancers.
I think it might be worthwhile if you have mantle cell lymphoma and you’re looking around and trying to figure out your options. Right now, if I was diagnosed, I’d be seeing if I could get into a CAR T-cell therapy clinical trial for mantle cell.
I listen to a lot of cancer care calls and listen to a lot of doctors talk about the stuff that’s happening with that. It just seems like there’s a lot of new modern therapies that are actually being created or tested and designed for mantle cell. They’re not FDA approved.
The only way you’re going to get a shot at getting them is a clinical trial. Do your research, do your due diligence, and follow your intuition.
I feel like I got really lucky. That helped. I showed up at the right place at the right time. That’s just luck, like I go to Las Vegas and I hit the button on the slot machine. That’s just luck, but luck happens. Then the rest of it is just doing research and following your intuition and making an informed decision.
Do your research, do your due diligence, and follow your intuition.
Guidance on PET scans and insurance
I ask a lot of questions, and I’ve learned a lot. I feel like the health care team around me tells me the truth.
I’ve learned that lymphoma patients are not getting an MRD test like I am. You should be getting PET-CTs for lymphoma patients. If anybody doesn’t say it’s a PET-CT, I think that they’re lying because I’ve asked everybody.
If you have lymphoma, PET-CT is really what we want, but insurance companies don’t pay for those for everybody. I’ve heard Medicare gives you 3 or entire life period, full stop. A lot of the rules are designed around cancer patients having one PET-CT per year.
Still, it’s just like this across the board. It would be really great if we could get some advocacy, maybe from LSS or somebody to really advocate for lymphoma patients in particular, that they should be entitled to PET-CT scans.
It may not be as important if you have breast cancer, as my mom had, or some other type of cancer, but it is for cancer that affects the lymphatic system and the lymph nodes. It shouldn’t be a fight for lymphoma patients to get the appropriate tests, which is a PET-CT.
I understand why the insurance companies do it, but I think there should be some advocacy just for that particular thing, which is something that I learned on this journey that lymphoma patients should get PET-CTs.
Advocating for yourself
I made a mistake with my insurance company when I left. My primary care was at Weill Cornell. And when I was looking for the specialist, I went into my insurance book and found somebody who took my insurance that was in the area. That was a mistake because I didn’t ask the right questions.
I learned later that she wasn’t board certified, and I learned how important that is. I learned that all the Weill Cornell doctors have to be board certified or lose their job. That’s great. When I leave there, I’m always asking now, “Are you board certified? Are you up to date?”
The last time they were board certified in oncology was 1997. That’s what you’re getting. I really think I had a bad experience there because I picked a doctor who didn’t continue education and wasn’t board certified. I don’t think she liked me much either.
The other day, I think she thought I was a little bit mental because I ask a lot of questions, which some doctors don’t like. She went as far as to try and prescribe me mental health medication during the diagnosis period because she thought I had anxiety that wasn’t in line with reality.
Then 4 or 5 weeks later, I was diagnosed with cancer. She was way wrong. She did call me on the phone when she heard. I give her credit for calling, but the message that she delivered was a little bit defensive. I think she felt bad that she was so way off, but I think she was way off because she just wasn’t a good doctor. I don’t think she was a good doctor for trying to push me into mental health medications and be dismissive of my symptoms.
Message to others going through cancer
I doubt there’s a mantle cell support group. There are like 2,000 cases a year. I’d be shocked to see that.
The closest I found is blood cancer support groups in general, but big shout out to support groups. It’s really great because here’s the reality. In the beginning, with a blood cancer like mine, at a minimum it’s going to be like 5 years.
If I did nothing, I’d probably die in 5 years. Chances are I’m going to have to do multiple therapies. It’s going to be an ongoing process. It’s going to get dragged out for probably, let’s say, a decade, hopefully way more. That’s a long time of your friends and family not wanting to hear about what you’re going through.
My friends and family were kind of concerned for the first 4 months or whatever, and they would check in or whatever. Right around the 6-month mark, everybody’s like, “OK. He’s not dying tomorrow or next week or next month.” The support groups are great places where you can hold, just be there and listen to other people, and also you can be heard yourself.
My family or my friends never had a bone marrow biopsy. They’ve never had a PET-CT. You’re talking to the wrong people, so support groups are a great outlet — and especially if you have blood cancer, typically the journey’s longer.
If you find a regular group that meets every single Monday or whatever it’s going to be, it’s like you are seeing the same people over and over again. I think that’s something great about support groups.
The one that I started in person pre-COVID (and now it’s on Zoom), it’s the same people that have been there, for the most part, for 2.5 years now. You kind of see people go up and down, and that’s also helpful to you.
You can also bounce things off other people. We talk a lot about doctors and second opinions and managing. We were just talking about that other doctor.
I’ve seen people in my support group dump their oncologists and pick another one just because they’re in the support group talking about it and everybody saying, “I can’t believe they talk to you that way. You need to get rid of that person.” It’s like you go to school. Not all teachers are the same, and not all doctors are the same. There’s like 6.5 billion, 7 billion people in the world, and we’re not all going to get along.
Sometimes a support group will help you figure out where you need to be or where you need to go and get you information.
The other thing I do is yoga. I do gentle yoga once or twice a week. I used to do pilates before that. It’s not serious activity. I’m not running or doing all this cardio, but it’s a nice reset outlet if you can find access to it.
Just have 1 or 2 things a week that you can do, and it doesn’t even have to be yoga. It can just be like a massage. If you can come up with a couple of things that you like to do each week and have that on your calendar.
I always try to have something fun to do to look forward to, whether it’s a weekend getaway or planning something with a friend. I feel like my work really has given me purpose and reason to live.
Prior to starting a company, I was a freelancer working for other people, representing other companies. Now, luckily, I have my own business, and I’m an entrepreneur having a passion for something. For me, it’s my business; for you, it could be anything.
Having that passion for my business and my company really gives me a reason to live. It’s like there are employees there. We have wonderful customers. We’re building something. We’re growing something. Having something to do that you’re passionate about is ultimately the most important.
1st Symptoms: Lump on left-side of neck that grew bigger over a couple years, new lump on right side Treatment: 6 cycles Nordic chemo protocol, alternating cycles of R-CHOP and rituximab + high-dose cytarabine, autologous stem cell transplant
Richard’s Stage 4 Relapsed DLBCL Non-Hodgkin’s Lymphoma Story
Richard shares his stage 4 diffuse large B-cell lymphoma (DLBCL) story and having to undergo treatment 2 different times after his cancer relapsed 5 years later.
After finding a new medical team, Richard decided to participate in a clinical trial testing venetoclax and selinexor to treat DLBCL.
Explore his story below to hear all about his experience with chemotherapy vs. the clinical trial, dealing with side effects and the support he needed to get through it all. Thank you for sharing your story, Richard!
Thanks to Karyopharm for its educational funding support of our program. The Patient Story retains full editorial control over all of published content.
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
1st Diagnosis & Treatment
Tell us about yourself
It’s great to be part of this. I love to tell people what’s happening and how things are going with my clinical study and just life in general, and just get another friend out there.
I moved here from Chicago 42 years ago, and so I think I’m going to stay. I’m married. We have 2 children. They’re adults now. Elizabeth’s my business partner, and we have a tamale company.
Richie, my son, is into real estate. In fact, last year, he was cited the best property landlord for the homeless. He helps people transitioning back into society from wherever. He and his friends buy apartment buildings, and they cut them in half to make them dorm-room size and fill them up.
My wife just left the design business that she was in for years. I say she was set free! Now, she works with my daughter in the bodega we opened for the tamale company.
We had a catering kitchen, and catering dropped off the map. We had to do something. We opened up a bodega, which is like a corner store.
Describe how you processed the cancer diagnosis
I was like, ‘Okay. How did I get it? Where did it come from? How do I get rid of it?’
Those were the 3 things that entered my mind.
I thought, “I want to go to the MIT of cancer research.” I found out that that would be MD Anderson. That’s only 4 hours from here, from Dallas.
I would go down. I called them that day. “I need an appointment. I’ve got this and this.” They said, “Okay. Have all your records sent down here.” I sent my records down there. In 2 days, I had an appointment.
That’s where we did the R-CHOP chemotherapy. After one round, there was no evidence of disease, no evidence of cancer. I thought, “That sounds good. The chemo knocked it out. Let’s go! I’m done.”
They said, “No. You’re going to have to do 5 or 6 more [cycles].” So I did. At the beginning, I was really health-conscious in my diet and exercising and trying to stay fit, but I really had to step it up now that I had a culprit in my body. It wanted residence.
What were the R-CHOP side effects?
It was hair loss and appetite loss. ‘It’s just lose, lose, lose all the way around me,’ I thought. That’s why I needed to get out of the chemotherapy. I wanted to stop.
My going total plant-based diet was a big aid to that. Total plant-based was just something else to get excited about. What can I do? What kind of mushrooms beat cancer?
No sugar. That was the first thing that went. No sugar, then dairy, then just total plant-based, and I was liking it. The new menus were interesting. It was exciting.
5 years later, it came back, and I knew right away what it was. The tumor came back.
I call it the ‘culprit’ because I don’t like to name it what it is. Because it’s not going to stick around.
Because the tumor came back, I had edema in my leg. I tried to self-treat for 7 or 8 months. I just upped the vegan thing and tried to do more exercise and massage and sound baths. I would do Reiki.
What made you seek cancer treatment?
My friend lives in Houston, but I’ll go down there and ride bikes. He just looked at my leg and said, “Oh, man, whatever you’re doing is not working fast enough. You need to have that looked at.”
I made the appointment to see Dr. [Farrukh] Awan. He just said, “Okay, you can continue what you’re doing, fine with me, or you can do this, or you can do this.” Then he said, “You know, there’s a non-chemo test I’d like you to take.”
I said that we have a tamale company. It was in the beginning of the tamale season, where it just goes berserk, so I just said, “How about January?”
He goes, “Yes, you’ll still have [the cancer] in January, I’ll still be here, and we can still do the same thing.”
COVID-19 slightly shifted the path forward
Then COVID was at its peak. He just said, “No, we can’t start now. We’ve got half the staff, people are getting sick. It’s taking twice as long to see just one patient because of all the work you have to do sterilizing everything.” He just goes, “No, you can’t start.”
Then 2 days later, called me up, said, ‘Hey, we can do this. We can do this as outpatient.’
Describe the venetoclax-selinexor clinical trial
What was the regimen?
I started with the selinexor and venetoclax. Then it caused nausea. My doctor kind of punched me in the arm, said, “Don’t be a cowboy. Take the [anti-nausea] medicine.”
He’s right. I take it so you don’t have the symptoms, but you’d still have that feeling in your stomach.
What interested you about the venetoclax-selinexor trial over other options?
My doctor said, “You can take it and go to work. Come in, and we’ll watch you the first few times you take it, the first few weeks, because in the beginning it’s a step up [in terms of dosage].”
You increase the amount, the dosage of each drug itself. Then they want to watch you in the hospital to see for the first 3 days after you take selinexor.
That’s typically about 2.5 days for when I still take it because I only take that [drug] once every 7 days.
Describe the clinical trial regimen of venetoclax and selinexor
Every day I take venetoclax. That’s 7 tablets. They’re about the size of your average vitamin C tablet. It can be mistaken for that, about the same color tint.
7 of those, and I just take them all at once. I take a bunch of water, make sure I can open my throat and just take all of them down. Also, an hour before that, they gave you some medicines to prevent nausea. I take those, set my alarm, then take the venetoclax after that.
Then there are also other drugs you have 2 hours before you go to sleep to prevent nausea from when you wake up, but I usually don’t take that. I’m asleep, and it doesn’t bother me. I don’t notice it when I wake up. It hasn’t been that intense with me.
Every day, 7 pills. Overall, including the venetoclax, I take probably 13. Then the other pills are very small, for nausea. Another is something to help my lungs, keep me breathing better. They include:
venetoclax
prochlorperazine/Compazine
olanzapine
loperamide
ondansetron
acyclovir (“twice a day, one in the morning and one in the evening”)
allopurinol
selinexor (“a tiny blue pill that’s packed full of energy”)
How often do you take the selinexor?
Once every 7 days. I think it’s 80 milligrams, which I think is 4 tablets.
Describe the experience so far on the venetoclax and selinexor
I’m going into my fifth cycle, which will be my fifth month. The first 3 weeks, they admitted me to the hospital for 3 days.
I loved it. [UT Southwestern] was a great, great hospital. I had a view in Dallas overlooking Love Field. The 22-foot windows, ceiling to floor windows. It’s during COVID, so nobody could come see me, not even the nurses. They didn’t want to come into the room, only if they had to take blood. Then they’d come in and out.
I got lots of work done, made lots of phone calls. I read a lot and got to watch a lot of planes land in Love Field at night. It was great.
The second [hospitalization], they said, “Well, you’re doing so well. We don’t think you need to do it the third time.” When you go in, they say, “Because you’re on Medicare, if you think you’re being [discharged] too early, if you want more time, you can protest that and you can stay.”
I did that the second time. They said 2 days; I got to stay 3. It was great. Nobody was around. I’m inside my own little resort. My wife used to love to see me go, too. “Oh, sorry to see you go!”
They have a full menu. You can order all from 6:30 in the morning until 7 o’clock at night. You can order anything you want, all day long. It was great.
The third time, the third week, they say, “Oh, you’re doing so well. We don’t think you need to go into the hospital.” When they [mentioned] Medicare, I said, I’m switching it around. I think I should be admitted. I’m using my Medicare rules, so let me in!
I guess they thought I was funny, so they let me go in one more weekend. I was the poster child for the selinexor.
Describe any other side effects you dealt with
Well, it is pretty invigorating. In fact, I was never a night owl, but now I am. It’s like I don’t require that much sleep, although I do sleep very well.
TPS: You’ve had the opposite of fatigue. You had somehow a lot of energy.
That’s right. That’s the only place I know it’s coming from, is the tablets I’m taking. That’s what I think.
Describe the difference between the chemotherapy and this clinical trial
It’s like night and day. The R-CHOP is torture. It’s not the disease that’ll kill you; it’s the treatment. At MD Anderson, it’s just massive acres and acres of zombies walking around. That’s what I saw.
You got to talk to people because they’re everywhere. They’re on every transportation around the area coming in. You can’t avoid it. You can’t avoid not addressing it. It’s like, “Hey, what are you in for? How did you end up here today?”
People are more than eager to tell you, kind of waiting for somebody to ask them.
It was a day of travel and a day of chemo. You need a day to rest before you travel again. That was never any fun.
It didn’t get better for a week. Then it got better, and then I’d say, “Oh no, I’ve got to go back. Here we go again.” But I was getting better. It was necessary for me to do that. That was the only thing I knew at that time.
Chemo regimen’s impact on family
If you don’t have support at home, you’re out of it. If your kids don’t want to eat that way or they don’t want to try new things, you’re cooking for yourself.
That’s no fun. I know just how much support [patients] need to do something as simple as changing what you eat.
How are you monitored during the clinical trial?
Every other week, I have blood work. Once a month, I see the doctor. I’ve had two PET scans, not crazy about that because that’s just all sugar, but it gives a great picture.
How was the progress of the venetoclax-selinexor trial?
I saw pictures of the intruder, the culprit (the cancer). When I started in January, it was like spreading into my kidneys and my whole lymph system. I saw [the tumor] in January.
It’s like a little tiny pea-size today. It’s gone. I felt that yesterday when I was having my PET scan. It’s just flat, nothing there.
No picture, no anything. It turned out great.
How does it feel to see so much progress made during this clinical trial?
This works. It’s gone. This worked or is working. I need to stay on this.
Every day, there are new studies coming out. I’ll do this for a while, keep it at bay, and then soon something will come up and say, “Here’s a clinical study. Take this pill one time, and you’re good.”
That’s what’s on the horizon. When I was first introduced to CAR T in 2016, it was just like, “I’m getting out of here. No way, you’re not doing that to me.”
My wife and I asked the physician’s assistant, who was telling us all about CAR T. It was just like, “No way, you’re going to do that to me.”
Now it’s come a long way, too. The next thing is right around the corner.
How long will you be on the venetoclax-selinexor?
In fact, today my doctor said, “Forever,” because of the type of lymphoma I have, the diffuse large B-cell, unless I do the CAR T. As Dr. Awan said today, “Or you get the next thing that’s right around the corner.”
It’s rapidly happening all the time. More and more studies have been approved.
Managing your cancer like a chronic illness
I’ve just got to do it. Do what you’ve gotta do. What’s next? I don’t want to get all caught up in that. I just said, “Yes, that’s fine. I got it. I know how to do it. Let’s go on. What’s next?”
If you have trouble, think of it as you’re a boy scout. You’re working for your badge, and you’re going to get it because everybody else has got a badge, so you want that banner with all the badges on.
I did talk to a patient. I don’t remember their name or anything, but they said that we live better than the Vanderbilts ever did or any of those people, the wealthiest of the wealthy people.
We live so much better than they did, because they didn’t have the same medical institutions that we have now. If they got a cold, they could catch pneumonia and die. Running water and bathrooms and all that.
We live better than the Vanderbilts ever did and the Rothschilds put together. It’s only getting better. It’s like, “What will they think of next?”
I’ve got more wealth than the Vanderbilts.
What turned you off about the CAR T process back in 2016?
Because you’re in the hospital and completely annihilate your immune system. You’ll be there for about 2 weeks. The last place I want to be is a hospital when you have no immune system. That’s where sick people are. It seemed so harsh.
Then if they ever take your T cells out, send them to “college,” and then we put them back in, and there’s still a chance for all this stuff [to happen].
My wife and I asked the physician’s assistant. We said, “If this was your daughter, would you give her this treatment?” He couldn’t look at us, so we just said, “See you.” That was our answer.
Clinical Trials & New Research
How do you feel about participating in a clinical trial?
We could be trendsetters. You’re part of this. When you beat cancer, how would you feel?
Yes, put me on the poster. We’re part of it. If you don’t think you can change the world, you’re doing it.
Describe what it’s like being in a clinical trial
Every day they ask for the time you take the medication, the dosage and any comments. I have my list right here that I was reading before that I know what to take. Then there are my alarms on my phones. There’s a difference between being in a clinical study [and the chemo].
It’s not like going through chemo when you’re out of commission for 2.5 weeks because of what you did to yourself 2.5 weeks ago, submitting yourself to chemotherapy.
[This time] I got my life back. Whether I had to take pills, I never thought I wanted to be the person who has the daily pill things all the time, that I keep them hidden and keep them in a sequence order that I take the pills.
I move them to one side of the cabinet because there’s so many of them. Like I said, there’s 13 different ones. When I take them, I move it to the other side of the cabinet so I don’t forget. Then the next time I see them, I’ll move them across.
I have my list in there and take it because the clinical study, when you’re taking the dosage at home, they really want documentation. They want a back up. Not like, “Did he take these?” “Yes. I think so.”
What convinced you to participate in the clinical trial?
Dr. Awan was really encouraging. He was just like, “You’re great. I support what you’re doing, but after tamale season when [the cancer] is still here, I’ll be right here, and we can start whenever you decide.”
That was the complete opposite from MD Anderson, where when I went down there, they were like, “We’ll get you started now.”
The doctor-patient relationship was key in deciding where to go for care
He’s a great guy. In fact, everybody on the staff is really good. They just talk to you, not as a patient. They just talk to you and tell you what’s going on.
They say, ‘Okay, here’s what it is. Things are looking really good. Do you have any concerns or questions?’
They tell you what’s coming up. When they started to increase my dosage every week, it got more intense on the nausea. I don’t want to play up that so much.
It’s there, and I don’t want to talk about it, because it’s not something to emphasize. You know ahead of time it’s going to be there. You take the pills, boom. It’s good.
I’d love to talk to somebody, some other patients, because mainly I have not ventured into going on the internet and finding out all about it. Finding out all this stuff, it’s like, “No, that’s not for me. I’m just going to keep on doing what I’m doing, live my life, selling tamales and forgetting about it.”
Highlight the importance of the caregiver and the role that they play, these unsung heroes
I have a caretaker, Debbie, who takes care of me. I can count on her because I can go off in the other direction pretty quick.
We [patients] just got [the cancer], but they have to orchestrate the whole thing. They’re taking care of you. They’re making sure you stay alive, that you eat.
My wife can make some gorgeous meal. I’m just like, “Oh, wow.” Then I just take one bite and just say, “I can’t. I just can’t.” She says, “That’s great. That’s fine. Just put it away.”
She helps me keep up with my friends because I don’t talk a whole lot about it, about my illness to my friends or actually anybody. I let my wife talk about it. If you need to know, she knows. It’s like, “Oh, how old am I? Oh, yes.” She keeps track of all that.
Why is it so important to find new treatments that might lead to better quality of life?
Just being able to move and feel good and get about, not be sequestered somewhere, it’s freedom.
I was just real fortunate to have my whole family behind me and actually caring more than I did sometimes when they make you do something.
Somebody would always take me to Houston [for chemo], either my daughter or my wife. That was a 2.5 day deal. The 4-hour car rides are always the best conversations.
[It’s manageable] if you’ve got the support. I stay out of it most of the time. [My wife] tells me what’s on MyChart. Of course, I keep up on my medication. My phone or my alarm goes off, and my phone throughout the day for different reasons.
The promise of new research
I’d like to encourage somebody to keep on going, because it does get better. I have [diffuse large B-cell lymphoma]. It’s not going to go away, but like I said, the next thing is right down the line.
CAR T would wipe it out forever. There’s an over-the-counter CAR T coming out, more or less over-the-counter. It’s simplified, which makes it a lot easier.
I was talking to my physician’s assistant. I bring in a record of what I take, what time I take it, how much of it I take and any comments. I had everything all filled out.
He’s like, “Wow, this is amazing. You have everything documented.” I said, “I was told to keep it documented.” He goes, “Yes. Some people have taken so many other medications for different things, that they’ll say like, ‘Oh, I forgot to take it this week.'”
It’s like, “Wow.” It has to be built into the system, I would think, like the dosage. I could not just forget, like, “Oh, I forgot to take those.”
What’s your message to other patients about participating in clinical trials?
The first thing I asked was what’s the success rate, and they’d tell you, realistically. Then I want to hear all the benefits. I don’t want to hear all the fine print, all the side effects.
The one big thing that we talked about: upset stomach. There was this, along with the other side effects. There could be more of a possibility to be struck by lightning. Who knows all those side effects.
Just go into it thinking you’re going to be cured. The [positivity] helped me. I can see myself at the end of this. Even now, there’s no evidence [of disease], but I still have a ways to go.
It never really leaves you, the idea of [the cancer] coming back, but that’s okay. I’ll deal with that.
What has helped you get through prolonged cancer treatment?
Know that there’s a god. You’ve got to find out for yourself. What better time than when you’re close to what you might think is the end of your life or something? What a better time to connect?
Have you ever heard of Wim Hof? He’ll change your life. He’s also known as the Ice Man, and he does breathing treatments. He’ll climb the Himalayas in his gym shorts. He’s an amazing guy, and he does these breathing techniques. You do a round of those in the morning, and you’re charged.
Meditation is very important because I’m alone a lot. You better like being with yourself, especially during all the quarantine we went through.
You have to want to be an introvert. You spend a lot of time alone, a lot of guided meditation. There’s some great ones on the internet. I use them all. I don’t want to commercialize this thing and name somebody’s name.
Meditation is great. Stay active. Stay physically active. Walk. Walking also jogs the brain. If you walk with somebody, it makes the job move quick, too.
How important is it for people to share that and for other people to listen to the stories?
It’s cleansing. It’s part of the healing. I’m talking to you; I made it this far. I’m going to tell you what else is going on. You learn a lot about yourself.
Maybe you put some limits on yourself that then when you hear yourself say it, you’re like, “Whew, did I say that? I guess I am like that.” It brings change. Change where you have to.
There’s encouragement everywhere. I just want to pass that on.
Stephanie Chuang, founder of The Patient Story, celebrates five years of being cancer-free. She shares a very personal video diary with the top lessons she learned since the Non-Hodgkin lymphoma diagnosis.
Cancer details: Characteristics of both subtypes 1st Symptoms: Lower abdominal pain, blood in stool, loss of appetite Treatment: Chemotherapy (Part A: R-CHOP, HCVAD, Part B: Methotrexate, Rituxan, Cytarabine)
Bobby was diagnosed with stage 4 mantle cell lymphoma at 56 years old. Explore his story as he outlines going through a clinical trial to reach remission.
He also talks about breaking the news to his loved ones, taking health issues seriously and taking care of mental health.
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
I can’t tell you the blessings that I’ve received that I would not have received had I never been diagnosed with cancer.
I know that’s probably the weirdest, oddest thing that anybody would say, but from my shoes, I don’t think I would change anything in terms of what happened.
It has brought me and my family closer together, it has helped me from a faith perspective, and there are so many people I’ve met whom I would have never met.
Bobby J.
Video: Getting Diagnosed & Staging
Getting Diagnosed
Tell us about yourself outside of cancer
I played golf in high school and college. I ran just to keep my legs in shape. It was really odd that right before I got diagnosed, I wanted to run a race with my son in Colorado, and I’d gotten pretty bad out of shape. I fluke-ishly found this race in Colorado, and he agreed to go with me. This was about 2 years before my diagnosis.
I got in somewhat decent shape to run the race. I ran it again the following year. The year after that was when I was diagnosed. Part of that, physically — the doctor said the reason why it helped me get through my treatments was that I was in such good shape.
I was getting in shape for a race I wasn’t aware of.
What were your 1st symptoms?
The first symptom I had — and didn’t realize — was fatigue. I was running. I live in Louisiana; it gets very hot here.
My son and I were getting ready to go back to Colorado to climb, so I was running to get in shape for that. I noticed after I’d run about 5 miles, I got tired. Usually I could go about 6 miles without any trouble, and I noticed that at 5 miles, I started getting really tired.
Once that happened, the next thing was my wife noticed an enlarged lymph node on my neck. I also had one on the back of my neck.
When I went to the doctor’s, he said, “When you come back, we’ll start dealing with it from there.” Fatigue really was probably the first sign. I would not have known that.
Describe the ultrasound tests
The next thing — after the antibiotics I took for 2 weeks that didn’t work — was I had 2 ultrasounds done. One was on the lymph nodes on my neck. I had another small lymph node on my ribcage. It was almost like a calcium deposit.
They did the ultrasound on my neck. Then they did one on my ribcage. Both of those tests came back inconclusive.
What happened at the ENT visit?
My general physician suggested after the colonoscopy that I go to the ENT since the colonoscopy did not show any cancer. We made an appointment with the ENT.
Of all the things I’ve been through, probably the most invasive thing I felt was when he had to check my throat and went through my nose.
I feel so bad for people who have to take the swabs for COVID because I know how uncomfortable it is. It didn’t hurt. It’s just strange.
The ENT looked and really couldn’t tell anything. The only thing he felt like he could do to make sure was to biopsy and remove one of the lymph nodes.
Describe the excisional biopsy
I went in, and the anesthesiologist came in. He said I’d be in his hands for the next hour, however long it’d take. I got drugged up pretty good! My memory was of speaking to the anesthesiologist. The doctor came in. My wife took some funny videos.
I was pretty drugged up. The next thing I know, I woke up, and they said they’d let me know the results in about 1 week. That was on a Wednesday. My next appointment was about a week later.
Had the doctors ever mentioned cancer being a possibility?
I don’t remember them ever mentioning cancer. It was that I could have cat scratch fever, I had a cat, because he used to scratch and bite.
Never to my knowledge did they say anything about cancer.
How did you learn the cancer diagnosis?
It was a very emotional day. I had an appointment for 3 o’clock. My wife and I went down. The doctor came in and said they’d just got the results back. He said I had mantle cell lymphoma.
He began to go through some of the items, like, “This used to be very bad. Now there’s a better survival rate.” I felt really bad for the doctor. I actually went back and saw him last year. I didn’t have an appointment, just went by his office and asked his nurse to see him. I said I didn’t know how he’s able to do this, giving people this kind of news.
It was a very emotional time. My wife, who was there with me, and I were only in for about 15 minutes.
How did you decide where to get treatment?
My doctor discussed some treatment options here locally. We opted not to stay here in town.
We had decided years ago that if anything like this ever happened, we would seek medical attention at MD Anderson in Houston. It’s close enough for us, and the reputation there is wonderful.
I remember I went back to work. I did not want to call my employees and let them know this is what happened. When we got back to the parking lot and we got my children on the phone, I couldn’t tell them. My wife had to.
We just got them both on the phone. Neither of them lived here. Next, we had to go to my office. I pulled my employees together, and I couldn’t tell them either. My wife had to tell them as well.
It was pretty devastating from that perspective. I’ve heard other people who’ve been diagnosed. Never would have dreamed that it would be me one day.
There were a couple of days it was very emotional because the one thing that I struggled with more than anything was they didn’t know how bad it was.
They just knew that I had mantle cell lymphoma. It was bad enough being told, but not knowing what stage I was made it worse. They didn’t know.
It’s important to delegate responsibilities to others if you can
One of the things my wife and I agreed on, or I insisted on, was that I didn’t need to think about anything other than getting well. I said I needed her to be in charge of appointments, telling me where I was supposed to be and when.
I’ve always been a very loyal worker. I put in the hours. I do what I’m supposed to do. During this time, I told my wife that whenever, whatever, this cancer was priority 1, and everything else would go to the backburner.
My wife took over that role and would let me know where I’d have to be and when. She kept everything organized and moving forward.
My veins are not great. I don’t drink enough water, so needles are not really nice to me. I have not had a lot of success with the CT scan, although I just got back from Houston last week for my check-up. It was all clear, and I only got stuck one time for my CT scan, which was unusual.
That one I dreaded the most. I really dreaded going down there — not worried about the check-up but for the stick for the contrast dye. I really didn’t like that one too much.
Describe the colonoscopy/endoscopy
The colonoscopy prep, for anyone who’s ever had one, there’s no fun there, especially when you’re not at home. The actual test itself was really not difficult. They put you to sleep, and you cruise through it.
Describe the PET scan
The PET scan was similar, but you have to be patient with it. They inject you with “nuclear sugar” — that’s my layman’s term for it. You have to wait about an hour before they actually put you in the tube. There’s nothing constricting, so it’s open-ended.
There really weren’t bad issues, other than the fact that I had to hold my arms up over my head during the test. For somebody who’s not really limber, 15 minutes in one spot is not really fun.
Describe the bone marrow biopsy
There was a local shot [of anesthesia], similar to the colonoscopy, so I really didn’t feel anything. I didn’t feel the incision and the actual biopsy itself.
I was pretty knocked out. I didn’t know other than I lay down, and the next thing I knew, I was in a wheelchair. It was not bad.
How long did it take to get the staging results?
I had all the tests done over about a week’s time. Their terminology for the stage 4 cancer for me was above and below the diaphragm, and the bone marrow was also involved.
Treatment Decisions
How did your doctor describe the “watch and wait” method?
My doctor said the mantle cell lymphoma was very slow-growing (indolent). One of the things I learned, or my interpretation of it, was that whatever they give you, any time frame of “how many years you have left,” it’s after you go in remission.
For me, I thought if I could not have any treatment, the longer I could hold the treatments off, the timeline for remission wouldn’t start. Even though the cancer was there and diagnosed stage 4, the doctor seemed to think that it could be years before they would treat me.
When he explained that to me, I thought that was cool with me because as long as my timeline didn’t start until after treatment and remission, it’s years I’d be adding onto my life.
He did a great job of explaining that. I had no issues with the watch and wait method and delaying actual treatment.
You ended up starting treatment soon after
Later, H. pylori (bacteria) was discovered in my stomach from the endoscopy, which caused an ulcer. My oncologist determined the ulcer was caused by the cancer and decided to start treatments.
The local doctor did not discover cancer in the colon from the colonoscopy because no polyps were discovered, and most colonoscopies do not biopsy the colon during this procedure. Cancer was found in the colon from the test in Houston because they did a biopsy.
This was the only time that my doctors actually disagreed.
The gentleman who did the endoscopy felt the ulcer was caused by the H. pylori. That was good because I didn’t have to start treatments.
But my main oncologist was the one who decided he thought the cancer caused the ulcer, so they’d go ahead with treatment. In his mind, we’d just wipe the cancer out. We started the treatments shortly after that.
Message about getting a second opinion and self advocacy
I think it’s very much about people being at peace with their decisions.
Like it or not, you’re dealing with life-and-death decisions. I’m not saying that had I gone somewhere else my outcome would have been different. It could’ve been the same.
I do know that we were very much at peace about making the call to go to MD Anderson. My doctor wrote the protocol for my treatment. To me, it’s different if you go someplace like that compared to a doctor maybe in a smaller city who doesn’t see mantle cell lymphoma patients. They may open a book and say this is what the book says your treatment is.
We also considered another place. I have a friend who lives in Baltimore, so we considered Johns Hopkins and maybe the Mayo Clinic, but that was a bit of a stretch for us. My wife and I were very much at peace going to MD Anderson, and it’s just a first-class place.
It was another emotional time. I’d actually signed up for this marathon the year before. I ran it in 2015, and it was in Nashville. My daughter lives about 20 miles away from there.
After I got diagnosed, the doctor actually told me he didn’t want me to run. My point for my oncologist, when he finally acquiesced, was that I wasn’t running it for my own self-satisfaction or gratification.
I was running to show that you can be sick and still run. You can be sick and still be active.
He finally relented. My daughter said since my oncologist didn’t want me to overdo it, she’d run with me. She doesn’t run at all.
It was probably a bigger achievement for her than it was for me because she finished. It took me about 30 minutes longer the year she ran it with me than the year before. I kept telling her she just slowed me down.
It was a great experience to do that, knowing that of all the things we were getting ready to be in front of.
My point was, ‘Hey, we’re going to do this, and we’re going to show this cancer who’s in charge here.’
Video: Bobby on Treatment and Side Effects (Clinical Trial)
Treatment and Side Effects
What was your treatment regimen (clinical trial)?
Summary: Ibrutinib (oral pills, 4 a day for 6+ months) + rituximab (infusions, weekly for 4 weeks, then monthly) + Consolidated Chemo (4 cycles of hyper-CVAD, 1 week in hospital, 3 weeks off)
The protocol for the first part of treatment was the ibrutinib pills. I took 4 of those every day. It is a blood thinner. Then I took the rituximab. I had my first infusion on a Monday. I had them 4 consecutive Mondays.
Issue with low heart rate
Because I started running, my heart rate had gotten fairly low. It was averaging somewhere between 47 to 48 beats per minute, which was a side effect from the running.
The protocol for the treatment was that if your heart rate was in the 40s, you couldn’t take it.
Since I’d get those results from exercise, the doctor felt it wasn’t going to be an issue. But everytime we would visit the doctor, they would have to call him before the treatment started because they would not mix it until he gave me approval with my heart rate under 50.
That was a little bit of a drag because usually we wouldn’t get there till 4 p.m. or 4:30 p.m. to take the treatment. It lasted anywhere between 4 and 6 hours. Then we’d have a 6-hour drive back home.
How did you pass the time for the rituximab infusions?
Fortunately, for me, they would inject Benadryl into the IV before they gave me the treatment, and it’d just knock me out. I’d go right to sleep. As soon as I took it, lights were out.
I actually slept for about 4 to 5 hours, which was about the length of time of the treatment. When the nurse came in to take the needle out, she goes, “You’re free to go home!” I was ready to go.
I drove myself, but my wife went with me every time. The first treatment I had, they gave me the rituximab really slowly because they didn’t know how I’d react to it.
After about 4 hours, I woke up and got a little restless, so I started walking the floor. When I came back, my wife was in my bed.
Then I had to sit in the chair the rest of the time. You move, you lose!
What were the ibrutinib and rituximab side effects?
The only side effect that I had didn’t happen until my July treatment. I broke out in a pretty serious rash that lasted for about 2 days, and then it went away and never came back after the other treatments.
I did not have any side effects from anything. It was strange that I did continue to run all summer, and I ran my fastest 10k, 5k. Times I’ve never run before!
All the time I was taking the pills and going through treatments, so basically, they did not affect me at all.
How did you learn there was no evidence of disease (NED)?
During 2016, I had 4 colonoscopies because even though my colonoscopy in December 2015 was clear, it was clear because they were polyps. When I had my colonoscopy done in Houston, they took biopsies, and the cancer was prevalent in my colon.
Unfortunately for me, because of the prep you have to go through for the colonoscopies, it was the last place that the cancer showed up. I had a colonoscopy in November 2016, and it was clear. It had already been clear everywhere else, so the colon was the last place where they found the cancer. It was now gone.
The doctor then said it was time to go to the next stage of the clinical trial, so I went from Phase 1 to Phase 2.
Describe getting the port placed
I had 2 options: the PICC line or the port. I didn’t want the PICC line. We’d visited a gentleman who had a PICC line during his third treatment.
Having to go through all the maintenance of keeping it flushed, and it was always there, even if you could tape it and put it under your shirt… I decided I didn’t want any part of that.
We opted for the port. For the procedure, they put me to sleep, although I do believe I woke up during the procedure. I didn’t feel anything, but because it was on December 1st, the doctor was singing Christmas carols.
I asked one of the nurses, and she said, “Yes, he was singing carols.” I was sort of coming out of it as he was finishing up, but there was not a lot to it.
You started the chemo (Phase 2) right after the port placement
They went ahead and accessed the port while I was there. I had it put in my left side because they said it would be better for me as a right-handed person.
I stayed in the hospital for a full week. I was taking the treatment the whole time, every day. They told me how many bags that I would get from each of the medications. It was a different drug each day.
Describe the prep before the Hyper CVAD chemo
The first day we went to the medical center and had the port placed, then we had to go to the actual hospital and wait there. We went to the room, and the nurse came in and explained what I was getting ready to take.
The nurse explained the medications they’d give me for nausea. They started the treatment. I’d taken my laptop with me. This was on a Friday, and I was answering emails.
I was on the phone, probably more so to get my mind off it than I was trying to be a hero and say I was working through my treatments.
Friday, after close of business around 4 o’clock, they indicated to me that I needed to make sure to walk every day. They were going to give me a shot in my stomach to make sure the blood flow remained adequate.
My wife and I walked the first day about 3 miles all around the complex. The next day, we walked about 2 miles.
Sunday, we got up and went to the chapel. The alarm for my pump went off because one of my lines got kinked, so we returned to the room to get the alarm silenced.
It just hit me all at one time. It was like somebody flipped the switch. I went from being fairly active, walking around, to just basically being dead.
Self-motivation to move around as much as possible
On the hospital floor, for every time you lapped, you could stop at the nurse’s station, and they’d give you a sticker. I figured out how many stickers it would take to make a Christmas tree for my door, and I made all the laps I needed.
How many days did you get off between the 1-week cycles inpatient?
21 days. We would go September 1st, and the next time I went into the hospital was September 28th. Then it was a week in the hospital, and then 21 days at home.
I did have a small window where it didn’t have to be exactly 21 days. I think my last treatment I was outside that cycle by maybe a day or 2.
The anti-nausea cocktail caused depression
The worst side effect from the nausea medicines was it basically put me in a depression. I lay in bed, did not want to get up. There were 3 different medications they gave me. I’m not sure what the 3 were, but it caused me to go into depression.
I never understood why people ‘give up,’ why they don’t want to take any more treatments or want to check out. I understand that now.
Even though I’m not a depressed person, the medication said, “I really don’t care anymore.” I didn’t care to get up, I didn’t care to get out of bed, and I didn’t care to walk. I was just like, “Leave me alone.”
We have a friend who came in who wanted to come up and see me. I had to tell my wife that I didn’t want to see anybody. I asked her to tell them sorry. I didn’t talk to my children on the phone. Nothing. I was very depressed.
Also couldn’t drive after first nausea medication dose
After my first treatment was over, it was the only time I did not drive there. When we got in the car, I was still pretty much comatose from the nausea medicine. They had to pretty much carry me out. I got in the car, put the seat back and told my wife to take me home.
She didn’t know how to drive home because she had never driven home from there before. I had to get us out of the city, and from there I went to sleep.
By the time we got home, the medicine had actually started to wear off, and I was pretty much back to normal the next day.
You asked to stop taking the anti-nausea cocktail
They just called it a cocktail, and it was 3 different anti-nausea medicines. In Cycles 2, 3 and 4, I did not take the anti-nausea cocktail. I believe I took some Ativan.
The main thing is that I got physically sicker, but I took that sickness over the depression.
Only in the first cycle of the chemo treatments did I ever get to that point. The rest of the time, I just said, “Okay, I’ll get sick.”
I got sick, then slept, got sick, then slept. But for me, it was better. I was more active. I was walking more. Even though the treatments were supposedly hitting harder, it helped me not have to take the anti-nausea cocktail.
Even though it was supposed to help me, mentally it was something I didn’t want. I drove home after the last 3 treatments as well. That was a difference for me.
Any side effects from the hyper-CVAD chemo?
There were the normal things you get taking this type of chemotherapy, like losing your appetite. The whole time they were telling me to eat something, I was like, “What’s the point?” I would eat it and then get sick.
And the food was great! The first two days I was actually able to eat something, I got to order off of a menu that was different for patients. Starting Sunday into Monday and Tuesday, there was no appetite at all. I didn’t want anything. Food was the furthest thing on my mind.
I have a pretty full head of hair for being 61 years old. I was in the shower. The doctors said if my hair was going to fall out, it was going to take about 2 weeks from when I got home to start.
I was washing my hair every day, and nothing was changing. I was going along and thought since I had gone through Phase 1 with no issues, I would go through Phase 2 with no issues as well.
About the 14th day from when we got home, I was in the shower washing my hair. After rinsing it out, when I opened my eyes, I noticed there was quite a bit of hair in the tub. Not only was it there, it was everywhere.
Don’t mean to get too graphic, but it took me about 30 minutes to clean up the shower. After I thought I had beaten it, the fact that it happened, I was just disappointed.
I really wasn’t traumatized by it. I didn’t know what I was going to look like with no hair.
I asked the doctor when I was told I was in remission why I had to go through this maintenance ordeal with all the harsh chemotherapy. He said, “A cell is very small.”
He said he could not guarantee, even though the PET scan was clear and the colonoscopy was clear, that there was not a cell or 2 floating around.
He said the chemotherapy would take care of it, so I said okay.
Video: Bobby Being Part of a Clinical Trial
Being Part of a Clinical Trial
Describe the clinical trial
The combination of the rituximab and ibrutinib pills was the first phase. The trial I was in, there were about 150 people altogether. I got a chance to meet the first person to be in the trial. That treatment regimen was a clinical trial also because of the second phase.
My normal treatment for the hyper-CVAD chemotherapy would be 6 weeks. I only had to do 4.
How did you discover the clinical trial?
I’m leaning very much on my wife in this situation. She actually heard about the clinical trial before we went down to MD Anderson. She was very much an advocate for me to get in the trial.
We thought we were going to be on the outside because they had only taken so many patients. By the time we got there, they actually expanded the trial, so I was in the expansion part of the clinical trial. I think they had limited it to about 100 patients at first. I was like number 140 or so.
They added 50 more spots, so I barely got in. It was something we wanted to do. I felt very positive about it.
Describe your impression of your oncologist
When I got there, the doctor I got assigned to was Dr. Wang, who is a superb doctor.
The first day we ever met him, he walked in and said however long it would take for us to be there, we should ask any questions we have, and that he’d be there until we were ready to go.
Just a super human being. Orlando was my first nurse, and the physician’s assistant — they were a wonderful team.
What was the prep like getting into the clinical trial?
Because of the way the trial was set up, the ibrutinib tablets that I took during the trial were at no cost. The pharmaceutical company supplied those as part of the clinical trial.
We would have to go to the pharmacy there at the hospital to get the pills. We had to keep a log of when I took the pills, my temperature and some other things.
When we went back to the clinic, they would take the bottle of pills, count all the pills I had left, and make sure that everything was accounted for in terms of the number of days I took them and how many pills were left over.
You couldn’t take other medications during the trial
There was a part of the trial where I got a sinus infection during the trial part, which I’m very susceptible to getting. I could take no medication for that. If my fever got above 100 degrees, I would have to go to the hospital. It got to 99.9. Just barely got under the wire there.
I couldn’t take anything for the infection because any medications I took during the trial period may have affected it. There were some medicines I would normally take that I couldn’t take during the trial.
Everything was very regimented.
What would have happened if your fever had passed 100?
They would have just gone in and made me stay there if my temperature had gone above 100. It would have been something they would have just watched.
It wasn’t life-threatening or anything like that. I just couldn’t take anything for it, so it would have had to run its cycle without medication.
What made you and your wife so sure about the clinical trial?
Knowing I wouldn’t have to take as many rounds of chemotherapy, and the trial had a very good success rate. We were told that chemotherapy, in and of itself, may cause cancers later in life.
One of the reasons they wanted to back off the 6 treatments to 4 treatments was to make sure the side effects years from now wouldn’t lead to another cancer from the chemo.
We felt very strongly going the route of clinical trial was the way to go. The success rates of the people who’d already been in it were really high, so we felt very positive about it.
Describe meeting the first person to go through the clinical trial
We were there for a check-up, and he was there for his check-up. My wife had created a Facebook page just for mantle cell lymphoma patients at that hospital. He had joined that group.
Every time we’d ever go to the hospital, we’d let the group know we’d be down there in case they wanted to meet. Today with COVID-19, it’s more difficult.
He was in the waiting room to go in, and it was pretty unique to see the first guy in the trial. He had probably started the trial about 6 months before me.
He looked fine, and it’s always encouraging to see somebody who’s gone through the entire process. There was a gentleman who actually called me and wanted to talk to me about my experience. When I finished talking to him, he said that if I did it, he could do it.
It’s always encouraging to see somebody who’s gone through it. You can survive. It’s just a matter of knowing that it’s a brief part of your life.
If you had been Patient #1, would you have still done the clinical trial?
If I would have been the first patient, I would have done the same thing. Just the fact that you’re with people who are very smart, you just have to trust your doctors.
Was the monitoring any different in the trial?
I think only because we were going back so frequently. We had to go back every month to get the pills refilled. We did have a journal. Every day we had to write down pills were taken. We didn’t skip any pills.
Ibrutinib is a blood thinner, so I had to skip every time I had a colonoscopy. They would not be able to take the biopsy if I was on the ibrutinib, so I stopped taking the pills 3 to 4 days prior to the colonoscopy and 3 to 4 days after.
It was all part of the protocol, so it was built into the trial, and the medical teams always knew that. It scared me, because the pills are very expensive, that I would drop or lose one. We kept up with the pills and with the journal.
What did you have to include in the journal?
There was not really any feeling documented, but I wrote down any side effects I had.
Going through the trial, I think I was the only patient I know of who didn’t have to take any platelets (get blood transfusions), never missed work other than the treatment days when I was in the hospital, actually ran during the end of the second phase of the trial, able to exercise, and pretty much normal during the whole trial.
Donating your tissue and blood samples to research
Going through the trial as a patient, I allowed the hospital to take extra blood samples and extra tissue samples from me, anything they needed from me that was “extra.”
I felt like there were people who’d gone through this before me who did that, and because I was at a research hospital, the more they had, the better it would be.
Hopefully, whatever I left for them to do their research on will help somebody behind me now. I’d encourage anyone going through this, if they’re asked, to also allow that. You’re already stuck in a lot of cases, so what’s one more vial of blood?
What’s the follow-up?
After I finished the trial, my last day of treatment was March 3, 2017. We went back to see Dr. Wang at the end of March, just as a follow-up visit. The check-ups are seeing the doctor and a PET scan.
He would check me and say, ‘Enjoy your life!’
My first 2 years of remission, we went every 4 months, and then my second 2 years, every 6 months.
My last 6-month treatment will be in May of 2021. I’ve already been told that if I’m clear, I’ll start going once a year.
Did you have to deal with insurance for the clinical trial?
At the clinic and the hospital, there’s an advocate there for you, as well as a dietitian. When we first went, the advocate we spoke with about insurance knew everything and had things squared away. My insurance company was fabulous. I have no complaints with my insurance carrier (Blue Cross and Blue Shield of Louisiana).
Never had a hiccup. Never got any denials. They were just absolutely wonderful. I appreciate all that they did during that time. It was a load that was taken off of me.
Video: Bobby’s Reflections
Quality of Life Reflections
Taking health issues more seriously
Going on a trip to Yellowstone was something I wanted to do, so we decided to go there as a family vacation after Phase 1.
When my wife was looking at pictures, she noticed some slightly gray areas where the skin had gotten a bit discolored. She said it didn’t look right, and so we asked our doctor about it. He sent me to a dermatologist.
They did a small biopsy, a little scrape, and it came back as melanoma. It was stage zero. I look at it as somebody my age, where the skin is supposed to change anyway.
Had I not been at the hospital and gone through this process, I would have never have known it. I would have just said, ‘I’m just getting old, and that’s just a spot that old people get.’ I wouldn’t have gone to the dermatologist.
What support got you through cancer treatment?
My family. I had a brother who’d gone through radiation and chemotherapy a few years before I did. He would offer me advice.
People from our church who’d gone through cancer. My family was incredible in the support they gave me.
My work, I can’t thank them enough, including my superintendent (of schools), who called me and said whatever they needed to do, they’d be there for me.
The support not only at home but at work, where I spend every day it seems like, was just incredible. I’m so blessed with that.
My wonderful wife, who stood by me the whole time. Made me take my pills. Made me get to my appointments on time. An incredible woman. I’m so blessed to have her.
How did the diagnosis impact your relationship with your adult children?
They’ve always known Dad to be a pretty strong guy, and I got that from my dad. He was a World War II veteran. He told me not to give up. He told me to always keep trying in life.
My adult children were used to seeing Dad strong. They were there for me. My daughter lives outside of Nashville and my son’s in Brooklyn, but they always knew the right time to call.
They checked on me, how I was doing, told me they loved me, and reminded me to keep going. They were there for me.
I finished my treatment March 3rd, and we returned to the race where it all began. This time, all 3 of us — my son, daughter, and I — ran.
We had a great day. I spent time with them. I have 2 grandchildren from my daughter, and so we got to spend some time with them there.
The importance of taking care of mental health
I am very much faith-based. I have a very strong belief. That peace that I got during this whole experience was through my faith and my beliefs. That part is really what got me through it.
It’s all well and good to have this huge support group around you, but you still have to do the work. It’s you who has to get through it. I don’t know what I would have done had I not had that to lean on.
I’ve always told people this: I have a blessing and a curse. I have a curse because I got cancer. I had a cancer that’s supposedly incurable. I do believe that I have been cured. I don’t believe it’s ever going to come back.
How has cancer changed your life perspective?
I can’t tell you the blessings that I’ve received that I would not have received had I never been diagnosed with cancer. I know that’s probably the weirdest, oddest thing that anybody would say, but from my shoes, I don’t think I would change anything in terms of what happened.
It has brought me and my family closer together, it has helped me from a faith perspective, and there are so many people I’ve met whom I would have never met.
I don’t think I would change anything. I know that’s probably an odd thing to say.
There are plenty of bad memories, like lying in the hospital bed and losing my hair. I had people tell me that I didn’t look bad bald-headed, and I would look in the mirror and think I was a strange-looking person!
I figured out one day why I’d looked so strange. My eyebrows had fallen out. Even though my head has a good shape to it and I probably didn’t look weird bald-headed, the weird person staring back at me from the mirror with no eyebrows looked alien.
Now I’m back to normal. I just have to give God praises for letting me be here on the anniversary of my first day of chemotherapy.
1st Symptoms: Lump on left-side of neck that grew bigger over a couple years, new lump on right side Treatment: 6 cycles Nordic chemo protocol, alternating cycles of R-CHOP and rituximab + high-dose cytarabine, autologous stem cell transplant