Welcome to part 1 of Andrew and Esther’s story of chronic lymphocytic leukemia (CLL), myelofibrosis, and living life as a patient and caregiver.
In this segment, Andrew and Esther Schorr discuss their initial reactions to Andrew’s CLL diagnosis, figuring out next steps, talking to your children about cancer and what topics they will cover in this series.
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Esther shares her caregiver story, reflecting on lessons learned through her husband’s CLL diagnosis in 1996.
VIDEO: How we Processed Cancer as Husband and Wife
How were you both at the beginning of this journey?
Esther: Andrew, at the point when you got a diagnosis of CLL, both of our reactions were, “What? What the heck? What is this?” For me, it felt very much out of our control. It was like, “Oh my God.” What was your reaction?
Andrew: I thought my life was over. I didn’t say this to you, but I thought, “I’m leaving a wife and 2 little kids. Hopefully I’ve lived pretty well.” But that’s it, because I didn’t have information.
Esther: I think that’s it. That’s what I think I want us to talk about. It seemed to me that what happened was you had those feelings. If I think back, I probably had some of the same. I was like, “Oh, my God, I’m losing my partner in life, and my kids won’t have a father.”
But there was a real transition when you and I talked about it, and we started to get information. My recollection was that we knew somebody who knew how to research these things.
Andrew: Right. When we first went to the oncologist — we’d never been to an oncologist before — and he gave us this diagnosis of chronic lymphocytic leukemia, we were both in tears. We didn’t know anybody, didn’t know what it was, etc.
Our friend David Nudelman helped us on our home computer to connect with others, and ultimately we connected on the phone. If you recall, Esther, I started going to lunch with other CLL patients in Seattle, where we lived. We started connecting, and then it was the search with their help for the smartest doctors.
Esther: Right. You did that in seeking out peers, and in parallel with that, my way of sort of getting my feet under me was to try to get a handle on my emotionalism and to get counseled and use some medication and whatever to be able to be there for you and for the kids.
Andrew: Right. You remember that somebody referred us to a counselor and I think his wife had leukemia. I seem to recall that. He said, “Hey, Esther, you’re kind of an emotional person. Maybe you try St John’s wort as a natural substance to see if it takes the edge off.” You had been opposed to any kind of medicine. You thought it would be “Invasion of the Body Snatchers.” But it worked.
Esther: Yeah, it did. It did work. I think that that’s a real example of how you and I are very different personalities. We’re dealing with gaining some control in what seemed like an uncontrollable situation. At least I remember that once we got to the right doctor, we understood the diagnosis. I do remember that it was a little hard to swallow.
It was Dr. Keating, if I remember. We ultimately got to a subspecialist, special specialist, when he said, “You don’t need treatment, maybe for years.” There was this hurdle to get over of, “What do you mean you’re not going to do anything for years?” Once we got past that, it felt a little bit more controllable, or it felt more calming, I guess. At least it wasn’t urgent.
Andrew: I went from feeling I’d be dead tomorrow to, “We don’t have to do anything right away.” But you’re right; it was worrisome. I think just in the family, [it was] what does this mean? When? How do we go on? What should we say to you? What should we not say to you? When do you go to the doctor again? What did the doctor say?
We had that with our children, certainly Ari, who I think was 6 or 7. He started to ask questions. You remember this, Esther? When Ari asked me, we explained that Daddy had a sickness in his blood. Ari was like 7, and he said, “Will you be there for my bar mitzvah?” [That is] age 13 in our Jewish religion. I said yes, but I didn’t know.
Esther: That’s a whole other topic of, “At what point do you talk to your children, and what can they comprehend?” That’s probably a subject for another time. I do remember that, and I also know that in the situations where people have chronic conditions, there are these ups and downs of waiting, either waiting for treatment or waiting for the next blood test.
I know that when you would go for those exams, there was a little bit of that anxiety again. It’s like, is another shoe going to drop? Is this going to be the time that you’re going to need treatment? And is that a good thing or a bad thing?
I was like, “Okay, we’re waiting. We’re waiting. Now do something.” When they did something finally, I actually felt better than the period of time where they were doing nothing. I don’t know how you felt about it.
Andrew: I felt the opposite. I said, “Oh, my God.” I didn’t want to face it. If you recall, the treatment started in Houston at the MD Anderson Cancer Center, this big monolithic monument to cancer research and treatment.
We were not from Houston and didn’t know anybody from Houston, so we’re definitely strangers there. I did not want to be there. I wanted to just go on, “Yeah, you got this diagnosis, but it’s not really going anywhere. Just let it ride.” I wanted to just let it ride. I was not ready for treatment.
Esther: So there you have it: 2 people, different reactions.
What topics will you be covering in this series?
Andrew: I think there are some funny things that have happened along the way. First of all, meeting some great people. Fortunately, with my illnesses (which have been long term), I’ve gotten to know my providers pretty well — the nurses, the doctors — as people. I think that’s been pretty rich.
There’ve been some episodes that have been screwy, fainting or just memorable moments, that you’ve had to work with your team. Also, just funny conversations you’ve even had with people trying to figure out, well, what’s going on with you?
Esther: I think a couple of topics off the top of my head is that it was very clear when we met with the special specialist that he was the right guy. There were a number of reasons for that. There was our local oncologist, and there was this subspecialist.
I think talking about what it takes to have a good relationship. When do you know you’ve got the right person taking care of you? That’s one. Another, I think, is for people like yourself and like us, how do you broach treatment and longevity and those things with children? With family?
I think relapse. Once somebody is through treatment, how do patient and care partner deal with the specter of relapse? What does that mean? How are the reactions different?
Andrew: How do you plan?
Esther: How do you plan your life knowing that there’s this thing out there that could or could not impact what you think is the ideal future?
Andrew: How do you travel? What if you get sick when you’re traveling? What are your resources? What’s the solution?
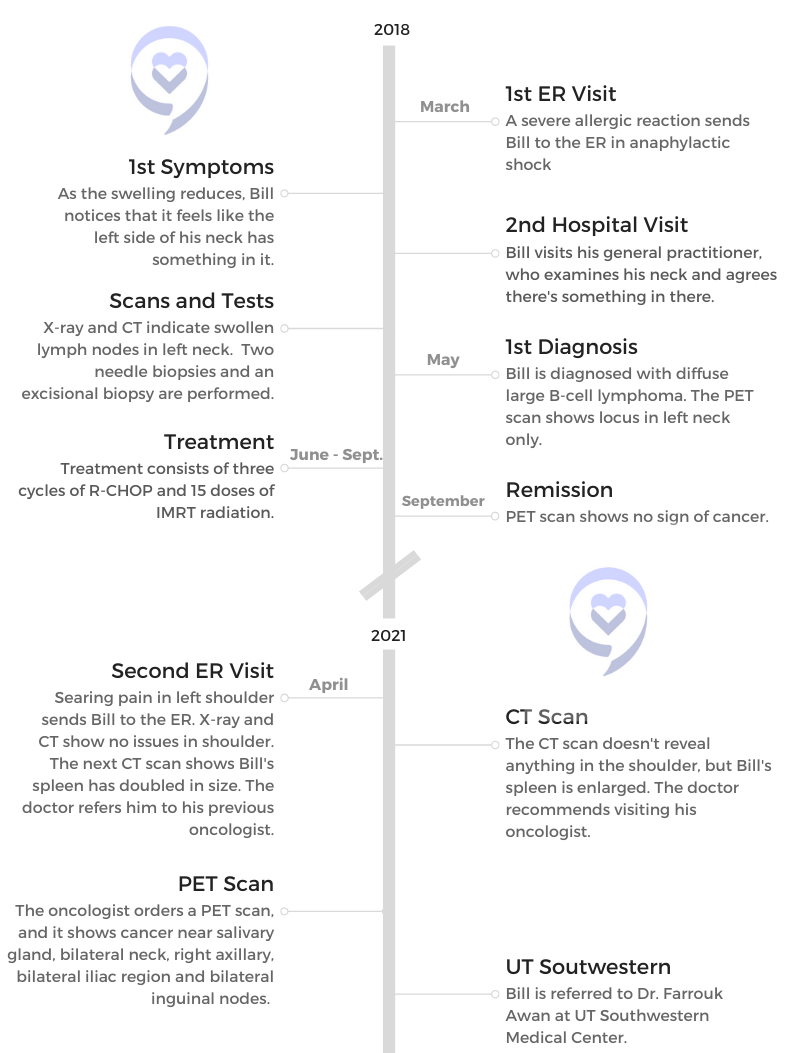
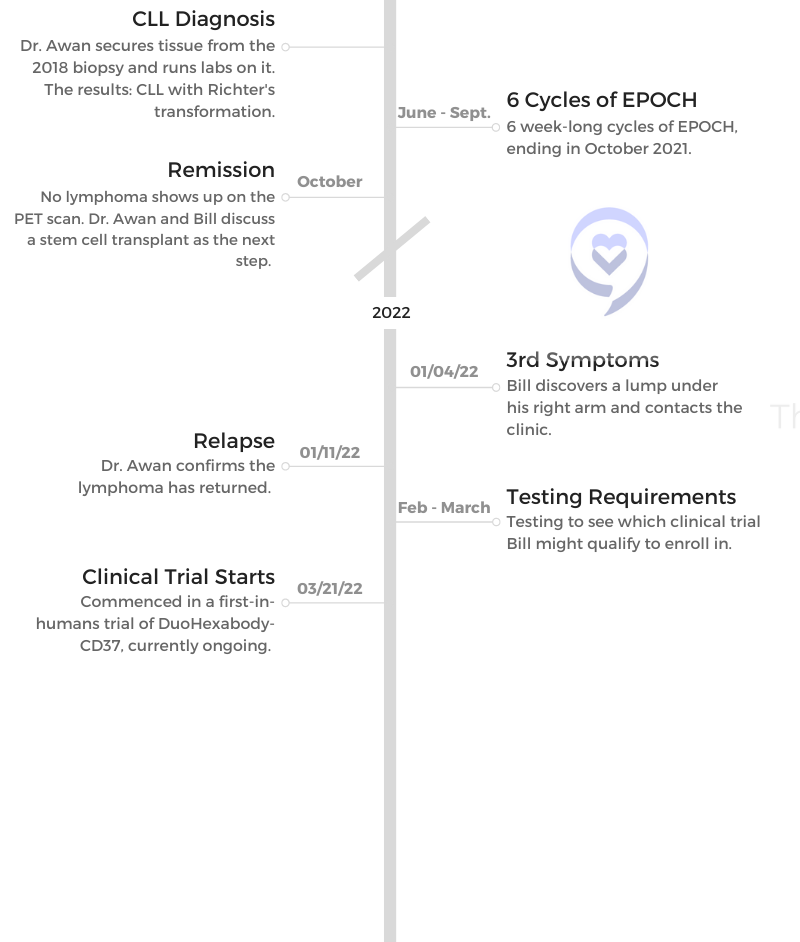
1st symptoms: Tightness, lumps in left side of neck, severe pain in left shoulder, enlarged spleen Treatment (CLL): 6 cycles of EPOCH, clinical trial for DuoHexabody-CD37
Barbara Kivowitz, Caregiver Expert & Author
“A critical ingredient we need throughout our lives in all circumstances is hope. Hope can exist and persist even when a cure is not possible. You can attach hope to anything.”...
"It’s just that tough. It’s scary and difficult, and you need to give each other some space, but also give each other that support and love."
...
Esther Schorr's Cancer Caregiver Story
"You need to take care of yourself as well as you take care of the person that you love so much who's going through it."...
Andrew Schorr: My Chronic Lymphocytic Leukemia (CLL) & Myelofibrosis Story
Andrew Schorr was a healthy runner with a wife and two young kids when a surprise cancer diagnosis changed his life: chronic lymphocytic leukemia, or CLL.
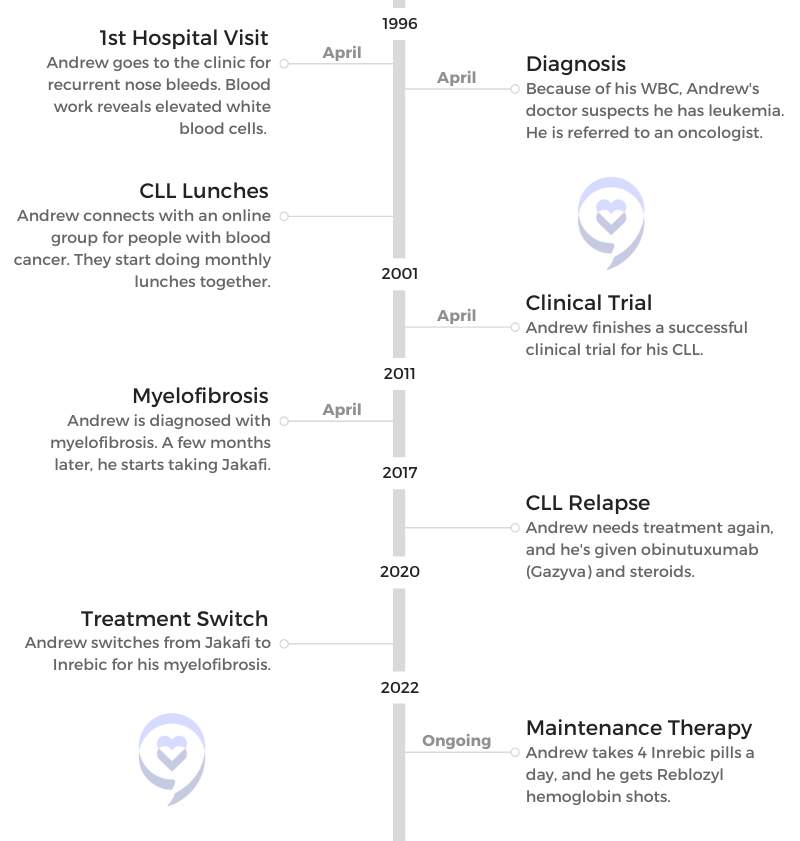
Schorr recounts learning and processing the CLL diagnosis, connecting with other CLL patients through online communities and in-person lunches and benefitting from 2 different clinical trials.
This is part of our introduction to a new series here on The Patient Story, “Cancer Friends,” featuring Andrew Schorr and Esther Schorr. The two co-founded PatientPower.info, a resource for other cancer patients and caregivers to help them through their diagnosis and treatment.
Join us every Sunday for a new “Cancer Friends” episode, airing on our video channel here!
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
While I’d like to plan for next month, next year, 10 years from now, I don’t know if I have that. So today the answer’s yes.
Andrew Schorr
How did you learn you had a blood cancer 26 years ago?
Processing his CLL diagnosis
[My doctor said] If your white count is elevated and you have no reason like an infection, it could be leukemia.
Dun dun dun. You’re really shocked. The only thing I knew about leukemia was the solicitations for the Leukemia & Lymphoma Society, typically with somebody knocking on your door and then showing you a picture of a little 4- or 5-year-old kid with acute leukemia.
That’s all I knew. It wasn’t really clear whether leukemia was a cancer that could affect adults. I didn’t know any of that. He said, “I’m going to refer you to an oncologist.” It was a beautiful spring day, as I said, in the evening. Esther and I took a walk in the park. I was 45 years old. We had 2 small children.
I was thinking, “This is it. I’m not going to live very long.” Leukemia can be a fatal condition, and I thought, “Have I had a satisfying life? And leaving Esther with 2 kids. Oh, my God.” It was pretty tough.
We reached out to a friend of ours, who was sort of a computer geek. Now, remember, this was 1996. There wasn’t a lot going on on personal computers then. Internet speed was really slow.
He came over on our little home computer, and he said, “There’s a news group for people with blood cancers. Maybe you should join and correspond with other people and find out more about this.” So I did.
The lady who ran this group was a woman named Barbara Lackritz, who was a school speech therapist outside Saint Louis and had chronic lymphocytic leukemia, which was the diagnosis I ended up receiving. I typed her a note, “We’re terrified. Can we call you?” We talked to her on the phone. Again, it was one of those spring nights.
Her famous words were, “Chill out. You’re not going to die anytime soon. There are certain doctors who specialize in this illness. My advice to you is to connect with them.”
That is what ended up happening. A couple of things there. One is you don’t know anything about leukemia. You don’t know anything about cancer. You feel your life is over and you don’t know anybody who has it.
Eventually I met other people in Seattle. We started having lunch together. We connected on the Internet and said, “Let’s do lunch.”
CLL lunches
Just to continue for a second, it became wonderful that even online, I knew I wasn’t alone. Esther, my wife, knew there were other spouses who dealt with this as well. In this little online world, very early in 1996, I said, “Hey, I’m in the Seattle area. Anybody else here?”
And, “Oh, I am.”
“I am.”
“I am.”
“I am.”
“Let’s do lunch.”
You go into a restaurant, and there are these people who look pretty normal. They don’t look like they’re at death’s door. You go over, and you say, “I’m Andrew.”
“I’m Gary.”
“I’m Carol.”
“I’m Frank.”
“I’m Susan.”
“I’m Pat.”
We all have a diagnosis of chronic lymphocytic leukemia, and some of them had had it for a while. We had different doctors. Some, I think we had the same doctor. It became very comforting. Then I think we started doing that monthly. Connecting with other patients was tremendous support.
Now, I will tell you, over time, we realized that chronic lymphocytic leukemia was not the same for all people. One person, Gary, had a transplant and ended up later passing away. Somebody else, Pat, who I’m still friends with years later, never had treatment.
Then I was in the middle, where eventually I did need treatment. I just think of us around the table and it became very real that there were other people who were dealing with the same condition. We had something in common, and we were willing to share.
What would you say to someone who has just been diagnosed?
The first thing I would say to particularly a new patient or a family member is the same thing that a veteran patient, Granny Barb Lackritz we called her, said to me, and that is, “Chill out.”
Even more so now, because the options in CLL for getting treatment that will be effective for a long, long time with others coming is very real. I think there’s a tremendous time of hope for all of us and it’s working. That’s part 1.
Part 2 is that one person’s story may not be your story. It can be very individualized. There can be different genetic, genomic differences that make your situation different. You may have other illnesses that affect overall how you’re doing.
That’s why it’s so important to get personalized care. If you do, for the CLL, there are some very effective options. If one of them peters out on you, there’s something else. I think it’s a very hopeful time.
Clinical Trial
Why did you decide to join a clinical trial?
I knew nothing about clinical trials and I would say I was at the starting point [like] many people. They say, “I don’t know if I want to be a guinea pig. What are they going to do to me? Will it really benefit me? Could it benefit others, etc.?” I just wanted to get well.
However, I had already connected then with a world-famous leading leukemia department at MD Anderson Cancer Center in Houston and one of the leaders in the field, a fellow named Michael Keating. When he recommended to me that there was a clinical trial that they were doing, they were the only site in the world adding a targeted therapy, a non-chemo drug to the existing chemotherapies.
They’d already had some experience with it with sicker patients, but they felt it could work for patients who weren’t sick, who were newly diagnosed, had no treatment and that it could do even better. I thought about it, and by then I was starting to develop symptoms after 4 years: swollen lymph nodes and large spleen, fatigue, etc.
There were other trials going on at the same time, including in Boston for a bone marrow transplant. In a bone marrow transplant, you’re kind of out of pocket for the better part of a year. With this other treatment, I was going to be able to continue to work most of the time, so that sounded more appealing than the bone marrow transplant.
I should mention that eventually the bone marrow transplant trial was stopped, but I’d already made the decision to go this other direction. So what did I do? Again, I went back to where I’d been at the time of diagnosis, and that is to connect with other patients. I went online.
“Hey, does anybody know anything about this clinical trial?”
This person in Texas, because it was MD Anderson, said, “I’m a schoolteacher. I’m on that trial.”
“I do roofing. I’m on that trial.”
“Can I talk to you on the phone?”
I did, and I said, “Are you glad you’re in it? Are you glad you’re doing it?” They all were. That patient-to-patient connection gave me some confidence, and [with] the leading scientist doctor, I had to say yes.
It’s scary when you do it because they give you a whole bunch of papers to sign. There were some patients who died very early in the trial, so there was this big black box: “You could die,” basically. Lots of legalistic stuff.
You have the doctor, you have the research coordinator, you have the research nurse, all these people in white coats. My wife, Esther, and I were sitting there. “Sign here.” And we did.
We said, “Okay, when does this start?”
They said, “In about 4 hours. You’re going to that unit, and you’re going to get an infusion.” That’s what happened. I started right away, and that was 6 months of treatment.
Figuring out the logistics of collaboration between MD Anderson and your local HMO
First of all, when I saw the second opinion at MD Anderson, my HMO doctor was not in favor. He said, “We’re not going to pay for you to go to Houston, Texas, from Seattle. They’re going to say the same thing and that is, ‘Start chemotherapy now.'”
I said, “No disrespect to you, but this is my life on the line. I’m going to go even at my own expense.” And I did.
The Houston expert said, “No disrespect for your HMO doctor, but you don’t need treatment yet. When you do, I’ll probably have a clinical trial that would be an option for you and we’ll discuss that. Go home.”
I should also mention that the “go home” was because we had thought of having a third child. He said, “Go have your baby,” which we did. There was a disconnect between the HMO doctor back in Seattle.
I went back to Seattle, and I said, “Dr. Keating says, ‘Wait,'”
“Okay.”
“And that maybe there’ll be a clinical trial.”
“Well, okay. Let’s see.”
I let Houston drive the bus, and the HMO doctor just nodded his head. What happened? We had to work out the logistics. When I needed treatment — swollen lymph node, enlarged spleen, fatigue, etc. — the trial was ready.
Clinical trial
We had 2 little kids, so Grandma and Grandpa, friends, aunts, uncles [helped]. Esther and I were going to be in Houston for at least a week. When you have little kids, that’s a lot of juggling to do. But we pulled it off, went down there, stayed in a little hotel that MD Anderson has across from the clinic, and then got the treatment as an outpatient. That worked out.
As far as expense goes, we paid for the travel, but that seemed like a small expense for the benefit it was going to get. Otherwise, I believe that the care was covered by what insurance I had. We had to pay for travel and work out the family logistics. It was an adventure.
The trial, I fainted the first night from IV Benadryl. That was an experience — the nurses giving me smelling salts, and I hit my head on a bar when I fell. My mouth was bleeding. That first infusion took about 8-and-a-half hours. It was on the final night — we were watching TV in the little room — of the TV show “Survivor.” I was feeling like a survivor on the island.
Then Esther wheeled me back to the hotel across the way in a wheelchair at like 3 in the morning. The trial worked out and it ended up with a 17-year remission, so I’m very grateful for that.
Phases in a clinical trial
Phase 1 is typically first in humans. That doesn’t mean they weren’t testing it in the lab on animals, etc., but first in humans. Often that’s with the very sickest people, where they’re sort of out of options often and that’s a phase 1 trial.
Phase 2, they have it pretty well figured out. Now there’s a larger group, maybe 100 people or more. They’re working. They’re tweaking the dosage. They’re really monitoring for safety, looking for any side effects, anything like that. Fortunately, I didn’t. I had nausea, but I was able to continue the treatment’s 6 cycles.
Then a phase 3 trial often goes worldwide. Now it’s on hundreds and hundreds of people as they’re really getting further data, and they’re looking for little signals of whether side effects or what they call adverse events (things that they don’t want to have to happen) show up.
What happened is that I got this combination therapy known as FCR (fludarabine-cyclophosphamide), 2 chemo drugs, and a targeted monoclonal antibody, rituximab. I was like patient number 70 and I got that combination 10 years before it was approved as a combination by the FDA.
Now, would I have been alive had I just had chemo and not had this Rituxan added and been in this trial? I don’t know. For me, it provided a real advantage and a head start on state-of-the art treatment. I’m very grateful for that. I think it saved my life.
What were you thinking during this process?
There are a few lessons in what I’ve been through. One is that you need to identify a knowledgeable health care team. Ideally, if you believe that medicine moves forward, you need through them — or maybe even additional resources — a window into what could be next or better for what you have.
Then you need to consider, if it’s not approved medicines, is there something that’s experimental in a clinical trial that could potentially offer you an advantage? That was the decision I made, that the traditional approach was not great. It was pretty toxic and did not cause a long remission.
I was 45 years old and then at the time of the trial, 49. I wanted to have a long life. I’m 71.5 now, so obviously it made a big difference. I think you have to really think about your future with people you trust and that’s what I did. It ended up being the right decision, for which I’m very grateful also.
We went ahead and had the hug from our doctor. Keating hugged Esther and said, “Go have a third child. You’re going to be around a long time.” That kid’s 25 years old now. It’s given us a lot of joy. He’s been a kid, so [there were] ups and downs, but we never would have had him. Every time I see my son, that’s a sign of the gift I was given by modern medicine.
The importance of speaking up for yourself
I think you need to be respectful of the doctors and nurses you’re dealing with, but recognize that they may have a lot on their plate. My HMO doctor was tasked with treating every cancer that any member of the HMO would have, with leukemia maybe not being high on the list.
Breast cancer, colon cancer, lung cancer be much higher. He really had spent a lot of time being up on that. Was he necessarily up or totally informed of the latest research for what I had? Maybe not so much.
I, in a respectful way, said, “I know you’re a very devoted doctor, but I want to go the extra mile.”
He said, “We’re not going to pay for you to go get a second opinion, but it’s your right.”
Well, guess what happened? I was eventually in the clinical trial, which was coordinated by MD Anderson Houston and the HMO clinic in Seattle, where I lived. I got them to work together.
How did you get them to work together?
By saying, “Here’s a world-famous doctor in Houston. He signed me up for this clinical trial. You have the medicines available in Seattle. Will you kind of play ball?” They said they would.
I got the remission, and I went back to see my doctor for a check-up in Seattle. I said, “How are you treating other patients now with CLL?”
He said, “Andrew, the same way you got treated because I, as an HMO doctor, learned from your experience being in the trial.”
Lessons about Living Life
What was it like going from the clinical trial back to normal life?
I think the word that applies then but applies every day is “uncertainty.” You don’t know if another shoe is going to drop, either from the medicines you had or from the illness that’s not cured, because it wasn’t cured. It was knocked back. I was in remission.
I would develop a cold, and I realized this pattern over time that it always led to a sinus infection. Then, even though they hesitate to use antibiotics broadly, I always needed an antibiotic and maybe a second course.
You begin to see a pattern of life after treatment. You try to take control of it with your local doctor, and so we did. As a cancer survivor, you’re always concerned is that ache and pain — or that cough you have or whatever — the sign of something more serious?
In the case of CLL, what you’d worry about would be getting pneumonia, which could be fatal. That’s what people with CLL die of: an infection that your body can’t fight off. You have to stay ahead of that. If you have a cough, “Oh, my God, is it leading to pneumonia? Should I call the doctor right away?” You have to take responsibility for that as a patient.
Always saying yes
But that said, the days you feel good, go for it. One thing I’d say about life after treatment is when people invite Esther or me for something or together, invariably I feel the answer’s yes. Do you want to go out to dinner? Yes. Do you want to come to a show with us? Yes. Do you want to go on a bike ride with us? Yes.
Why? Because that’s what life’s about. While I’d like to plan for next month, next year, 10 years from now, I don’t know if I have that. So today the answer answer’s yes.
What guidance do you have for people?
First of all, I’ll mention something about social media. Often the people who post on social media have some more urgent, serious concern. I didn’t post anything.
I just went on with my life and CLL faded in the rearview mirror. I knew I still had it, but it wasn’t affecting my life. I think as you go on, or if you’re in watch and wait but you have no active symptoms that are affecting you, just go on with your life. Yes, you may hear about somebody who has some issue, but today most of these issues can be treated effectively.
If you have the right knowledgeable health care team, that’s part of your responsibility to secure that team. But if you do have the right team, then if you’re in watch and wait or you’re in remission, I think it’s about, “Go do what you want to do.”
Going through Treatment Again
Why did you have to get treatment again in 2017?
I knew that I was not what they call MRD negative, or minimal residual disease or measurable residual disease negative. One of my friends, Dr. Wierda at MD Anderson, had done a test, and he said, “It’s going to come back sometime. It’s going to show up.”
I had that in the back of my mind. Then here in San Diego with monitoring from my doctor here, Dr. Kipps, we could see the white blood count go like that. It did come back. I wasn’t shocked that it happened.
Then okay, it worked before. What do we do now? It wasn’t the same treatment. It was sort of more modernized treatment. And guess what? That was in 2017. We’re in 2022, and the CLL has not been a factor after going through those cycles of that treatment.
My pattern of CLL is to know that it’s there, that it could raise its head again. We’ve talked about this sometimes among patients: Whac-A-Mole. We have effective tools to bop it on its head and then go on with your life.
Editor’s Note: obinutuzumab, or Gazyva, and high doses of steroid
That was because I’d already been diagnosed with another condition, so my CLL doctor had to be very thoughtful about how to treat CLL without negatively affecting the other condition, myelofibrosis. He did it right. It worked out well.
Reacting to the steroid
The steroid was a funny part of it, because when you get steroids, you can get pretty hopped up. They were giving me medicine I could take if I was having trouble sleeping, and I was. But when it wasn’t time for bed, which was most of the time, I was cleaning the house or shopping for groceries.
Esther just sort of sat there while I’m [whooshing around]. If you had a fast-motion camera, you’d see me going all over the house, doing things, going on errands, fixing things, really wired. Then at some point, you crash, and then you do it again. But it worked.
How did you manage the roller coaster of emotions?
You’re going to get through it. I think for anybody who’s been through cycles of cancer treatment, you’re in this tunnel, in a way, but there’s light at the end of the tunnel. There’s a date when you believe you’re going to stop.
You’re getting powerful medicines. You understand that they likely have some side effects. You just have to get through it. When I was originally treated, I developed increasingly serious nausea. If I walked into the clinic, just the smell of the clinic made me nauseous, not even having treatment.
There’s a goal, and the goal is that the treatment hopefully will be finite, and your disease will be controlled. That’s happened to me a number of times.
DVT and Myelofibrosis Diagnoses
DVT diagnosis
I never expected to be diagnosed with anything other than a recurrence of chronic lymphocytic leukemia. Never expected it. I would go to the gym with my wife, Esther, early in the morning, and I noticed that I was getting leg pain in my right calf. Pulled a muscle, right? Gym, makes sense.
It continued a second day and a third day. We were actually at a shopping mall near where we lived. This was in Bellevue, Washington. We’re going from one side of the mall to the other, and I’m limping, trying to disguise it for Esther. I didn’t want her to really say, “What’s wrong?”
Anyway, it’s in the evening. We get home. She’s putting our youngest child to bed. I’m kind of concerned, and so I called the consulting nurse through our insurance company — the little number on the card if you have that kind of insurance. The nurse said, “I’m going to get the doctor to call you.”
We were in a program. My wife worked for Microsoft and they actually were testing doctors making house calls. The doctor called, and I said, “I’ve got this pain in my leg.”
He said, “Is your calf red?”
I said, “Yeah, it’s little red.”
“Is it warm to the touch?”
“Yes, it is.”
“Do this maneuver with your leg: turn your ankle, do the stretcher. Does that hurt?”
I said, “Yes, it does. It’s a pulled muscle, probably.”
He said, “I don’t know about that.”
I said, “Do you want to come make a house call?”
“No. I want you to go to the emergency room.”
“When?”
“Now.”
I said, “Do I need to call an ambulance?”
“No.”
I said, “My wife and kid are asleep.”
Going to the hospital
I snuck out of the house at like 11:30 at night. I didn’t want to wake them. I drove to the hospital. He had called the emergency room to tell them I was coming. They did an ultrasound. It was the weirdest experience because the ultrasonographer, in those days anyway, she was moving the ultrasound wand around your body, and then she was talking to the machine.
I guess it would make some recording for the radiologist or whatever. I had no idea what she was saying. She did the right calf, and then she did the left leg. I said, “Why are you doing left leg? I don’t have any pain there.”
She said, “That’s the protocol. We have to do that.”
I’d had a cough at the time, by the way.
A little while later, the emergency room doctor came in. He said, “Congratulations, you have a DVT, a deep vein thrombosis, a blockage in your right calf. You also have one higher on your leg on the left side that you don’t feel, but it’s there. And guess what? You’ve got pneumonia, and I’m putting you in the hospital now.”
Anyway, I finally called my wife. Then the family heard about it, and they’re all showing up the next morning. I’m hospitalized for this DVT, which you can die from if it goes to your lungs, called a pulmonary embolism. All right.
Clinical trial #2
As I was finishing treatment over a few days, there was a guy who’s sitting in a chair in my room. “Who are you?”
He said, “I’m a clinical trial coordinator. We have a trial for a blood thinner to prevent DVTs, recurrence of DVTs. Would you like to be in it?”
I thought, “I’d been in a clinical trial for chronic lymphocytic leukemia. It worked. Now I’ve got this other thing. I don’t know what the hell it is. Maybe that’s a good idea.” So I signed up.
I was in the clinical trial for a blood thinner, and they were monitoring me, which they do very carefully when you’re in a clinical trial. They do all kinds of stuff, EKGs and blood tests and regular visits. You’re like a VIP. I love the attention. It’s great.
Then the principal investigator called me and said, “Something’s out of whack with your blood. Not blood thinner stuff. You need to go back to your hematologist here in Seattle.”
So I did, and he drew 10 tubes of blood. Okay, then I forgot about it. I was in the trial center. I went to the major convention for blood cancers, called American Society of Hematology. I tried to go as sort of a reporter every year.
Myelofibrosis diagnosis
I was getting out of the taxi one day there at the convention center, and the phone rang. It was a Seattle doctor. He said, “I got to talk to you.”
I said, “What?”
He said, “You have a blood cancer.”
I said, “Chronic lymphocytic leukemia? I’ve already had that.”
He said no. He said, “Myelofibrosis.”
“What the hell is that?”
He said, “It’s scarring in your bone marrow.”
“How do you know?”
He said, “We did genomic testing. You have the condition, and it’s driven by the gene called JAK2 V617F.” This is like gobbledygook, right? “Therefore, we know it’s myelofibrosis.”
I said, “What do you do about it?”
He said, “Nothing right now. Someday you might need a bone marrow transplant.”
I was scared. The only other thing I’ll say about the diagnosis was I’m now at a convention of 30,000 hematologists. Now, I knew a lot of them from CLL, and they were very upbeat about new treatments for CLL, which have continued. They were very upbeat. “CLL, oh yeah, we got a lot to offer patients.”
I said, “I may have this other condition, myelofibrosis,” and their face would fall. I knew it was fatal, potentially fatal, and that they didn’t have a lot to talk about.
Myelofibrosis treatment
I happen to know the doctor who is world famous, who had interviewed previously about myelofibrosis, although I didn’t know much about it.
He said, “Come see me in Houston.” He was an MD Anderson specialist, a world expert. He said, “We’ve got something to talk about now.” The funny thing was, at the same convention, they have exhibits of different drug companies and stuff like that. There was this little booth for a company that had just gotten approval for the first inhibitor of this JAK V617F gene to tamp it down for people with myelofibrosis.
Guess what? A few months later, that newly approved drug became my treatment, and it was highly effective. Diagnosed with something I never heard of again. Stranger in a strange land. Thank God medical science had something to offer, which worked.
Maintenance Therapy
Can you describe what it’s like to be the person who has benefitted from clinical trials twice?
When you talk about cancer, I wish we could say there’s been miraculous progress in every cancer. That’s not true, but there’s been a lot of progress, and it continues. I think I’m just a really lucky guy that the illnesses, the cancers that I’ve been diagnosed with, have been treatable in ever more refined ways as I’ve lived with them. Thank you, God, that I’m living at a time where there’s been progress for what I have.
I think my advice to patients and family members is turn over rocks. Not with false hope, not somebody selling you snake oil, but with validated, real evidence-based information. Is there somebody or something for you that could make a difference and is an example of medical progress for what you have?
Now, I’ll step back for one second. In cancer, there are a lot of people who don’t have the appropriate testing or the most knowledgeable pathologist look at their blood or their tumor type. They get a misdiagnosis, or there’s not a clear test that’s done to show their version of a cancer.
Job 1 is to know what you’re dealing with. Job 2 is to have a health care team that’s knowledgeable in the full range of options.
I think Job 3 is to have hope that with the right team, with the right diagnosis, that either now or coming soon, there may be something that can help you. If that helps you but peters out, there may be something waiting in the wings to help you even better. That’s what’s happened with me.
Switching in 2020 to another recently approved treatment
The original medicine I was on to inhibit the myelofibrosis, the trade name is Jakafi or Jakavi outside the U.S. The generic name is ruxolitinib. You learn these long words.
Then when I came to San Diego on that drug, eventually my specialist — who’s also a scientist and had done a lot of the groundbreaking work in another drug in that class, fedratinib or trade name Inrebic — said, “I think this may offer you some advantage. Let’s consider changing to that.”
I did, and it’s worked well. I trust in my doctor. Both medicines have worked well, and I’m leading a pretty good life.
Pills and hemoglobin shots
That Jakafi I took, I don’t remember what color the pills were. Sometimes the dosage moves around over the years. I take 4 of these red Inrebic pills every night, and then your blood counts are monitored. My hemoglobin was going down, and going down lower than I’d ever had before.
My doctor, Dr. Jamison, has had good results using a drug called Reblozyl (the trade name). Luspatercept is the generic name. It’s not approved for myelofibrosis, but she’s getting Medicare to pay for it through some scientific argument that I don’t understand.
You get a shot pretty quick, either in your belly, your abdomen or your arm. The nurse gives it to you at the clinic. That boosted my hemoglobin from a low of 8.8 to 11.5. What did that mean? It made the difference for me. Huffing and puffing going up a flight of stairs to being able to ride my bike and not feeling like I needed to lie down. I’m very, very grateful for that.
I’ve done that about 3 or 4 months now, and I’m very grateful that that exists.
How have you managed everything?
I think you have to be a proactive patient. It may be your spouse or your adult child or your best friend. I think you have to look for answers. Not false answers, not phony answers, but you have to look for real answers and providers who are knowledgeable.
I’m very grateful that I’ve been able to do it. But I had to look. I had to push for that. I had to be a consumer. So many people are smart shoppers about buying a house, buying a car, buying a new sweater. Why should it be any different if you’re facing a life-threatening cancer? You’re not a little lamb. You and your family are consumers, so be savvy.
I would say be positive. We’re going to find the right answer. We’re going to find who’s in the know. We’re going to find and get a full understanding of our options. Both what’s approved, what’s maybe experimental, what could make sense. We’re going to find out where there’s financial assistance.
In the meantime, we’ve been given time. If you’re having some good treatment, what does it give you back? It gives you time. Then you can’t say, “I’m going to ‘woe is me’ and mope.” You have to say, “I’ve been given today. What am I going to do with it? What am I going to do that’s positive today?” That’s how I approach every day.
1st symptoms: Tightness, lumps in left side of neck, severe pain in left shoulder, enlarged spleen Treatment (CLL): 6 cycles of EPOCH, clinical trial for DuoHexabody-CD37
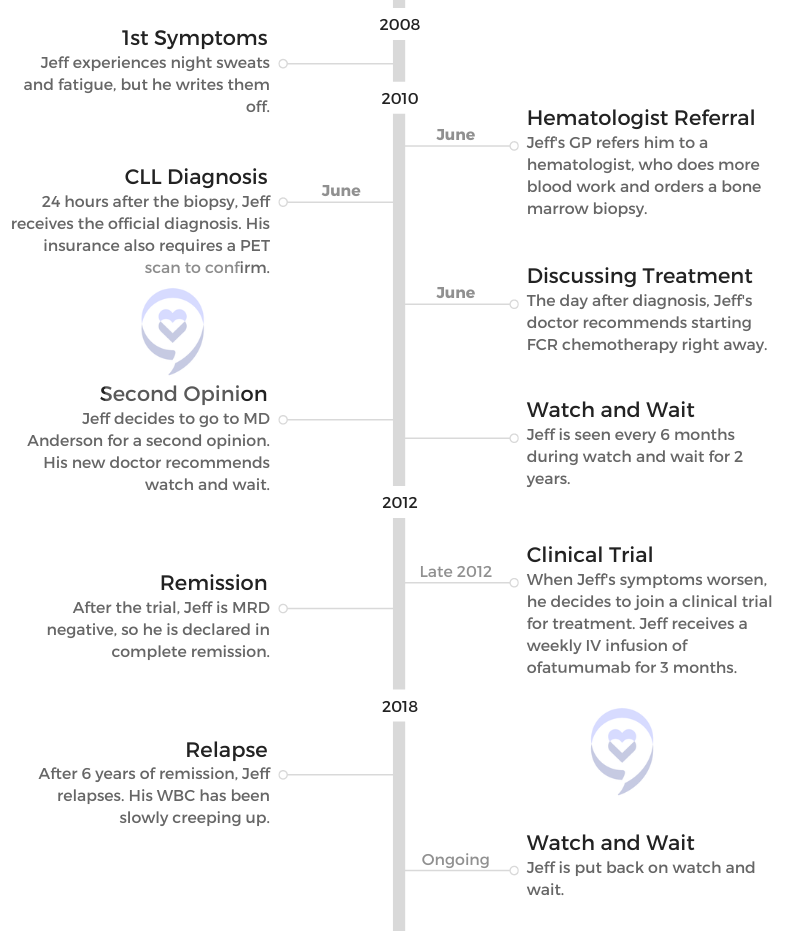
When Jeff started experiencing fatigue and night sweats, he didn’t expect to be diagnosed with chronic lymphocytic leukemia (CLL).
Jeff’s story includes undergoing watch and wait, joining a clinical trial, reaching remission and going back on watch and wait.
Along the way, Jeff learned some important lessons that he shares with us: getting a second opinion, cutting out unimportant things and finding humor in all situations.
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Go live a great life, because it absolutely is possible.
The CLL Diagnosis
Introduction
Tell me about yourself
I always start off by telling people that I am a very shy introvert. I count to 3, and then I start laughing because that is 180 degrees opposite of what I truly am. From a very young age, I have been a public speaker. I loved being on the stage and connecting with people, and that’s one of the things that gives me a ton of pleasure. I continue doing it to this day.
As far as the best part about me, I think I have the most awesome daughters and awesome wife in the entire world. My family has been absolutely wonderful throughout this — we’ll call it a “journey.” It’s not a journey. It’s a pain in the butt. They’ve been absolutely great, and I love the fact that we have so much closer of a relationship now. I’m going to say that’s partly due to CLL.
What were your first CLL symptoms?
I was in my mid-40s at that time, and I just thought things were normal. I had some family history of some issues — some high blood pressure, some high cholesterol — and I was seeing my doctor regularly to keep that managed and under control. I like to use the term being a “compliant patient” [for] following those instructions.
I really didn’t notice that the symptoms I was having were out of the ordinary. I love Thai food, and I eat a lot of Thai food. Occasionally, I would get night sweats. I was thinking, “Hey, that’s just eating too much spicy food before I go to bed.”
I was tired all the time, and I was like, “Okay, this is what it’s like to be male hitting midlife, and you run out of energy.” It turned out that was wrong.
I’m very fortunate that my GP, who I still see every 90 days, was keeping tabs on things. He said, “Look, something’s wrong. I don’t know what that something is, so I’m going to get a pinch hitter. I’d like you to go see a hematologist, and let’s find out what’s going on.” And that’s what I did.
The CLL Diagnosis
What was the first indicator to you that this is something very serious?
Unfortunately, I remember exactly how I felt throughout that entire process, because it was a part of my life where everything changed in a very compressed period of time. My GP said, “I need you to go see a hematologist.”
I was like, “No problem. I see specialists all the time.”
He said, “I’m going to make the appointment for you.”
Okay, fine. The appointment was made for the next day. Great. Not a problem. I was doing okay right until I got into the hematologist’s office. I didn’t think that cancer was a possibility, and I didn’t think anything major. It was, “My doc wants to check off some boxes.”
Literally, it was like somebody had taken a baseball bat, swung at full speed right into my gut, and just took all the air completely out of me.
Seeing the hematologist
When I walked into the hematologist’s office, everybody in there was old, ugly and sick. That’s what it looked like to me. I realize that sounds like a generalization, but I’m thinking to myself, “What in the heck are you doing in this office?”
[I] got ushered into the back, and the hematologist looked over the blood test results that my doctor had sent over. He said, “Nope, I want to do this myself.” They drew some blood, and he said, “Nope, this is not good. I need you to come in tomorrow. Bring your wife. She’ll have to drive you home. We’re going to do a bone marrow biopsy.”
Jeff spoke at the high school for his daughter Zoe’s class.
I can give you a really detailed description of what a bone marrow biopsy is, and I guarantee you you’ll feel it after I tell the story. But the TL;DR (too long; didn’t read) is you lie down on your belly, they shove a corkscrew in your hip, and they pull out a bunch of tissue.
Then 24 hours later, I learned that I had leukemia. In a period of 48 hours, I go from being a tired, middle-aged dude to, “You’ve got cancer.”
What was your reaction?
The moment was a phone call from the doctor, not the doctor’s nurse. He had reviewed the bone marrow biopsy results, and he said, “I would like you to come back into the office with your wife.”
I said, “Well, I kind of know where this is going. Why don’t you just tell me what’s going on?”
He said, “No, that’s not how we do things here.”
I said, “This is how we’re doing things here. I promise I’ll come in tomorrow, but I need to know what’s going on.”
He said, “Mr. Folloder, you have leukemia, and you need to come in tomorrow so that we can discuss how we’re going to treat it.”
Literally, it was like somebody had taken a baseball bat, swung at full speed right into my gut, and just took all the air completely out of me. My wife and I freaked out — and I still get misty about it — but we kept our word.
We went to the doctor again the next day. He scribbled some things on a pad, and he tried to explain what chronic lymphocytic leukemia was and why it was an important cancer. Then he said, “We need to start treatment right away.”
I was like, “Wait, wait. I’m just a little bit tired. Why do we have to start treatment right away?”
He said, “I want to put you on what we call the gold standard of care,” which was a combination therapy called FCR that was very popular at the time and is still used somewhat today.
I started taking very deep breaths. Then for whatever reason, he decided that it was important to tell me that I should expect to live 6 years. That’s when I stopped breathing heavily.
I was like, “Okay, this is a lot to digest. My wife and I are going to head home, and we’re going to talk about this. We make decisions as a team.”
Patient-Doctor Relationship
Deciding to get a second opinion
We got home, and we started talking. I looked at my wife, Penny. I said, “He’s fired.”
“Wait, what? What?”
“He’s fired. I’m not going to work with anybody who’s putting an endgame on my life right now. I don’t feel comfortable with this guy.” We’ve got friends and family that work at one of the greatest cancer centers known to the entire universe. It was time to get a second opinion, like right now.
‘You may die with this. You’re not going to die from this. What we’re going to do now is absolutely nothing.’
Jeff’s 2nd Doctor
I called up my aunt, who worked there at the time, and told her what was going on. I said, “Look, I get it. The diagnosis is not going to change.”
She said, “Well, you’re probably right about that.”
“But where you are, the treatment options are huge. I want to make sure that the treatment that I get is the right one for me, so can you get me a hookup?”
It’s very bizarre for a mid-40s somebody to be asking a mid-60s aunt to “get me a hookup. I need to see the right doctor.” But that’s exactly what she did. Literally that same week, I got into that hospital, and I saw one of the world’s leading experts on CLL. My entire trajectory changed for the better.
Can you describe the concept of firing your doctor?
Not every doctor has the best training in how to communicate with patients. Some do it much better than others. For me, having a sincere, candid conversation that’s not dismissive is crucial to me being able to relate to the doctor and to be able to be that compliant patient.
My doctor, that first one, had basically already written me off. In my playbook, that wasn’t going to work. In the communities that I help lead and help advocate for, we tell everyone, “Your doctor can be great, but you have to get a CLL specialist on your team.”
He doesn’t have to play the lead. She doesn’t have to play the lead. But you owe it to yourself to get a CLL specialist as part of the team. Even though your local hematologist may mean well, they’re seeing every type of blood cancer patient.
A CLL specialist, that’s it. All they do is CLL, and getting that perspective can be life changing and mind changing.
To put a really bright underline under that, the person that I saw at this giant hospital in the Houston area asked me, “What did the first doctor want to start you on?”
I told him, “He wants to start FCR right away.”
He said, “That’s really interesting.”
I said, “Why is that interesting?”
He said, “I helped invent the FCR treatment. I know all about the FCR treatment. It’s a really good treatment, and yeah, he’s right. It’s a gold standard. But it’s not right for you.”
I took a really deep breath, and I was like, “Okay, this doctor is really out there in terms of how big his ego is.”
“I invented it.” That’s kind of cool. But he was able to bring me down to a calmer place. “We’re not going to do that because I don’t think it’s right for you.”
I was like, “What is?”
He literally picked me up off the chair, gave me a hug, and said, “Look, you may die with this. You’re not going to die from this. What we’re going to do now is absolutely nothing.”
I was like, “Hold on a second. It’s cancer. We’ve got the early diagnosis. What about the whole program — find it early, attack it hard, go after it, then go live your life?”
Jeff with John Brown, who he describes as a father figure from diagnosis through treatment and relapse.
He said, “Yeah. Sorry. Not how this disease works. We’re going to keep eyes on you, we’re going to keep eyes on your blood, we’re going to keep eyes on your symptoms, and we’re going to keep eyes on, ‘How is Jeff doing? How is Jeff living?’ We are here to help you have the best possible life, so we’re going to monitor closely. When it’s time, we’re going to treat you with the best thing that’s available for you at that moment.”
That’s exactly what I needed to hear. That’s the kind of doctor relationship that I needed. Tell me what’s going on. Don’t pull any punches. Make it personalized. At least connect with me as a human being to make sure that I understand you get it. Living a great life is important. That was a big deal.
He also picked my wife up out of her chair and hugged her, and she was like, “Wait, why am I getting this hug?” But be that as it may.
Working with both your local hematologist and a large cancer center like MD Anderson
That is a very common setup. There are great cancer centers all over the United States — all over the world, actually. A lot of them are just doing amazing research and doing some really cool clinical trials and good work to connect with the CLL community. They do realize at their core that as hard as we try, as great as some people’s insurance is, it’s just not possible to make that physical trek to a center of excellence, if you will.
Most of the professionals that I’ve talked to in my patient advocacy work refer to it as the quarterback scenario. The local guys, the local gals — they’re the team. They’re the ones who are meeting you face-to-face and making sure that your care is done on a regular basis.
The CLL specialist absolutely can be seen every now and then, or just once to call in a play to make sure that your local people are on top of what the latest and greatest are. I know lots of people who do just that, and they’re getting great care.
The importance of finding the right doctor
It is something that does have a long-term element. I’m couching my words very carefully right now, because when I was first diagnosed, nobody used the word “cure.” [It] was not part of the language of CLL. Here we are, a dozen-plus years down the line, and for a bunch of subsegments of CLL, the doctors are now starting to toss that word around: “cure.”
This could be a long time, but for some of us, that could still be a finite long time. We see the end of that road. It is really, really important to connect with your doctor as someone that you can get along with. I remember very early on, I was connected with a person on one of the Facebook support groups who wanted to come to the Houston area and meet with the same doctor that I was seeing at MD Anderson. I thought it was great.
I said, “Look, I know this is going to be scary because you’re coming in from Florida and this, that, the other thing. I’ll tell you what, I can carve out some time. I’ll come meet you at the hospital. I’ll sit with you while you’re waiting to see them. We’ll chat and we’ll get some lunch.”
She did the appointment. She came back out. I went, “How did it go?”
“Can’t stand him.”
I was like, “Wait, what?”
“No, he and I? No, this is not going to work.”
“Tell me what you don’t like,” and she did. I said, “I got this one,” and I wrote a name down on a piece of paper. I said, “Not right now, [but] when you get home, call this doctor. Sorry, she’s not in Florida. She’s up in New York, but I think you’ll get along great with her.”
Sometimes you don’t make that connection the first time. Even if you’re seeing one of the greatest CLL specialists in the world, the personalities may not perfectly mesh. Keep trying. It may take 1, 2, 3, 4 appointments, but you have to find somebody that you can be comfortable with, because this is going to be a long-term relationship.
The patients and their caregivers are not nearly as polite about it. “Watch and wait” is on the borderline of being sarcastic because sitting there doing nothing is so 180 degrees from what everybody has been told about cancer for their entire life.
While you’re in watch and wait, you may be watching. You may be waiting. But you’re worrying, and you’re freaking out about every single, solitary thing because anything that goes wrong, you [think], “That must be the cancer. That’s the CLL kicking in. I’ve got a rash. Ooh, that must be CLL. I can’t do this. Must be CLL.” It becomes this waterfall that you just can’t escape, and it’s constantly beating on your head.
Can you explain getting through knowing you had cancer but not treating it?
I think the best word that I can use to describe watch and wait or conscientious surveillance is that it’s “oppressive.” That’s the best word that I can use for it, because every day you do have to parse all the things that you’re feeling and figure out what can be dismissed as just being normal and what is actually salient that you need to communicate to your team.
Every time you go to have a meeting with the team, they always tell you, “We want to know everything. Don’t leave anything out.” Of course, I started this off like every typical male patient ever does. I would go in for my regular appointment. In the beginning, I always brought my wife with me. The nurse practitioner would come in. The first question that was asked was, “So, how are we doing today?”
My typical male response was, “Fine,” and I left it at that silence.
“So you’re doing okay?”
“Yeah.” My wife [was shaking her head] back and forth.
“Ma’am, you want to tell me what’s wrong with your husband?”
It’s learning how to get past the, “I’m a strong man. I can’t show any weakness,” to, “Okay, I got some crap going on. Here’s what’s happening. What do I need to be worried about?”
As we progressed through not just months but years of that watch and wait, I learned how to be a better communicator with my doctor, with the mid-level practitioners and with my wife about, “Okay, this is important. This is not so much.”
What helped you with the oppressiveness of watch and wait?
I am what most would consider a Type A personality. Add on a soupçon of OCD, and you have a really good description of how my life has been. My biggest problem right up until my cancer diagnosis was that I was an inveterate list maker. I would make tons and tons of lists of all the stuff that I had to get done: stuff I had to get done short-term, mid-term, long-term, plans. This, that, the other. That’s how Type A people are.
The oppression of watch and wait combined with that was not a good mix. As a matter of fact, it was somewhat toxic, and I was getting very frustrated with myself. [I was] getting very frustrated with my family, getting frustrated with my cancer, and getting frustrated that everything was conspiring to make sure that I didn’t get stuff done. Quite frankly, that sucked because that’s not how I had lived my entire life, and I’m not exactly sure what all came together.
It was probably about a year into watch and wait when I came to the realization that I simply couldn’t do it all anymore. It’s not that there wasn’t enough gas in the tank; it’s that I didn’t have enough bandwidth to do everything all the time, 24/7, anymore because things had changed.
I did pull out one of those classic bright yellow legal pads, and I drew a line down it. On the left was stuff that I keep, and on the right was stuff that I throw away. I literally made a big important list that said, “This is all the stuff that’s worth doing. This is all the B.S. that just doesn’t deserve my time right now.”
I stopped doing that B.S. stuff. I cut a bunch of stuff out of my life, and I told people and commitments, “Sorry, you’re on your own.” I had to claw back time for myself. That is how I dealt with watch and wait. I was able to pull up the parking brake and do something that not many people get an opportunity to do, which is reevaluate your life, throw away all the bad stuff and focus on the good stuff.
Self defense training as a stress reliever
Did you cut out relationships and tasks that weren’t meaningful?
It’s all of the above. An example would be: most Type A OCD leaders believe that the best way to do a job is to do it yourself. I wound up doing everybody else’s job in addition to doing my job, and that came to a crashing halt.
“Well, here’s the deal. I hired you to do this job. Do your job. If I don’t like the way you’re doing it, I’ll find somebody else to do your job.” That sounds very perfunctory, but it was a life-changing moment for me because I no longer took it personally. If someone that I worked with failed, it wasn’t my fault. It’s their fault. I could put that on the “do not do” side of the list and make it go along.
As part of still living life, Jeff went to a ZZ Top performance.
Having a mindset change
I was traveling a lot for work. This was long before COVID, everybody discovering Zoom and teleconferencing, and all that stuff. I stopped doing a lot of the traveling. I started taking more time to do the things that made me smile.
[It could be] something as simple as instead of getting on a plane and flying to Atlanta, jumping in the truck, driving, actually enjoying the drive and seeing the country. Put on some jazz. Smoke a cigar while I’m driving (don’t tell the doctors). Have a good time. It was a mindset change where the important stuff is important.
Let’s make sure I have enough energy to do the important stuff instead of shortchanging the important stuff. Things like dealing with neighbors’ problems. It used to be, “Hey, I’ll get this taken care of for you. I know who to talk to.” No, not on my list anymore. I realize that a lot of this sounds trivial, and it is trivial right up until you realize how much time and energy you’re wasting on a lot of that stuff.
Asking for Help
How does financial toxicity affect people?
The financial toxicity side of this is the biggest fear stop sign that I deal with in these support groups. Everybody is really, really jazzed about the fact that we’ve got so many new, good, effective treatments coming. Everybody’s really, really thrilled about the fact that side effects are easy to manage. They’re really, really pumped about the fact that access to these is becoming more and more widely available.
What takes the wind out of their sails is $4,000 a month, $10,000 a month, $13,000 a month or $27,000 for a bag of medicine. People wonder how they’re going to get that bill covered because there’s so many different questions. We don’t have enough time. We don’t have enough energy. There’s not enough gas in the tank to debate the health care system.
Medical insurance, at least in my mind, is not insurance. It’s a way to spread the payments over a lifetime. Some people have programs like that. Other people don’t. I struggle with that because I know that there are patients who could be helped who can’t access that help for want of money.
Not knowing about assistance programs
There are programs out there, foundations, associations, nonprofits and even the drug companies themselves. All of them have a whole bunch of fabulous programs that can help people with the financial burden. The big problem is people don’t hear about that until long after they get the price tag upfront.
There’s no shame in saying, ‘Yes, I need some help.’
You get the shock, you get the freak-out, and you get the, “Oh my God, I can never do this.” Then maybe you’ll get information about how you can cover shortfalls down the line, or maybe you don’t get that information and just walk away.
That’s disturbing and upsetting for me because, yes, I believe that everyone should have access to this medicine. That doesn’t always come through right now. I want everybody to be helped, and I can’t help everybody.
What are some of the assistance programs?
The first 3 that I bring up:
The Leukemia & Lymphoma Society (LLS). These folks have great education programs. They have great learning programs. They put a lot of stuff on the plate, and they also have patient assistance programs. People can apply for these programs. They open and close regularly, and most of them don’t even have an income barrier. Sign up, and you get an LLS gift card to help defray your costs.
The PAN Foundation is a great group of people who do nothing but make sure that people who need patient assistance get patient assistance.
Then the third one, which I think is the most important one: the drug companies themselves. Everybody forgets to go ask the drug company. Quite frankly, although we’re talking about this in terms of cancer, any medication that you’re prescribed that doesn’t have a generic, I always recommend [to] go to that company’s website. Chances are there’s a copay assistance program available for you. They’re there, and they’re available.
If somebody wants to give you $10, $50, $1,000 or $10,000 to help you with your treatment program, take it. There’s no shame in saying, “Yes, I need some help.”
What’s your message to folks who are nervous about asking for help?
This is critical to a successful patient experience. If you’re male [you think], “Everything is okay, and nobody’s going to see me being vulnerable.” It doesn’t quite work. I know it’s part of being a guy, but it just doesn’t quite work. This is heavy stuff. This is big stuff, and there are people that can help you with that big stuff.
I was having a conversation with a gentleman who actually, of all things, was my life insurance salesman and is still my life insurance salesman at this time. I had let Keith know that I had been diagnosed with leukemia. We talked for a bit, and he said, “You probably need to call these folks at CanCare.”
I was like, “What’s CanCare?”
He said, “They’re a really cool support group.”
I was like, “No. Stop. I’m not sitting around in a circle singing Kumbaya with everybody and learning how to pass a peace pipe. No, not going to do that.”
He said, “No, they do things a little bit different. There’s no group support thing that they do. You call them up and let them know what’s going on, and they match you one-on-one with someone who’s just like you that’s gone through what you’re going through.”
I thought to myself, “That’s not bad. That sounds doable.” I called CanCare up, and I got connected. Lo and behold, I acquired a CLL Sherpa, and this person was like me. My age, male, same goals, family and all that stuff. He’d been there, done that and got the T-shirt.
Getting rid of some of the burden
It was great to be able to talk to somebody who knew what I was going through. Frankly, that’s getting rid of a burden. Watch and wait — it’s oppressive enough having cancer. It’s oppressive enough. Going through all of this is oppressive enough. Being able to get rid of some of that burden is a big deal.
If things aren’t going 100% right, let the team know. Let your significant other know. Let your best friend know. Let somebody know, because you can get help, and you don’t have to do this by yourself.
Jeff has a passion for F1 racing
Clinical Trial Experience
Joining a Clinical Trial
Time for treatment for CLL
I can remember the appointment that I had at Anderson when we were going through that evaluation. I said, “Yeah, the fatigue is beginning to kick in.”
They asked me, “Well, what does that mean?”
“That means that I’m crashing a lot earlier and a lot harder than I used to, and I’m missing out on some stuff.”
“What do you mean, you’re missing out?”
“I can usually stick it out, have an extra cup of coffee, maybe throw down a chocolate bar or something like that, and get everything done that I needed to get done. Now, sometimes I go, ‘This is going to have to wait because I don’t have enough gas in the tank.'”
That’s when my team went, “Okay, it’s time for treatment.”
I wanted to say, “Wait, all I had to do was say that earlier, and we could have started treatment?”
“No, we needed you to be honest, and you’re being honest.”
It was the combination of my blood work, my symptom load and my quality of life. That matrix all came together, and it was time for treatment.
Why did you decide to do a clinical trial?
For many, clinical trials are this big, scary thing that sounds like, “I’m going to be a guinea pig. I’m going to be a lab rat.” I’ve since learned that’s somewhat of a misnomer. A lot of times when you’re offered the prospect of a clinical trial, it’s not very on early in the clinical trial. It’s down the line.
As it was explained to me, “This will give you the opportunity to get access to medicine that we already know is going to be beneficial. We’re just fine-tuning it at this point. It will be as good or better than the standard of care.”
When it was presented to me in that way, my next question was, “So what happens if I get the placebo?”
“There’s no placebo. You’re getting the medicine. Downside: you may experience some side effects, but we think those side effects will be less than the standard of care.”
Pizza was the only thing Jeff could eat during treatment.
They need to be able to connect with patients who are the right targets for that treatment.
Jeff comfy in his flip flops at the hospital.
I said, “Okay, sign me up. I’m in.”
Then a nurse walked in with a stack of about 6 inches of informed consent that I had to go through. That was a bit of a nightmare. I was completely comfortable with my doctor, who had already demonstrated his prowess by saying, “I invented FCR. We don’t do FCR for you. We should do this because it’s going to give you the best shot at a complete remission for the longest period of time with the least amount of side effects.”
I want to ring this bell one more time: the fact that I was getting this message not from a generalist, but from a CLL specialist. This is somebody who eats, drinks, sleeps, breathes CLL 24/7. That doctor sees more CLL patients in a day than most generalists will see in a year. That has gravitas.
Later in a clinical trial, what are the other considerations and questions patients and care partners should be asking?
The very first question that they should ask is, “What’s this going to cost me?” We have to be candid. Medical research is really, really expensive, and it doesn’t always yield success. There’s a lot of swinging and missing that Big Pharma is doing in order to get a successful treatment.
When they get further down the line — stage 2, 3 and 4 of their clinical trials — they’re getting to points where we’ve got this. We’re just rounding this corner. We’re sharpening this edge. They need to be able to connect with patients who are the right targets for that treatment.
Like you mentioned earlier, CLL is not the most common cancer out there. In the United States, maybe there are 15,000 new diagnoses in a year, and you’ve got a couple of drug companies trying to create a drug for a small subsegment of them. Treatment sounds really, really good, but if I can get it for free, that sounds even better.
Even though I had great insurance at the time, quite frankly, my insurance company (me) didn’t have to pay for the drug. All we had to pay for is the administration of the drug. That’s a huge consideration.
We talked about CLL not being the most common cancer. We talked about medical research being expensive. Being able to pay for the medicine is a really important consideration. Sometimes a clinical trial is a great way to sidestep a huge chunk of that expense.
Jeff adopted Leuk, who helps keep him company.
What is the human experience of a clinical trial?
I thought it was going to be very lab ratty, even though I knew up [in my head] that I wasn’t going to be one. In [my heart] I was still scared. I did everything in what’s called the Ambulatory Treatment Center at Anderson. I would show up on a very regular basis in a room that was slightly larger than my walk-in closet and get plugged in. I would get my IV going, and we’d get all the pre-meds and all that stuff.
The first time around was a harrowing experience because they kind of couched what would happen. They said, “You should expect your first treatment to go about 8 hours, because your body has to get used to this stuff. There’s going to be some adverse reactions. When those happen, we have to stop what we’re doing, treat your reaction and then start all over again.”
Yeah, 8 hours turned into like 23, and I exhibited most of the adverse reactions to the treatment that were on the list from all that informed consent. It’s very disturbing to wake up out of a Benadryl-induced stupor to have your wife saying, “You’re a tomato,” and you’re solid red. Now you’ve got spots, and now this, and now that.
All that happened, but they treated me like royalty. At no point did I feel like I was in danger. I was getting the best of care. It got to the point where I could drive myself to the Ambulatory Treatment Center. I could get plugged in by myself. I could get the treatment. I could get the saline flush, and I could drive myself out. It became routine.
Jeff during the clinical trial he was a part of.
I was thinking to myself, “Well, even if this doesn’t work, they’re going to find out what didn’t work. Those are more data points. It’s not hurting me, and I stand a really good chance, according to my doctor, of getting a complete remission. Let’s stick with this.”
I did, and amazingly, I did achieve complete remission. I got the coveted MRD, minimal residual disease negative, for 6.5 years without having to go through traditional chemo. That was, I believe, worth the price of admission.
Reaching remission
Everybody was learning along the way. I’ll circle back to earlier when we talked about me being the compliant patient. Of course, as part of the clinical trial, they said, “Would you mind giving up all these additional tissue and blood samples during the trial so we can check this, that and the other thing?” Of course, I said yes.
Did you know if this was a blinded study?
In this clinical trial, everyone who was participating in the trial was receiving the medicine. They were not receiving standard of care. It was a fairly down-the-line clinical trial. Everybody was going to get the medicine. We need to see how different karyotypes react to the treatment and at what treatment level.
Meaning dose?
Dosage response. Is it a partial remission? Is it a complete remission? Is it MRD negative?
A few minutes ago, I was bragging [about] 6.5 years of MRD negative. I probably am not supposed to know that was one of the best responses in the clinical trial, but it was. And 10 years later, it doesn’t even bear asking why that happened, because we’ve moved past that already. We’ve already got so many cool new drugs.
The folks at Anderson were plotting out that bell curve and going, “Okay, Jeff is trisomy 12 mutated [and] all these combinations. He got 6.5 years. This person was this type; they got 1 year. This person [had] no response at all.”
All that information is important because they were studying a treatment mode that was far less toxic than the standard of care. FCR is a combination of chemotherapy and monoclonal antibodies. What I did was exclusively monoclonal antibodies, because somebody said, “If you’ve got a high expression of this CD20 marker on your cells, this stands a really good chance of knocking that sucker out.” It did for me, so great on the data point.
Editor’s Note: In the clinical trial, Jeff received an IV of ofatumumab.
Reflections
Using humor to deal with cancer
I have this bright red shirt with white letters, and on the front of it, it says, “Sarcasm. It’s how I hug.” My family knows that that is true. If I can’t find something to laugh at, you know things have gone really, really bad. I am going to find something to smile [at]. I am going to find something to laugh at. I am going to find something to dial down the tension. Otherwise, the oppression just gets to be too much.
Sometimes the humor is inappropriate. I will admit that right now. I can remember the word choice that I used when my daughter came into the Ambulatory Treatment Center with a bag full of Chick-Fil-A nuggets. “Honey, you can’t have those here.” That’s the paraphrase. I gave her the full-on of why having the fried chicken smell where people were receiving treatment is not a good idea. I may not have used the best choice of words, but we did laugh. So there’s that.
Making life changes
After I was pronounced MRD negative, complete remission, I was like, “Huh. I got my life back.” I kind of realized there was a quid pro quo that was expected at this point. I had gone through an awful lot. I had done an awful lot.
I’ve got a reset button that got pressed. What am I going to do with it? For the first time in my life, I decided perhaps it’s time to start taking better care of my body. I have been thin and relatively fit for most of my life, despite my family history of heart disease and all that happy stuff.
I started exercising. My wife had been a wonderful care partner throughout my treatment, the diagnosis and everything leading up to MRD negative. But she didn’t take very good care of herself while she was doing this, and she got big. She got very big. For someone who’s 5’4″ and that big, it was not healthy.
I got to MRD negative. I turned around, and (of course, with a bit of sarcasm) I said, “We can only have one health care crisis in this house at a time. Mine’s done. Let’s work on you.” My wife went through a very awesome program at a Houston health care center, and she lost over 75 pounds. She’s kept it off this entire time, but we had to make changes. We made changes in the way we ate and how much we ate.
Going back on watch and wait
Since she was exercising, I started exercising. Being a Type A personality, a little bit OCD, walking around the block once or twice turned into 5Ks, turned into 10Ks, turned into half marathons, turned into a full marathon. It was pretty cool. My mindset was, “I have to do something to make sure that what I got is not squandered.” I did that, and I kept at it.
After a while, I noticed that the fatigue was creeping back in. I noticed that the “allergies” weren’t quite allergies, because there wasn’t any oak pollen in the air. There wasn’t any tree pollen going on. There wasn’t the typical Houston-area mold going on. It was my body going, “Hey, there’s a problem.”
‘Go enjoy all the stuff you need to do to smile. Everything in moderation, including moderation.’
Jeff’s Doctor
I had that appointment at Anderson, and they did the blood work. My doctor came in, and he had that look on his face. I knew what that look meant. My habit of always giving my doctor a bottle of red wine every time he gave me good news was coming to an end, because he was going to tell me that I was in relapse.
Zoe, Jeff’s daughter, wearing her grandma’s wedding rehearsal dress.
I was, and it was okay. I really wasn’t prepared for him to say, “And we’re back in watch and wait,” because that’s exactly what the program was. In my mind, watch and wait was a one-time thing. It wasn’t something that had the potential to be multiple [times].
I was like, “Wait, we’re doing watch and wait again?”
He said, “Your blood work’s not great, but your symptom load’s not horrible. So let’s wait. Let’s see how it progresses.”
Has it been hard to get back into that state of watch and wait?
It’s been easier this time than it was the first time, because I know what this means. I have a different doctor at Anderson because my doctor retired. He was entitled to retire. He’d been doing this for a long time. My new doctor had a wonderful way of explaining watch and wait in a way that I hadn’t heard of before.
He said, “Look. Think of it this way. At MD Anderson, our job is to keep you alive, period. The longer we keep you alive, the more time we have to develop more medicine, better medicine, less toxic medicine. I’ve got some really good stuff in my pocket right now that I can treat you with now, but you don’t really need it now. If we push this out another 6 months, year, 2 years or 3 years, just think of what we’re going to have in store for you.”
I’m good with that. I know what the combination would be if I were to need treatment right now. I also now know some of the candidates for what the treatment might be 6 months from now or a year from now.
Staying healthy while accepting limits
Can I go drop off my briefcase, head out the door and knock out a half marathon right now [while] speed walking? No, I’m going to have to work up to that.
I don’t have as much gas in the tank, but I still speed walk every dang morning. I still do my sit ups. I still even play around with dumbbells. For the love of all that’s holy — my daughters have me eating oatmeal and chia seeds with fruit in the morning. I’m putting in the effort. The oatmeal is not really that bad. It’s just weird. I’m putting in the effort, and I’m still enjoying everything that I do.
Yeah, I’m in watch and wait, but the oppression is not as heavy as it was, because I’ve got an understanding of what’s going on.
Living life with moderation
When I first started seeing the folks in Anderson, I felt the need to do this confessional thing.
“So, Doc, you need to understand, I do enjoy the occasional cigar. I smoke a briar pipe from time to time. Is that going to be a problem?”
“How often do you smoke, Jeff?”
“Couple of times a month.”
“Not worried about that.”
“All right, Doc, you need to understand, every night I have a whiskey or 2.”
Jeff is a whiskey lover and has tried most of the back bar at his local favorite
“Really? What kind of whiskey do you drink?” I had to name it off. He said, “When was the last time you were drunk?”
“1992.”
He said, “I think we’re good.” I opened my mouth again, and he was like, “Stop. I’m not here to make you miserable. I am here to help you live a great life. So go enjoy the whiskey. Go enjoy the bowl of ice cream. Go enjoy all the stuff you need to do to smile. Everything in moderation, including moderation.”
Now, I’m a dozen-plus years into it. I’ll share a little secret with you: I still have that whiskey every night, except it’s a much higher quality whiskey. Because why not? Why not? If I have that whiskey and pretend to watch something on TV, and I have fallen asleep and gone off that cliff at 8:30 in the evening, I don’t care. I’m up at 4:30 in the morning anyway, getting my exercise in. I still got 8 hours of sleep in. Who cares when it happens? Watch and wait’s not fun, but it’s not as horrible as it was the first time around.
What is the biggest takeaway you want people to remember?
I think the most important message that I can deliver to anyone who’s newly diagnosed with CLL is, “Get the right specialist on your team,” because doing that will allow you to get in the mindset of enjoying your life. Being diagnosed with cancer is horrible. It sucks all the air out of the room.
We have learned so much in 12 years about treating CLL. I am not going to shy away from the fact that there are some people who are newly diagnosed with CLL that are not going to have good outcomes. That’s still something that we deal with. But the truth is that for the overwhelming majority of people who’ve been diagnosed with CLL, some of you may never need treatment. And those of you who do need treatment are probably going to have a fantastic response from it and have the opportunity to live a great life.
Since that’s going to happen, from a Type A personality, make a list. What’s all the stuff you want to do? What’s all the good stuff that you want to do? Put it down on paper and keep your promises to yourself. Go live a great life, because it absolutely is possible. The fact that all these medical professionals are now using the C-word (cure)? Cool for us.
1st symptoms: Tightness, lumps in left side of neck, severe pain in left shoulder, enlarged spleen Treatment (CLL): 6 cycles of EPOCH, clinical trial for DuoHexabody-CD37
Michele was diagnosed with chronic lymphocytic leukemia (CLL), a blood cancer that is the most common form of adult leukemia. Read on to learn about her journey through diagnosis, watch and wait, clinical trial treatment, relapse and living life as a chronic cancer patient to the fullest.
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
1st Symptoms and CLL Diagnosis
Experience outside of CLL
Life before CLL
Before CLL, I was very career oriented and family oriented. I was that kind of woman who had to do everything super well. I was A++ at everything. I’d started out in broadcast journalism on TV news before I segued into the corporate world — or as we say in the business, the dark side of journalism.
I was the global chief of communications for a $9 billion publicly traded company, and it was a really cool job, very stressful, with long, long hours. When I say long hours, I mean I slept a few hours a night, seven days a week, because of time zones and the media. It was a great job until I was diagnosed.
What about your life now? What are your hobbies?
I’m happily married. I have a terrific husband, who is so supportive of everything, of things that I do with friends, things that I do for work, my patient advocacy. Also, he is the best care partner there is.
In addition to that, I’ve always been a fitness nut and into exercising. I used to go to the gym before COVID. Now I do what I can at home. I do yoga now because I’ve learned that’s really good for you and to calm the mind.
I have Gabby, who is our chocolate lab. She’s my buddy, and we seem to do everything together. She has been also a great support to me during all of everything that I go through with cancer and outside of cancer.
Diagnosis
First symptoms
I thought I was a healthy person. I always had been very healthy and active. My God, my schedule alone! I figured you had to be a healthy person to be able to keep the hours I did and to always be traveling everywhere for work.
I was on planes 1 to 2 times a week, and they could be going anywhere in the country or in the world. Healthy eating was really big for me as well. I started having these weird things happen, each one in itself didn’t seem like a big deal.
I talk about these so that other patients, when they hear this, will know that these are things they should watch for if they have CLL. It’s things that if you look back, you’re like, “Oh yeah, that happened to me.” It took me a while to even realize that these pieces were there.
I figured you had to be a healthy person to be able to keep the hours I did and to always be traveling everywhere for work.
Ongoing infection
In November of 2010, I had a flu or something that led to chest congestion and a sinus infection from hell. I just couldn’t get better. I went to an ENT, and they didn’t do any blood work or anything. They just treated the symptoms because they had no clue that anything else could be wrong.
That lasted a really long time. I was traveling. Each of these times I had just traveled out of the country. Long flights, long hours. Not eating as healthy as I’m used to, not having time to exercise.
Scalp infection and bumps
A few months later, something else happened. I had this weird scalp infection, but it looked like I had burned myself with my flat iron. I’m just like, “Stupid, clumsy me, or maybe this happened at the hair salon when I had my hair cut or colored.”
I had these huge bumps at the base of my skull. I had no clue at that time that lymph nodes were everywhere and that those were lymph nodes. Then I went to an emergency clinic because it was just so bad, and my husband thought that maybe someone should see it since it really looked pretty gross.
I went there, and they gave me a shot of some kind of antibiotic. Then I went to my dermatologist, and they again treated what that was.
Then a few other times, I just kept getting sick. I would catch a cold, and it wouldn’t go away. I would get a flu or sinus infection. It just lasted forever. These are all really common things now that I know about CLL. These are really common things and signs for someone to look at and put all together that you have something.
Elevated white blood counts
Your white blood count, the highest end of the range should be pretty much in the mid to high 8000s. Mine was maybe 11 consistently, and then 14. That’s what flagged my primary care physician (PCP).
Plus, when you see your PCP, it’s not that often. He wanted me to come back in maybe six months. Of course, I delayed that because of work and being too busy. I’d kind of forgotten. It was like, “I don’t even know what that means. What’s the big deal?”
Then when I went back, it was still elevated. That’s when he suggested I see a hematologist, which in my mind was just a hematologist. I didn’t even connect hematologist and oncologist.
I didn’t return his calls for a long time until my assistant sat on my desk and said, “I’m not leaving until you call your doctor. This is the fourth message. You’ve got to call.”
Still, it didn’t dawn on me because I didn’t think about it. I didn’t take the time to think about it. I was so busy with everything. Why is he calling me? I didn’t even think there could be anything wrong.
This is something you shouldn’t do. I have since learned, and I learned the hard way. He was very calm about it. I have to give him credit. “I don’t want you to be alarmed. Your white blood count’s a little elevated. Again, I really would love you to go get this tested again and see a hematologist.'”
In my mind, I was like, “Yeah, someday I’ll go do that.”
Finding the hematologist
My PCP was a bit north of where I worked, and he knew how busy I was. He said, “I don’t know anybody in Miami, but see if you know anybody who can make a reference or recommendation for you.”
Someone I knew who was a nurse recommended this particular doctor. I walked into the University of Miami Sylvester Cancer Center, and it still didn’t dawn on me what I was being tested for.
I went through tests and questions, not knowing, having no clue. Nobody told me why I was being tested. Maybe he assumed my PCP told me, and my PCP maybe figured he told me.
I had no clue, and I’m like, “Why is he asking me this? Why are they taking so many tubes of blood? And why is he telling me, ‘I’m sure you’re fine’?”
I honestly had no clue. I was so busy. I registered hat it was a cancer institute at University of Miami Medical Center, but I never, ever put two and two together that that could be me.
Testing after blood tests
Then he did a verbal really long list of questions for family history. My parents were very healthy all their lives and living long lives. It’s not like they were young and passing away.
Again, I was just like, “This is taking so long. I have to get back to work.” This is how crazed about work I was. I’m like, “I have a deadline. I have a reporter waiting back at the office. I’ve got to get back to the office.”
I look back, and I realized that that’s probably not the best way to be in life. You really have to think about your health at times. The other thing is, though, it protected me in a way from knowing how grave this could be.
When I walked in there, I didn’t think that could be me.
I see people hooked up to IVs as I’m walking through. I see cancer patients and in wheelchairs, sadly without hair. When I walked in there, I didn’t think that could be me. It didn’t even register. If I had had time, perhaps I would have been a basket case, because it’s shocking to think that that’s you. That’s your future.
Time it took to get results
It took a while to get any kind of call. I put it out of my mind. I’m like, “Okay, whatever. I guess I’ll hear something if anything’s bad.” It took a couple of weeks, and then I heard from someone in the doctor’s office that everything was fine. That’s great. I’m thinking, “Of course it’s great. I’m healthy.”
I got a call a week later, and she said, “The doctor wants to go over your test results.”
I said, “I thought you said everything was fine.”
“Well, he just wants to meet with you.”
I’m like, “This is really nice,” but really I’m thinking, “My schedule is so packed.”
She said, “No, really, he really just wants to go over these things.” Again, you would think that it would dawn on me and I’d be petrified, but I was not.
The CLL diagnosis
I was just, as the English would say, gobsmacked. I sat down, and I had no clue what he’s going to say. He came in and said, “Well, you have the C-word.”
This is how out of tune I was. I’m like, “What is he talking about?” It wasn’t top of the mind awareness what the C-word was, because again, I didn’t know I was being tested for the C-word. Then I’m like, “Oh no, that C-word.”
He blurted out, “You have CLL, another C-word, chronic lymphocytic leukemia.” He said it so fast, and I was in shock. I was dumbfounded. What did he just say to me?
Of course, that changed my life right there. Then I heard “leukemia.” That’s all I heard. I’m like, “This doesn’t sound good.”
He said, “I’ll see you in four months,” and he went to leave.
I said, “Wait.” Of course, having my journalism training, I always have a million questions. “Wait, wait? Shouldn’t we get rid of this now?” The things that we would normally think that are logical for cancer.
He’s like, “No, you don’t have to be treated. You may never have to be treated.”
This is just not making sense. I’m in shock, and I’m like, “What do you mean? Well, what am I supposed to do?”
He said, “Just go on. Make sure you wear a mask when you’re in public.” The cruise industry is big in South Florida. He said, “Wear a surgical mask when you’re on a ship.”
Meanwhile, I’m in the cruise industry, and I’m leading press conferences. I’m like, “This is not a good visual.” This is before COVID times. We’re talking back in 2012, and that would not be a very good visual. That’s all he had for me.
I didn’t understand. I needed more information. He could not wait to leave the room. I asked, “Do you have any literature on this? How about on the hospital’s website? Is there somewhere you can suggest for me to look? For me to research this?”
He had nothing. And that was it. Then he put his hand on my shirt. He said, “Don’t worry, you’ll be okay.” He was an older doctor. He did get it right on my diagnosis, but when I walked out, I just knew that I probably wouldn’t go back there.
Switching doctors
I knew something wasn’t right. For me, that wasn’t my cup of tea to be treated that way and also to never be told what it was I was being tested for. I was really in shock, as well.
He couldn’t even say the word. The other thing he said was, “You have the C-word, but it’s the best one you can have.” None of this is making sense in my brain.
When that clicked, I’m like, “How can that be best of anything? It’s cancer.” I’ve heard this from other patients. They say they’re told that it’s the best one you can have, and that just offends everyone.
Advice for doctors from the patient perspective
Maybe you shouldn’t say it’s the best cancer anymore. Don’t say it’s the “C-word.” This could be a style between doctors and not to get patients overly worried, but if you’re testing someone, maybe you should let them know what you’re testing for and list a few things that it could be.
Maybe he didn’t know which kind of blood cancer. Maybe this was my PCP who should have told me, but you would think they had an idea if I was sent to a hematologist oncologist.
Let me know, or put it in a list of various things it could be. You don’t want to overly worry me in case it’s nothing. That, again, could be a generational thing between the doctor.
Emotions after the doctor left the room
I was just like the jilted girlfriend holding on at the last moment, like, “Please don’t leave me.” Of course, now I can look back and joke about it because we have self deprecation, having cancer and having been through these horrible things.
That was a very low day in my life, and I proceeded to make some pretty stupid decisions after. The other thing is I drove myself, and it wasn’t around the corner from where I work. That shouldn’t happen.
Processing the diagnosis
I went back to work and acted like nothing happened, and I went home and crawled up in a ball. Before I did that, I burned the hospital bracelet in my bathroom like it didn’t happen. I had water running so I wouldn’t set off. the smoke detectors. This is me. I’m always thinking of everything.
I burned the hospital bracelet. In my bathroom. Like it didn’t happen.
I burned it because I was so upset. Maybe it didn’t happen if I burned it? I don’t know. Then I convinced myself maybe this was wrong. Maybe they had somebody else’s blood test results.
I tell my patients now, “Do not do this.” I curled up in the fetal position after I went on Google and did a search, and it said I’d be dead.
Some had said three to five years; some said five to eight years. That was very old information that I found, or speculative. I hadn’t yet learned that first night what the credible sites would be and how they’re credible. At that time, 2012, there wasn’t as much available on the internet about our various diseases.
Telling family
I called my sister, I told her — wait till you hear this one — I was going to leave my husband. We had not even been married two years, and it wasn’t fair for him to have another wife with cancer.
His first wife had cancer, and she had passed. I just couldn’t do that to him. She talked sense into me. She was like, “You need to hang up with me and call him right now and tell him what’s wrong.” I was like, “I just can’t do this to him and the kids.”
His children became my children, and I just didn’t want them all to go through this again. It was really hard on so many levels. But I 911’ed him when I hung up with her after she talked sense into me. I don’t even know how this was for her.
It was too late for him to take a plane that night, so he was on the first plane in the morning. He was in Boston. I was in Miami. That’s when it really hit, when you’re together and share it. I don’t know how he even got to the airport himself and how he got on that plane.
Then we figured out what I was going to do, and it was basically I had to leave. I left Miami and left everything: parted with work, my home down there, my life down there, my friends. I had some really terrific friends because I had been down there about seven years for my career. But what’s more important? Health and family.
My mom was up in Massachusetts, as well. I didn’t even tell my mother for a long time because I didn’t want her to worry, and I knew I wasn’t going to be in treatment.
“If I’m not in treatment, just what is the point?” I thought. I have no clue what to even tell people. I have it. So what?
Getting a second opinion
I had a second opinion within six weeks at Dana-Farber with the head of the CLL department. I didn’t even know that there was such a thing as a specialty in CLL. and that was something else I wish that the doctor had mentioned in Miami.
I was just so lucky and blessed that where we lived in Boston, we’d be seven miles away. There was a CLL specialist, an entire department, so I started seeing her.
I was hoping that those tests were wrong. I really did hold on to that hope in the back of my mind. I knew there was something. If I thought about all those things that I had mentioned earlier, there was something.
I came back to Boston full time to be with family and try to figure out what I was going to do then. I realized watch and wait is a real thing and that yes, I can still work.
Worrying about reactions
It affects everyone in your family circle. I wasn’t thinking straight. I did worry about them, and I just didn’t think that it was — “fair” is probably the wrong word, because none of it is fair right to any of us.
Life during watch and wait
Watch and wait’s also called “active surveillance,” and it exists in some other things as well. There’s another blood cancer where it’s called a few different things as well. What patients call it is “wait and worry” or “watch and worry.”
It’s somewhat inhumane when you think about it. You’re basically waiting and watching your disease worsen until it would be so bad that you need treatment versus doing it the way you logically would with a different type of cancer that we have all heard about. You know that you treat early, get rid of it and you have better chances.
There are some patients who never need treatment, so that watch and wait could be forever for them.
Michele
Not everyone gets worse, and CLL is such an odd disease that not everyone needs to be treated. There are some patients who never need treatment, so that watch and wait could be forever for them.
Until they test certain things like your genetic factors, prognostic indicators, they don’t know how you will be and how your disease will progress or not. That’s one factor that they look at.
From the time of diagnosis, I do suspect I had CLL longer before from different factors, but from diagnosis they say it’s generally an average of two and a half years to treatment, which is just about what it was for me.
Learning about CLL
I’ve heard this from so many other patients, and I just want to tell you, use that time of watch and wait to educate yourself on CLL because it helps. For one, you do need treatment if you ever need treatment.
I was diagnosed ten years ago and I’m here, and there’s just so much hope for patients. It also helps prepare you for what’s going to happen. For me, the more I know, the better it is for me because then I know more of the facts as opposed to me wondering.
That’s when my mind kind of goes like to places it shouldn’t go. Once I could understand facts, it really helped to calm me down. That’s really why I started reporting on CLL for other patients to help them to demystify what it’s all about.
Living with chronic disease
Waiting for signs
There is a percentage of patients that do need treatment immediately, and they don’t like that either, as opposed to being able to watch and wait. For the watch and wait, every time you go you wonder, “Will this be the appointment that they tell me?”
You start to learn, and you also open communications with your doctor. “When will you know it’s time? Can you give me an idea how long in your experience for someone like me it’ll be?”
Again, we are so different, all of us. It’s tough because there are so many factors. For my white blood count, it was a certain amount. It was that, and it was lymph node burden. It was spleen size and all sorts of things.
I have a friend whose white blood count is at 240,000, but it’s not time for treatment for her due to other factors in her blood work and in the exams that you get. For me, it was totally different.
That’s why it’s so important to make sure you do keep your appointments. For me, it was every three months and then every two months as I got closer to treatment, and then it was just time.
For a lot of the patients I’ve spoken to, it really does vary. One of the things that helps determine this is something called a FISH test. That will show your genetic markers, your prognostic indicators, and they also do something called a flow cytometry.
I know there’s a good number of patients who have never had these done, and they’re not in treatment yet. I do suggest that you ask for those because it does help for you to know what those are.
For me, it was a combination. My platelets started going low below range. My white blood count started doubling, although it never even got as high as this other person I’m speaking of. I know other patients that have gotten even higher white blood counts and still aren’t in treatment.
It was my lymph nodes, and they can tell that by physical examination. I mean, you could see my lymph nodes. They were all swollen. You could see them here. It wasn’t only my lymph nodes; it was a combination of platelets and other counts they look at. They want to look at your hemoglobin to see how that’s doing.
All of that put together. It takes a specialist really to put all those all these puzzle pieces together. That then is the point. For someone else, it might be that their white blood count gets so high and their platelets tank maybe lower than mine did, and maybe their spleen is really swollen, so it’s time for them.
There are all different indicators there that help. I know someone else who their white blood count went down, but they had CLL and some other factors happen. It’s just that varied for patients, depending on what it is about their disease for time for treatment. I also encourage second opinions.
CLL Treatment and Clinical Trial
Video
What was the catalyst for you to go into treatment?
The catalyst for me to start CLL treatment after having been on watch and wait for a little over two and a half years was that my white blood count had doubled a few times in values between appointments. Also, my lymph nodes had grown to a large size that was palpable for my CLL specialist to find. My spleen was enlarged.
These are all signs. Other blood counts also had either gone up or down to levels that were not within range anymore. All these things that point to, “It’s time for treatment.”
Clinical trial
I was very interested in a clinical trial because at that time in 2015 there was only one. Things have just changed. It’s crazy, and it blows my mind when I think how much things have changed in six years.
There was pretty much the gold standard of treatment, which was FCR. It is by infusion, and it’s basically fludarabine, cyclophosphamide and Rituxan.
There was a trial open that I was offered. It was for young — and I’m young for CLL — and fit patients. Here I was, in the gym almost every day. At that time, actually, I had started running. I fit the criteria.
At the time, either they had said it could be curative or to put me into full remission and keep me there. I was like, “Yeah, sign me up.”
What I didn’t realize when I was signing up is that it was with ibrutinib, an oral treatment, which became the next gold standard of treatment. I was on full strength of both simultaneously for six months, and then I just continued on with the ibrutinib, the oral BTK inhibitor, which many CLL patients out there could be on or had been on or will be on.
Within a couple of weeks, almost overnight, I felt like my lymph nodes had melted.
I had had what they call night sweats, which are like hot flashes, and I had them morning, noon and night. I was just a furnace. I froze everyone out of my house. We shared a summer home with another couple, and I froze them out of that house. They would push up the temperature. I’d be like, “I can’t. I’m so hot.”
I was on two full-strength treatments simultaneously for six months. Most patients do one or the other, and yet all of this was happening to my body at once.
That is another sign that it’s worsening. I also had had another sinus infection, which was the worst ever. I thought I had experienced the worse ever. These are all signs that they saw that my immune system was deteriorating due to my disease that was progressing. These are things that do happen to CLL, not all CLL patients, but some.
It was just amazing. The night sweats stopped within a few weeks. Just so much of what had happened to me seemed to be getting better. Then I started with chemotherapy side effects that a lot of people have. It’s a bit of a trade-off, but I knew that there was a light at the end of the tunnel for the first six months.
Increasing fatigue
My fatigue increased. I also had fatigue with CLL. It got progressively worse and worse the closer I got to time for treatment. Fatigue is another big factor that I hadn’t mentioned for most patients. By the time I started treatment, I was taking naps every day, which is like against my religion.
I always think that’s what you do when you get old, but I had to give into it. Then when I started treatment, I absolutely eventually had to nap earlier in the day because infusion chemo is cumulative. I never thought about it at the time, but I was on two full-strength treatments simultaneously for six months. Most patients do one or the other, and yet all of this was happening to my body at once.
Ibrutinib and FCR regimen
With the ibrutinib, you take two pills daily — no stops, it’s just continuous treatment — and concurrently the FCR. For FCR, you would be at the hospital as an outpatient for four days a month. It was by infusion, and that was for six months. It wasn’t a full day once they figured out the speed of your chemo, of your drip. In the beginning, it took much longer. By the end, I was zipping through in four hours.
Dealing with the side effects
I never stopped going to the gym and working out. I hired a personal trainer because I didn’t trust that I would be able to judge what I could and couldn’t do, and I still wanted to be pushed a bit, but safely.
I made sure I hired one that had a great background in physical therapy and physicality. I did that three days a week and did yoga another day. Every week except my infusion week, I did this.
For me, that was one way also to keep control of my body. I felt like it was controlling me or others were controlling it. This was my way to be able to control something.
Her name is Amanda Kelsey. She was able to judge my energy level somehow. She was able to read my energy levels and tailor my workouts without my realizing she was doing this. One day I asked her, “How did you know I was tired today?” She would know; that was great.
There are studies that show that you have less side effects if you keep active, if you move and have some kind of movement during treatment.
I had neuropathy in my feet at times. Not constantly, but at times it would hurt to walk. For those of you who follow Kicking Cancer in Heels, I wasn’t able to wear my highest of heels in those days because it hurt too much.
It’s happening again now that I’m back on treatment, but I had a hard time holding on to things. I remember picking up a jar of spaghetti sauce in the supermarket, and it fell out of my hands. Of all things to fall! I was so embarrassed. It would hurt to hold hand weights, and I didn’t have strength to grip.
These are pretty common with many chemotherapies. They’re not fun ones, but there are worse. My fatigue, though, is really profound and one of the worst of my symptoms, and I wasn’t able to go at my normal pace or even half my normal pace.
There were others, as well, but at the beginning I wasn’t sure what it was from. Was it FCR? Was it ibrutinib?
Dermal reactions
I also had a lot of dermal reactions. I started breaking out in hives a lot. Redness, red, splotchy things on my face. I had to start seeing a dermatologist, and I learned it’s better to go to one that specializes in oncology because they know what to do.
If you can find one, there are only 51 or 52 institutions in the U.S. that have them. I didn’t know that. I was just, again, so lucky to be going to a cancer center. Ask them if maybe they know of them or can refer to one that’s local for you.
It was a game changer. All she had to do was look and, in a second, know what it was. From what I understand, various chemotherapies do this. It’s not just the ones for CLL. They do know what to do if it’s somebody who understands the effects of oncology drugs and your skin.
Treating dermal reactions
Also, I learned how to cope with each of the different things that happened. A lot of strange things happened. It would break my heart when I’d see online chat rooms on Facebook and patients would say, “I’m going off my treatment because of my skin side effects.”
I would feel so badly and and try to answer. I’ve done reports on all the different things that you can use. Sometimes it’s just a particular ointment. Sometimes for hives Benadryl is the best, but that knocks me out. But at least they go away. I’ve been trying to use both.
Someone had said a couple of antihistamines can help. There are different ways, but there seems to be something for almost everything on these particular side effects for that. None of those were horrible things to do. It wasn’t like you had to do anything drastic. Again, being your own patient advocate, pushing, asking, “What can I do? This isn’t working for me. Can I see someone? What can I have that can help me?”
Until March of 2016, it was everything. Then at that point, it was just ibrutinib, and ibrutinib you stay on indefinitely. By the way, I so encourage people to go in a phase 2 or later clinical trial because that means the dosage has already been determined. You don’t have to worry about that part of the trial, if you have choices.
Some patients have already gone through all kinds of treatments. This would not be a first-time patient. They do sometimes go on a phase 1. For those of you who have never been in treatment, phase 2 or later is like getting tomorrow’s treatment today.
For me, ibrutinib had been approved for relapsed patients, but it hadn’t been approved for those who have never been treated. I couldn’t have gotten that drug otherwise if I wasn’t on the trial. FCR, on the other hand, is not used that frequently. This trial that I was on, now the results are in after all these years.
Unfortunately, I’m one of only a few patients — and I want to say it was 89 percent of the patients went into the Holy Grail of CLL, which is called uMRD, which is undetectable minimal residual disease. Of course, I had to be one of the few holdouts. I almost reached it. Almost very, very close. It put me into a very deep remission, a deeper remission than if I had just been on the ibrutinib.
I stayed on the ibrutinib quite a while, about three-and-a-half or four years, until my adverse events or side effects became so untenable. The fatigue was really one of the worst because I was working, but I couldn’t work at full speed, nor could I really work full time yet as long as I was on it. Because of that, I took a bit of a drug holiday and stayed in my partial remission until I relapsed last year.
Having both FCR and ibrutinib and that I was in the first cohort — they kept telling me the fatigue was from treatment in the beginning. After a year after treatment and I was still tired, then they started trying to figure it out. It’s not like there were other options at the time, and then other options started happening. The drug was working beautifully, other than one lymph node being bigger than it should be.
Bone marrow biopsies on a trial are done more frequently than otherwise. Some patients never even have to undergo a bone marrow biopsy. In the first year of the trial, every three months I had to have CAT scans and a bone marrow biopsy. The bone marrow biopsy is more precise than a blood test to find out what percentage of your bone marrow is infiltrated by your disease.
When I went into treatment, I was at 91 percent infiltration by my CLL, and when I heard that I was like, “Oh crap, I really should be on treatment.”
You want to be on treatment in the beginning, and then after you get used to not being on it, it’s like, “Treatment? Oh my gosh, I have to go on treatment now?”
It’s the irony of this. In other ways, I was so happy to be on treatment because for me, I was confident I was getting better versus getting worse. That is a turning point.
I think also when patients have been on treatment, they know what it’s like. They don’t get as nervous perhaps for the next one. You still get nervous, but you know what it’s like, and you know that you’re getting better.
Going off treatment
Finally, I did say that it was really affecting my quality of life, and that’s when my doctor started suggesting I go off of it. I felt so miserable, but she wanted me to go off. I was afraid to go off because I knew I was staying, as odd as it sounds, healthier on it.
We actually had a tug of war with the bag with the ibrutinib in it. I pulled it towards me. She pulled it towards her. I pulled it to me.
I’m like, “But I have to stay on.
She’s like, “No, you’ll be okay.”
Finally, I let her be the victor because it honestly was great being off treatment. I was able to find out that, yes, I still had energy. That was the other thing, trying to explain to the doctor the real me that she had never met. Well, she met in the beginning when I was working.
Here I am, back to work, able to work tons of hours and still do all sorts of other things. All they see is you as a patient. You have to explain really how you are. I was able to prove to myself — which I needed to — that yes, once again I could get back to having a lot of energy.
I’m glad I was able to do it. It was wonderful seeing that I am still the person I thought I was, and I could still have energy and that age hasn’t taken over. Things didn’t change from having been on treatment, because that’s the other thing you don’t know. Have I changed? Has it changed me?
It actually ended up being two years before it started being noted as being progressing, but it wasn’t time for treatment again yet. You have to wait until it gets worse. It presented itself a little differently this time, and it became more aggressive toward the last two months before it was time to go back on treatment.
I wasn’t happy that I had to go back on treatment, but I did know that I would because it is a chronic disease and the majority of patients do. I was hoping I would have gotten a little longer without treatment, but that didn’t happen, especially with COVID.
When I stopped treatment, it was maybe only ten months before people went into lockdown with COVID. So I just kept thinking, oh gosh, when am I going to be able to live life? That’s another reason why I wish it had lasted longer but I’m back on.
Choosing between treatment options
I didn’t know which treatment to go on, so I once again, got a second opinion and a third opinion this time. I am really happy I did because the good news is there are so many choices right now to go on, which was so different than when I first went on treatment when there were hardly any choices.
There’s no cure yet, but a lot of the specialists say there will be a cure for us to look forward to.
There are so many choices that it was kind of hard to decide. Also, there were so many trials. I opted to go on the next generation of BTK inhibitors, something called acalabrutinib, otherwise known as Calquence.
I was waiting for a phase 2 of a particular trial that my doctor had suggested and that I had spoken to others about. By the way, the second opinion you get should really be from a CLL specialist. Even if you don’t see a specialist, I suggest you talk to one for a second opinion.
I am considering going on a trial in the future. The original one we thought of is no longer one that we’re looking at, because I am doing so well on the drug that I’m on. We may add in another drug potentially to put me into a deeper remission again, so that’s what’s next.
What is most important to you when deciding the path to take?
Every patient is different on what works for their lives or not. I was hoping to have finite treatment. That’s not as important to others. Some people are fine staying on indefinite treatment, and it’s easier for them really to just take a pill. It’s much more serious than just taking a pill like a vitamin.
I don’t want to minimize what it is, but their lifestyle versus having to worry about infusions or worrying about being overnight in the hospital for any particular treatment that you have to go through or from being monitored.
I really did want finite treatment, and that’s not what I have right now. I’m doing really well with the drug I’m on, which is wonderful. I would still love to have finite treatment. The things you have to look at is, “What’s right for you? What will work for you?” What works for me may not work for someone else.
Again, some of this has to do with how many times you’ve relapsed or if you’re new to treatment. It has to do with certain treatments. It depends on the things that we were talking about before, your prognostic indicators.
Those are like 11q, 17P, TP53, and IGHV mutated or unmutated. I don’t have the worst, but I don’t have what they call the best. I’m somewhere in between. I have two of those.
Then for some patients, one works better than the other. There are all these combinations of treatments on top of that, like endless combinations and endless trials, which is really wonderful for us. There’s no cure yet, but a lot of the specialists say there will be a cure for us to look forward to. I do hope for that.
Being on acalabrutinib
Ibrutinib, you take your pills once a day. Acalabrutinib, you take it twice a day, for me anyway. Different patients sometimes take less. There are sometimes side effects on this that go away. In the beginning, just like most patients, I had horrible headaches, but not all the time. They go away within a few weeks.
If you drink coffee, which I try not to later in the day, then it goes away. They know this now because the drug’s been around a while. You can also take Tylenol.
It has less side effects than the ibrutinib because it is a newer drug with less toxicity. I have only one other real side effect, and that is — we’re unsure if it’s neuropathy or joint pain — in my hands. That’s something yet to be determined, and that too could go away. I’m hoping for that.
Finding Purpose in Cancer
Video
How did you work through the identity shift of having cancer?
It is such a difficult thing, and it was one of my hardest challenges with the diagnosis and trying to figure out who I am. When no one else was home except our dog — I would talk to her because she was safe — I would just sit on the floor and cry and say, “What am I supposed to do with this? What is my purpose? I need to do something. I don’t know what my purpose is.”
One of my friends said to me two weeks after I was diagnosed, “What’s your new dream?” I’m like, “I don’t have any right now.” Then that sat with me. I have no dreams because I knew that I couldn’t go back to the schedule I kept in my career. Even if you’re healthy, you probably end up not healthy because you really should sleep, and you shouldn’t be working all those hours. I kept trying, so what is it?
Finding purpose again
It’s interesting that the day I started chemo is the day I started reporting from the infusion chair. I didn’t realize that was my purpose yet. I did it to help others and to demystify it.
I learned that actually made me feel better because even though I still didn’t realize it was the purpose, it gave me a purpose. It kind of gave me a job when I went to chemo and infusion. I didn’t really think about it as much. It was just like, “It’s my job here to report on what this feels like.” I was living in two worlds.
Once I started feeling better, I took on clients as a communications and PR consultant. I’d work with agencies for their clients, and I was doing my patient reporting. I started doing more and more in the patient influencer and advocate community.
When the first Wonder Woman movie came out, I saw it. I know this may sound silly, but Wonder Woman jumped into battle ahead of all of the troops — men, because it was World War Two in this movie — and she just went head on into battle with everything firing at her, and she used her cuffs to fight them off like my cuffs.
Wonder Woman and fighting cancer
I started using that for visualization for many things. I could never really get into meditating and visualizing different things in your body and it being disease free. Suddenly I had something to count on. It was in my brain. I was fighting off those cancer cells. My husband went on Etsy and got me each piece of the Wonder Woman costume uniform. He was in the military, so to him, it’s my uniform.
I have a real metal shield. We’re not talking plastic here. Swords and the cape, the whole thing, the crown. I’ve got it, and it really helps me fight off my cancer in my mind. Also, it’s given me the power to move forward in my patient advocacy and in fighting off my CLL. I know that I can be Wonder Woman and fight it off and be the victor and have the strength for that. I try to think of it now as going into battle against my disease.
What I’ve done won’t work for everyone because we are now immersed in the cancer world for work and ourselves. I’m able, probably through journalism training, to separate it.
When I’m doing the work, I am not the story. I’m not used to being the story. It’s so much easier to be the one asking the questions versus being the one giving the answers. I’m able to separate things out.
Support groups
There is a close woman support group that another woman and I co-founded called CLL Women Strong. I invite any of you out there to join that, or also there are other support groups out there for virtual meetings.
There’s AnCan, which is for all blood cancers. They are online. There are so many on Facebook. One is just called CLL Support Group. I co-administer that with another fabulous co-patient, Jeff Folloder. There are just so many out there. There are CLL/SLL women’s groups. Find one you identify with because you can post things and people will answer.
They’ll be there to support you. You need people who understand what you’re going through. Support groups didn’t exist when I was first diagnosed. It’s also really hard to find other women and other women who are diagnosed at a young age and going through this. Now those things do exist.
Everyone’s kind of growing with technology in this, but also you’ll find kindred spirits that understand and you can identify with, because your family isn’t the place to always go to for this. They’re not going to understand, but don’t let that get in your way of finding what’s right for you.
Bill’s Chronic Lymphocytic Leukemia with Richter’s Transformation Story
Interviewed by:
Stephanie Chuang
After an allergic reaction sent Bill to the ER, he noticed lumps in the left side of his neck. A series of tests revealed diffuse large B-cell lymphoma. Then he was in remission for 3 years before another ER visit for severe shoulder pain turned into another diagnosis: chronic lymphocytic leukemia (CLL) with Richter’s transformation.
Bill discusses how his diagnosis intersects with his original misdiagnosis, what it’s like being part of a clinical trial, hope for the future and the important of patient advocacy.
Explore his incredible story below. Thank you so much for sharing, Bill!
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
VIDEO: 1st Symptoms & Diagnosis
1st Symptoms and Diffuse Large B-Cell Lymphoma
Introduction: Tell us about yourself
I have been in vocational Christian ministry for most of my life. I’m a retired Anglican priest, and for the last 16 years I was the rector of St. Estimation Anglican Church here in Waxahachie, Texas.
What were your first symptoms?
I went to the ER with anaphylaxis. I swelled up like a toad and turned red. The therapy for that usually is some kind of steroids and antihistamines to kind of calm things down. I noticed when all the swelling in my face reduced, the left side of my neck seemed to be a little thicker than the right. I turned my head, and it would be tight.
I thought, “That’s weird.” We went to my general practitioner, a good friend for 30 years, and I said, “John, there’s something in there, I think.” He mashed around, and he said, “Yeah, you got something in there.”
Early on, I thought, ‘Okay, this could be something serious,’ and as the diagnoses proceeded, it was serious.
That led to an X-ray and then a CT, and the radiologist said, “Yeah, you’ve got some swollen lymph nodes in your left neck. You better check that out.” That started some diagnostic stuff — needle biopsies, finally an excisional biopsy — and the verdict came back: diffuse large B-cell lymphoma.
At what point did you realize it was serious?
My Christian faith helped a lot, obviously. I think actually it kind of snuck up on me. I’m one of these guys that wants to read all the radiologist reports before I talk to the doctor. The first one I read used the word “malignancy” at one point, and I thought, “Ah-ha, okay.”
I asked my good friend Dr. John, and he said, “Well, he thinks it’s a malignancy. We don’t know yet, but he sees a lot of it, and that’s what it looks like to him. That’s why he used the word.” But he said, “Let’s keep going.” Early on, I thought, “Okay, this could be something serious,” and as the diagnoses proceeded, it was serious.
Processing the Diagnosis
How did you get through the scanxiety waiting for the results?
Actually, I had my plate full of things to do. I had not retired from my work, and so there were things on that plate. I have 3 living daughters. At the time I had 5 grandchildren, 4 of them nearby, and there was plenty to do.
I wasn’t just sitting around twiddling my thumbs and worrying. I just kept on keeping on. I felt okay. I didn’t feel sick. I thought, “Okay, we’ll just wait and see what comes down the pipe and deal with it when it gets here.” It stood me in good stead to do that.
I kept my wife and children up to speed immediately, of course. We’ve got a pretty close-knit extended family, so everybody was on board, and they were concerned.
The local oncologist was fairly optimistic. He said, “We caught this very early, and it is a version of lymphoma that is quite responsive to therapy.” He said the cure rate is quite high for this type of lymphoma, and especially with catching it so early.
It was only in one spot. We had a PET scan, and that’s the only part that lit up. He was optimistic. He said, “The standard therapies we can do is basically 2. Statistically they’re the same as far as outcomes. You pick.” I did, and we did it, and it worked. Everything went into remission. We got our PET scan at the end of it.
Why did you choose the mix of chemo and radiation?
I assumed what everybody assumes about chemo: that it makes you sick. I don’t like to feel sick. I thought, “Okay, well, if indeed you can’t distinguish the outcomes statistically, I’ll take the less sicky one.” So I did 3 of the R-CHOP and 15 of the radiation, and it seemed to work just great.
What was the follow-up protocol after the cancer went into remission?
After that, he would see me every 6 months and physically examine me for evidence of swelling lymph nodes where he could palpate and where he expected things to show up, and nothing ever showed up.
The pain was excruciating. I’ve never had pain so severe in my life ever.
I think I had a PET scan about a year later. I’ve had so many of those. It started to run together, but there was just no evidence of the cancer for the next 3 years.
CLL Symptoms and Diagnosis
After 3 years of normalcy, what CLL symptoms sent you back to the ER?
The pain was excruciating. I’ve never had pain so severe in my life ever. I don’t know what is wrong with the ER people that when I showed up, they should have put me in a closet and closed the door because I was howling. I’m in a big waiting room full of people, and I’m just bellowing. I can’t help it.
They finally get me out into the place. They do an X-ray. Nothing. They can’t see anything unusual. They do a CT, and they’re starting to pump me full of morphine and finally get things calmed down.
If it was coming back for me, then okay. Lots of other people have been there and done that. It looks like it’s my turn to be there and do that.
The doctor came back after a bit with the radiologist report. He said, “The radiologist has looked at your CT, and he can’t find anything in your shoulder. Anything. Instead, I recommend you go to an ortho guy to check it out further, but we can’t find anything. However, he does notice that your spleen is twice the size it was a year ago, and he said that it’s crumbling. In view of your earlier treatment for lymphoma, you should probably check back with your oncologist pretty quick and have him follow this up.”
It’s almost like the first occurrence of the cancer. I go to the ER for something else and oops, you see something that turns out to be lymphoma.
Bill before, during and after R-CHOP chemo.
What was the impact of having cancer again?
The fact that it was possibly cancer again wasn’t a shock. I know enough people who have been through similar situations. I know people who have fought cancer for years, and so the fact that it keeps coming back is not a surprise. If it was coming back for me, then okay. Lots of other people have been there and done that. It looks like it’s my turn to be there and do that.
I was frankly puzzled by this shoulder business. Much later, when I finally connected with the doctor at UT Southwestern, he said, “Oh, well, I’ll tell you what that was. It was your spleen. The nerve pathways from the spleen and your shoulder travel together. We call it referred pain. Your spleen is really in an uproar, but it’s not going to hurt down there. It hurts up here. I have other patients with the same problem.”
What did the PET scan show?
He did another PET scan, and this time, sure enough, the spleen was greatly enlarged; it glowed like the moon. The sites where there were colonies of lymphoma cells were in both sides of the neck, behind the ears, around the salivary glands, in the abdomen, in the iliac region, the inguinal nodes and over here under my arm.
It had clearly reappeared in a great many places all at once. I was definitely a candidate for something a lot more serious than what was offered in the cancer center locally here. That’s why he wanted to refer me to one of the big hospitals up in Dallas.
VIDEO: CLL Treatment
Treatment for Chronic Lymphocytic Leukemia
How did you choose where to go for treatment?
He didn’t give me a staging number. What I can get out of Google is that it was probably a good stage 3 at least, if not 4. Usually with these things, if you get lymphoma above and below the collarbone, you’re in deep water.
We had a friend of a friend who had consulted a doctor at UT Southwestern, and he was extremely pleased with the outcome and the relationship with the physician. Because we trusted the recommendation and the people making it, we thought, “Okay, providentially, here’s a report that sounds credible and encouraging. Let’s go for that.” That’s what I did.
How did you find out you were misdiagnosed?
He laid out a couple of different scenarios. The first thing was to find out what I had. He was a little suspicious, I think, of the diagnosis.
Dr. Awan actually secured the tissue from the 2018 biopsy, and he started digging around in the DNA. He had resources available to him that my original oncologist did not have.
When he deployed those resources, he said to me at one time, “Well, it’s either mantle cell, or it’s CLL, or it’s a transformation.” He didn’t explain a thing about transformation. He just said it’s going to be 1 of these 3. I could tell he was betting on it probably going to be mantle cell.
Then he went and got the lab work done. He called me back and said, “Mr. Mouser, I am really sorry to tell you that what you have is a transformed CLL. You were actually misdiagnosed in 2018.”
I don’t want to leave the impression that my original oncologist is incompetent. He saw diffuse large B-cell lymphoma, and it was there. But what I actually had was an atypical CLL, chronic lymphocytic leukemia.
It’s atypical because most of the markers for that never showed up in my blood work, and yet the genetics showed that’s what I had. Then about 1 to maybe 5% of CLL patients undergo something called a Richter’s transformation, where the CLL begins to generate a really aggressive diffuse large B-cell lymphoma.
That’s what my original oncologist saw. He saw something. What he saw was really there, and he treated it. What he didn’t see is underneath is this atypical CLL that’s boiling up this aggressive lymphoma. Frankly, an oncologist in his practice might never see that. It’s extremely rare to run across a case of it.
What were the treatment options?
Dr. Awan dug and dug and dug, and he said, “Oh darn, you’ve got that.” I thought, “Okay, what do we do now?” He said, “Okay, here’s what we’re going to do.” He laid out a strategy that starts with the 6 cycles of R-EPOCH. He said, “The first thing we’re going to do is clear out all the junked sites.”
It wasn’t going to cure me. He was quite candid. He said, “R-EPOCH hasn’t cured this in 20 years. It’s never cured it, and it’s not going to cure you now. That’s not what we’re doing it for. We’re doing it to get rid of most of the tumor mass in you, and then we’re going to hit it with something else.”
That’s what we proceeded to do. We went through the 6 cycles, 6 week-long cycles of R-EPOCH. He told me later that he didn’t think I was going to make it through the first 3 because it’s pretty stiff stuff. I guess I’m atypical in a lot of ways, because frankly, I felt best when I was in the hospital.
Maybe I was just flying high on prednisone. I don’t know, but I felt good, and I went right through it without any problem. I didn’t get really sick, and the hair came out. Still, I tolerated it quite well.
At the end of October, I had another dark PET scan. We pushed that stuff so deep away that you couldn’t see it for the PET scan. That part was successful as far as it went.
What was the next phase of treatment?
It was supposed to be a stem cell transplant. I’m not exactly sure why there were delays. Some of it is related. There’s just a lot of delays in the medical profession today with the COVID stuff and the restrictions and the therapies and patients that pile up.
The holidays came up, and they had to do the HLA typing and a lot of tests. Before you do a stem cell transplant, you’ve got to contact donors. I actually discovered I had several donors, so that wasn’t going to be a problem. But then you got to contact donors and see, “Are you still going to be a donor?”
Time passed, and so November and December passed. The 4th of January, I was scratching right there. I thought I felt a lump, and I thought, “Oh, dear. Maybe this was going to be bad.” I sat at the computer and sent a note to the clinic. The next morning, I got a reply that said, “Can you come tomorrow?”
If you have a really serious cancer, you should, if at all possible, use resources in a major research center.
I did. Dr. Awan examined me, and he just kind of rolled his eyes and said, “It’s back.” Of course, by that time, I had discovered the inguinals were swollen, too. Stem cell transplant was off the table. We were off the known areas of the matter. He was thinking; I could see the wheels spinning in his head.
He said, “I think what we’re going to do is BiTE. We’re going to get you in a clinical trial for one of the new BiTE drugs. Then if we can push it back again with those, we’re going to hit it with CAR T.” That’s the current plan right now.
Processing the Second Diagnosis
What are the biggest lessons you learned from this experience?
In one of the videos the Patient Story did with Dr. Awan that I viewed, he made a comment that I certainly endorse, which is this: if you have a really serious cancer, you should, if at all possible, use resources in a major research center. Those are the places where if there is real therapeutic help, cutting-edge therapeutic help, it will be there.
Now, what put me at ease is I am richly blessed with mature, responsible, loving children nearby. If I were to drop dead now, my wife would be well protected and cared for.
It will not be in the outer rural regions. I live in a town of about 30,000, but we’re about 45 miles south of Dallas. We have great medical care here for the ordinary stuff, including heart attacks. For kind of wild and woolly cancers, no.
That’s why as soon as the oncologist that was treating me here saw this new resurgence, he told me, “You need to go to Dallas and see 1 of these 2 centers.” So I did.
That’s what I would say to anybody. Go where the researchers and clinicians are working together to fight this stuff. If there’s true help that’s going to help you, it’s going to be there.
What helped you most through the dark moments?
If I had the biggest worry, it wasn’t dying. I’m not afraid of that. What bothers me about dying now is dying before my wife. We’ve been married 41 years. You dig really, really, really deep reps in 41 years. You run in them, and it’s comfortable and everything works. There’s this wonderful division of labor between the spouses, and you just chug, chug, chug, chug, chug. Take one of them out of the picture, and suddenly it’s not only companionship that’s gone. It’s all kinds of domestic duties and processes that now devolve onto the remaining spouse.
I didn’t want that to happen to her. Now, what put me at ease is I am richly blessed with mature, responsible, loving children nearby. If I were to drop dead now, my wife would be well protected and cared for. She’s competent. She’s not sick. She’d be very lonely and grieve, but we’ve got support. The family is there to carry her on.
I’m greatly comforted by that. That also tends to greatly relieve my anxieties about, “I’m not going to make it through this one.” Anyway, at her age and my age, we’re short timers anyway, but I really wish that she didn’t have to be a widow. I think I would do better as a widower than she would as a widow, but maybe I’m wrong. We’ll see.
VIDEO: CLL Clinical Trial (Bispecifics)
Clinical Trial Types and Requirements
What was your first reaction when he said the term “clinical trial”?
I was familiar with clinical trials. We got our first initiation into cancer therapy 25 years ago when my third daughter at 9 years old contracted a brainstem tumor. The first word I had from a doctor is these don’t heal. He basically said, “We can’t fix this. The only way that there was any hope for her is out in a lab someplace in the research center.”
For my daughter, she pretty much began with clinical trials, and we went through a lot of them. Pediatric brain tumors, I think that’s probably the toughest cancer nut to crack there is. In 25 years, it really hasn’t gotten beyond where it was with her. They’re just so hard.
Anyway, that’s where I got thrown in the deep end of the pool. When Dr. Awan said a clinical trial, I fully understood what he was talking about. I knew the difference between phase 1, phase 2 and phase 3 trials.
I am 1 of 90 people in North America and Europe who are receiving this particular drug for the first time.
I was actually hoping that there was a promising stage 2 or 3 that I could qualify for. It turns out I am participating in a phase 1 trial, which I can say more about in a minute. Clinical trials were not scary. I knew that for really difficult, hard-to-cure diseases, the true therapies that will finally succeed are today going to be in a clinical trial someplace.
Dr. Awan was never unclear about that from the beginning. R-EPOCH was just a cleansing thing before we tried the stem cell transplant. If that didn’t work, then we were off into the clinical trials. That’s where I am.
What are the differences between the phases in a clinical trial?
Phase 1 trial
In a phase 1 trial, they’ve done work in a lab in petri dishes and animal studies and monkeys and things like that. In a phase 1 trial, they’re putting the drug in humans for the first time. I am 1 of 90 people in North America and Europe who are receiving this particular drug for the first time.
The purpose of a phase 1 trial is to see if the drug is safe. Will it hurt the patient? Now, obviously, they have a good idea that it’s going to help the cancer, or they wouldn’t be giving it to a human. They’ve got evidence in animal studies that it attacks and kills the cancer, so that’s good. But you still have to put it in a human body, and sometimes what happens is we go, “Oops. We can’t use this because it’s going to produce something so bad.”
A phase 1 study’s purpose is to see if this will hurt the patient. Now, if it helps the patient also, great. Once they’ve decided it’s safe, then you move into phase 2 studies, where you’re looking not only on the efficacy, but at what dose? You want to know if it’s 1 gram, 2 grams or 10 grams. Once a week, twice a week, once a year? There are all kinds of factors in dosing and timing, and these have to be discovered experimentally.
Phase 2 trial
If you go through phase 2 trials and you can prove efficacy, you can say, “This is an optimal dose.” Then you expand to a great number of much more patients, trying to get more and more data. You can generalize more and more and more about adverse consequences and how to manage them.
The FDA obviously is watching very carefully all this process. If that all goes well, then eventually they have to be able to prove it. Once in a great while, you’ll see some efficacy so spectacular that the FDA will jump in and say they’ll approve it immediately. They say, “It’s unethical to go through all of this when we see how amazingly curative it is.”
The criteria for participating in a clinical trial is set by the company that wants the drug to be tested. Dr. Awan had slated me for 1 clinical trial. Then his coordinator started digging into the requirements, and she discovered that the company had specified that the participant could only have 1 therapy post standard therapy. I’d had 2, so I didn’t qualify.
Then we went to a second clinical trial where that wasn’t a factor, and it was the phase 1 of the particular drug I’m being tested on now. I could have 2 therapies post standard therapy, and they would allow me to.
Then of course they want to know my age; they want to check out my heart. They want me standard and healthy enough so that results that come in aren’t complicated by other health problems that I might bring to the participation. That’s understandable.
There were lots of scans and examinations and stuff to verify that I met all the criteria the drug company asked for, and I was approved. We began on March 21st.
Can you describe the financial aspects of a clinical trial?
In clinical trials, the funding for that is really coming from the drug company. That includes the hospitalization if they want you in the hospital, PET scans, anything that is medically necessary to get you through there, or if you have an adverse consequence and they have to medicate you or put you in ICU.
That didn’t happen, but if it did, the drug company pays for that. The patient is contributing his cooperation as a participant, and the drug company is covering all the medical costs.
CLL Clinical Trial Process and Environment
What is the regimen of the CLL clinical trial treatment?
Beginning
It’s pretty intense at the beginning because it is the first time in humans, and there is no data on what’s going to happen. Everybody wants to be super cautious that if something goes off the rails, we can manage it quickly. That means putting me in a hospital setting. I have 1 more week to go as the last 3 weeks have gone.
Current Process
I enter the hospital on a Sunday afternoon and get settled in. Bright and early, they do some blood labs at about 5 in the morning. That is to determine what my white cell count is.
The drug that is going to be administered to me might be adjusted up or down slightly, depending on what my white blood cell count is. Then about 10:00 a.m., they begin some pre-medications: some dexamethasone, a pretty stout steroid, and some Tylenol and an antihistamine.
These are all prophylactic to put a lid on what they think is likely to be a reaction. They don’t know, but they want to be especially careful.
Then they give me this infusion through an IV. I’ve got a PICC line. They hook me up to the IV pole and infuse the drug over a period of 4 hours. At the end of the 4 hours begins another 4-hour observation period. They’re taking EKGs very frequently. They’re doing vitals every 15 minutes for 2 hours.
I wear the pressure cap on my arm or even take it off. Then it’s like every 30 minutes for the next hour, and then it’s every hour. It’s kind of tedious, but I do understand why they need and want to watch so carefully. Frankly, I’m glad. Now nothing is happening, which is great. I’m happy that had anything ever happened, they were right there.
Then I remain in the hospital for 2 more days. I take my laptop. I have work and writing I do. Then on Thursday, we do the whole thing again. Then at the end of the day on Thursday, I’m discharged to go home. I spend Friday and Saturday at home, and then the next Sunday, I’ll go back in again.
Next steps
Next week will be the last hospital stay, and after that infusions will not be twice a week, but just once a week at the clinic. It’ll be an outpatient thing. I don’t know how long that goes — I’d have to check the protocol. It’s probably another month or 2, and eventually it’ll go to an infusion every 2 weeks and then every month.
Meanwhile, they’re taking PET scans all the way through here, watching what’s going on with these swollen lymph nodes. Are they changing? Not changing? If they do change, which direction and how much and how fast? They don’t know.
It’s extremely involved at this point. In phase 1, I think it’s probably extremely involved when they don’t have any roadmap at all. We do need to be careful and very thorough, and they’re watching.
Who is part of the CLL clinical trial team?
There is a research team from Dr. Awan’s clinic. Dr. Awan is the chief investigator, but he has his assistants, who are actually in the hospital managing the paperwork. As these reports are being gathered, they’re sending them to the drug company. I don’t know where it’s located. I think there’s actually an office in the States and in Europe someplace.
Actually doing the infusion is a very simple thing. It’s just an IV infusion. I’m on an isolation floor in this hospital. It’s the place where they do stem cell transplants, CAR T and extended chemo, like I did last summer. It’s highly protected; it has HEPA filters everywhere and negative pressure stuff. I don’t know. There’s stuff in the architecture that is designed to keep that thing as sterile as possible. Nobody can get in there except patients and medical people.
What’s it like being in a controlled environment without friends or family?
It’s not been bad. You and I are talking here face to face. My wife can do this, too. We can talk a couple of times a day by Zoom or phone. She would much prefer me to be here in the evenings, but the fact that we’re separated in different universes — no, that’s not really been the experience.
I got to know most of the floor staff in the 6 weeks I was in that floor last summer. When coming back, it was, “Hi, good to see you again.” I know a lot of them, and so that’s good. I don’t feel lonely.
VIDEO: Bispecific & CAR T-Cell Therapy Side Effects
Treatment Side Effects and Records
What are the CLL therapy side effects?
I had a side effect in the first infusion, and I really do think it was unrelated to the drug. When I had the R-CHOP 3 years ago, they would give me 1 of the earlier BiTE drugs, actually rituximab.
The nurse would always ask me, “Do you feel chills? Do you feel nausea? What’s your temperature like?” I had no problems. They would give it to me in small amounts, and then as long as I didn’t react, they’d up the rate until it was gone. Same thing here, but this time I had a reaction.
There’s something called rigors. It’s like severe chills, and it’s not uncommon as a reaction to any infusion. I just never had one of those. They gave me Demerol and Benadryl, and within 5 minutes it was gone. It never came back. It never happened again. I don’t think it was related to the drug.
Have you noticed any improvements?
As far as what I see about the drug, I’ll just report I can’t judge this drug. I’m not the doctor, I’m not the researcher, and I’m not the clinician. I do know that when I went in, I had a lump about the size of an apricot pit right here in front of my ear and another very painful lump under my ear lobe. It was the lymphoma side.
Within 2 days after the first infusion, it disappeared. Of course, I was like, “Whoa, that’s amazing.” I have this big thing under here. Today, after 3 infusions, it’s now about 50% of what it was. I told Dr. Awan this. I said, “I am flabbergasted at the speed of the changes.”
I’ve thought a lot about what he said, because he looked at me and said, “Well, it’s early days.” That’s about all he said. I’ve thought about that a lot. Here’s my supposition. He’s done lots of clinical trials. He’s probably seen many immediate improvements that over time didn’t pan out, so my enthusiasm is not something he’s going to join in.
Now, am I hopeful? Of course. Do I, reflecting on it, think that I’m going to get over this by this road? I hope so, but I don’t know yet. We’re going to find out. In the meantime, I’m having fun because it is, quite frankly, a delight to get a medicine and see something as dramatic as that. I think, “Wow, this stuff is amazing.” Right now, for me, it is amazing.
How long will you be undergoing this treatment?
I haven’t got anything specific, but I think the trial that I’m participating in, I’ll continue with that until it either stops working — in other words, PET scans show that there are no changes or it starts progressing again — or it disappears and the PET scan comes back clean. Then he would probably want to say, “Okay, now let’s throw the CAR T at it.”
After the twice-a-week infusions, they’re going to do a PET scan and see. I know they’re going to see a shrinkage because I can see a shrinkage. I can’t see a shrinkage in my spleen or the iliac region of my gut, but I can see where the nodes are close to the surface. I can palpate the inguinals in here. They’re gone here and going away here.
Do you journal about your experiences?
The closest to journaling that I do is that I have a pretty extensive list of people from family and previous parishes I’ve served who are praying for me. I write to them updates periodically, explaining what’s going on and what kind of challenges I’m facing and specific things I want them to entreat the Lord about. That is my journaling.
How often does the clinical trial team ask questions about how the treatment is affecting you?
It happens pretty frequently. On that floor with the kind of therapies they’re doing for patients, there can be central nervous system complications, especially when you get into stem cell transplants or CAR T.
When the nurse comes in for those patients, it’s to say, “Tell me your name and your birthday. Where are you? What day is this? What town are you in? Recite the months of the year backward.” Things like that.
I was chatting with one of the nurses one day about this. I said, “You do this every time. I’ve got these months memorized. Can’t you come up with something different?”
She laughed. She said, “I had a patient about a year ago. I walked into her room, and she was chatting just like you are with me. I said, ‘Who’s the president?’ And she said, ‘William McKinley.’ I thought she was joking. I said, ‘What year is it?’ And she said, ‘I think it’s 1830.'”
Anyway, the woman was lucid but totally in a different place. They check up there and regularly are asking to be sure that I’m still compos mentis.
If bispecifics and CAR T had the same efficacy, which would you pick?
If both outcomes are the same, what I’m doing now is obviously preferable. It’s an infusion. It’s not painful. CAR T puts you in the hospital for at least 2 to 3 weeks, and if you have complications, that could go to 4 to 5 weeks. CAR T is still evolving.
I was talking with Dr. Awan a couple of weeks ago about the CRISPR technology. What’s going on in the research centers with CRISPR is the ability to take T-cells from a healthy donor. Then they use those T-cells. They edit the DNA in those healthy T-cells from the donor so that when they are infused in a patient, they do not attack the patient’s body. Graft host disease gets eliminated. They become like blood plasma. They can be given to anybody, not just one person.
CAR T right now works on me, but it wouldn’t work on you. CAR T is specifically individualized right now. It’s not scalable very easily, but they’re working on a different approach, where it will be scalable.
He says they can build kill switches in these T-cells so that when they insert a certain trigger chemical, an innocuous thing in the patient, all these special T-cells will just die.
It’s amazing what they’re working on here. None of these have hit human trials yet, but they’re in the works. If you know where to look in the scholarly work, scholarly journals, you’ll find reports about these kinds of things. It’s just mind boggling what they’re going to be able to do.
Advocacy and Support
Why is advocacy important?
Advocacy is best done by somebody other than the patient, if possible. That’s hard because it’s 2 people involved in the whole process. I was my daughter’s advocate, and that’s how I learned how critical it is, especially for children, to have an adult advocate all the time because they’re vulnerable. They don’t know anything. They can’t contend for themselves.
Adults are the same way, and many of them are vulnerable. Any patient is going to feel a kind of vulnerability in that setting. If you have a complaint or you think something’s not right somehow, it’s difficult to complain or challenge the people that are supposed to be helping you.
That’s why an advocate that’s not the patient is really the best, because then the patient can be a patient and the advocate can contend for the patient as needed.
The best advice I would give to somebody going into something like this is to search diligently for a good support group of people who are in the same setting, the same battle.
Never, never, never cease to ask questions of your doctor.
I’ve been part of 2 different support groups that had both patients and caregivers and medical personnel. All of them were participating, and those were wonderful because then patients can compare notes as they run into questions they have.
They can devise strategies many times about workarounds that a disease might throw at you. It’s hard to do certain things. How do you work this out? People are pretty good about helping each other.
What support groups do you want to share?
The first one I ran into is still functioning. It’s called BRAINTMR. When I ran into it, it was an email list thing back in the late ’90s. I think they’ve got a forum now, but it’s a fantastic group.
Then recently I ran across 2 Facebook groups. One is devoted to stem cell transplant patients, and the other one to people with Richter’s. That group is pretty interesting. Mostly what we’re learning is all of the different novel immunotherapies that are out there being tested. It’s really exciting to hear what’s going on.
I’m very hopeful I might actually lick this thing. I’m in it for the long haul.
If you’re hit with cancer and you don’t know anything medical, doggone it, there’s a learning curve there that’s pretty steep. If you can find anybody in a support group to help guide you on sources of information, that’s going to get you in the stream pretty fast and allow you to talk intelligently to your doctor and ask intelligent questions. Never, never, never cease to ask questions of your doctor.
Anything else you’d like to share?
I’m very hopeful for myself and hopeful for people who have the problem I’ve got. This is one of the nastier ones to have than the more ordinary kinds of lymphomas.
When I first checked out with my cardiologist about a year ago, he kind of rolled his eyes. He said, “The advances in hematology and blood cancer, we don’t have anything like that in cardiology.”
He said, “You’re very fortunate if you’re going to be really sick to have that sickness, because there’s a lot of help that’s just coming down the pipe real fast.” I agree from what I’ve seen, and I’m very hopeful I might actually lick this thing. I’m in it for the long haul.
1st symptoms: Tightness, lumps in left side of neck, severe pain in left shoulder, enlarged spleen Treatment (CLL): 6 cycles of EPOCH, clinical trial for DuoHexabody-CD37
Mary Clare’s Relapsed Acute Myeloid Leukemia Story
Mary Clare was diagnosed with acute myeloid leukemia (AML), the most common type of acute leukemia, at just 36 years old.
In her story, Mary Clare shares how she got through chemo, 2 bone marrow transplants, full body radiation, a clinical trial, and recovery. She also highlights the mental, emotional, and sexual impacts of cancer.
Full body radiation (total marrow irradiation, or TMI)
Bone marrow/stem cell transplant
I don’t think I’ve moved on. I think that I’ve learned how to manage the uncertainty. The side effects. The future.
Not knowing if things will come back and also just acknowledging that the support system that you think you had isn’t always there, your world gets pretty darn small sometimes.
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Symptoms & Seeking Answers
How did you know something was wrong?
I was running programs for a college with lots and lots of high school students, who were coming to the college that summer to be part of arts programs. It was a hectic, crazy job. I had 350 students I was working with from all over the world. I was exhausted.
Normally, I respond to situations like that with all adrenaline all the time and then crash the week after the program is over. But I had felt poorly. Everything upset my stomach, and I was very fatigued and tired.
I knew something was up, and I thought it’s a cold [or] it’s allergies. I had gone to the medical practice on campus, and they said, “Oh, you just have a cold. Here’s some Flonase.” I didn’t think anything of that.
A couple weeks later, the program ended. I felt pretty crappy, and I started to have really bad headaches. I’m a migraine sufferer from my early 20s.
But it was nothing like migraines. It was these headaches that would wrap around the back of my head. Just the worst headache of my life, so I ended up going to the urgent care at the University of Chicago, which I had previously gone to.
What happened at urgent care?
As soon as I came in and talked about my symptoms, they were very concerned. First they wanted to do a spinal tap. That scared me, of course. [I was] thinking, “Oh, I just need better migraine medication or something.”
I knew something was wrong, but I had no idea that a blood test later that day would lead to me being admitted to the hospital that same night.
How long did it take to get the blood test results?
The urgent care is an offshoot of the main hospital of University of Chicago, so they have labs that are ready. I was able to go from my urgent care appointment across the hallway, get a blood sample taken, and then I came home.
I live about 10 minutes away, and they called maybe an hour later saying, “Something’s not right. We’re thinking about having you come back to do the blood again. But just keep your phone by your side. I’ll call you back.”
When did you hear back from the doctor?
Actually, that evening we were packing to go on a trip. [It] was going to be my first trip with just my husband and I. My daughter was little. I was making dinner and packing, and the phone rang again as we had sat down for dinner.
It was the doctor that I had seen at urgent care, a young doctor saying:
This is very serious. You need to come into the emergency room right now and pack a bag. You’re going to be staying here for more tests and more observation.
How did you process the sudden news?
We don’t have family nearby, so our first thought was, “How are we going to do this with my daughter?” [She] was 3 at the time. “How do we do this with a 3-year-old in tow?”
We just go to crisis mode. For us, the feelings don’t come till a little bit later. What are the practicalities of this? I think parenthood comes with that.
My daughter’s good friend lives 3 doors down, so we called them. They didn’t answer the phone, so we just packed a bag for Twila (daughter) and walked over there, trying to say, “Mom is not feeling well. We need to find out what’s going on.”
She immediately was like, “It’s my first sleepover! This is amazing.” She was just excited.
It was very odd. You’re putting on a face for your child.
My husband took her to the neighbors’ place and knocked on their door. They didn’t answer the phone because they’re in the middle of story time for their girls, but they welcomed her with open arms and said, “Whatever you need.”
It really made us be able to take our parent hats off and be able to absorb some of the situation. It felt really hollow. It felt like dread. It felt like something I’ve never felt before.
How did you decide where to go for medical advice and treatment?
My husband works for the University of Chicago, and my daughter went at the time to the laboratory schools, which is associated with the university. We would very much call ourselves a university family.
The majority of our friends work for the medical center or our academics, so we’re kind of in that world already. It’s just down the street. My husband walks to work, and I previously have worked there.
It felt like we weren’t going anywhere new or different; this is our neighborhood. It’s just a block from my husband’s office and a couple blocks from my daughter’s school.
It was a bit surreal in that regard, because it was just like we’re driving past our grocery store. I know where to park and all. Just very strange knowing that we were going there not knowing what that next piece would be.
We were totally clueless that I would be in the hospital for the next 6 weeks [and] that we would be dealing with this many years later as well.
We were pretty darn clueless, and we were hopeful, scared. I’m probably making really stupid jokes because that’s kind of how we deal with things.
Describe the first procedures at the hospital
What was surreal is that we had an appointment at the ER, which is not something you do. They knew we were coming. It almost felt like going to like a restaurant and saying, “Here’s my reservation. I have a reservation.” They had a room ready for us.
It didn’t take very long until 3 doctors, at least 2 of them oncologists, came in the room. They laid it out that based on my blood sample that they had taken earlier that day, my white count was really strange.
The rest of my blood results were out of whack. Their best understanding at that time was that I had leukemia of some kind, some sort of a blood disorder.
They did use the word “cancer” but said that they needed way more information. What they did know is that things move very, very rapidly with blood cancers and blood disorders. To be able to provide me the best care, I needed to check in to the hematology-oncology floor at the new hospital just a couple steps away.
It was a Friday night, so we actually had a weekend in the hospital where they checked in a little bit, but I didn’t really see the person who would become my team.
The 6 people that would come and really talk to me did it Monday, so it was very odd. I was like, “This seems so financially crazy to have me stay here for 2 days and just kind of check in on me, where I felt fine.” I didn’t feel awful. I felt a little sick but not terrible.
What were the first steps once you were in the hospital?
Monday, they hit the ground running at like 7 a.m. It was meeting with teams and learning what the plan of care would be.
Are we going to start immediately with chemo? We would do a bone marrow biopsy to get more information. All of those things went into place.
It was a head-spinning day, but we had that weekend to be able to kind of rally our team and support and to do some research on our own. We had actually [gone] into meeting with the oncology team pretty informed.
A good friend is an oncology pharmacist. She deals a lot with transplant patients, so we were pretty well informed.
Bone Marrow Biopsy & Diagnosis
Describe the bone marrow biopsy
I’ve probably had about 20 bone marrow biopsies at this point. The first one, I had no idea what I was in for.
They basically explained it to me, “We’re just going to take this tiny little sliver of your hip. It’s a very quick procedure. It’s done at the bedside. We don’t have to put you under or anything like that; we will numb the area.”
In my mind, I had thought of like when I had a mole removed or something like that in dermatology, that it would be something akin to that, but a little bit more. I think in a lot of ways, my doctors and my team have tried to not totally scare patients.
Not all details are shared before certain procedures. This particular one, [they said] you’re going to feel a pinch in a burn, there might be pressure, things like that.
What I realized pretty quickly is that it’s sort of like getting a root canal on your butt. That’s the best way that I could put it, because they do a little bit of work [and] have a bit of a drill.
I was pretty well drugged. Over the years of doing this, I now know my favorite cocktail of drugs to have before before a biopsy.
Was family in the room?
My husband was sitting there, also having no idea what was going to happen. My mom had flown in from Virginia, and so she was on the little patient couch at the end of my bed.
You’ve had about 20 bone marrow biopsies. What’s your advice on how to deal with them?
I think anyone who’s going undergoing a procedure where you’re either getting your port in or a PICC line — a bone marrow biopsy, in particular, it’s good to know how your body reacts to different medicines.
For example, if they give me Dilaudid, which is a very typical drug to be given that causes you to be mentally out of it, that for me was successful as far as no pain, but I would be vomiting for hours after.
I would feel way out of it and would just have to sleep for the rest of the day. I realized that was not the right drug for me, and I had to ask for something else.
I ended up with what they think is a lighter alternative, which is a heavier dose of Ativan mixed with Benadryl. I’m not mentally engaged with the pain. Certainly, I can feel things, but with Ativan you have a very limited memory from that experience. It does incur some memory loss, which in this particular case is great. I was totally down and okay with that.
Also, in previous outpatient settings, after using just the Ativan, I could sleep for a little bit. After the procedure on the table, maybe an hour after that. Then I’m a little out of it. I certainly can’t drive myself home.
I’m able to walk the block or 2 to the parking garage, have another cup of coffee at home, and restart my day. It doesn’t derail everything. It took a while to figure that out.
It also took a while to figure out that there were some members of the team that were seasoned and more experienced in doing difficult bone marrow biopsies.
I’ve learned that I’m one of those people that it is tricky. Some people have more forgiving bones, and I don’t. I learned the same thing goes with blood draws.
I’m a really tough stick, and so you need someone who has the combination of skill and confidence. If they don’t — if they have the skill but they don’t have the confidence, it’s not going to happen. Likewise, if you have the confidence but not the skill. Those are some things that I’ve learned over the years.
How long did it take to get the bone marrow biopsy results?
For the bone marrow biopsy, we received some news the next day. They had everything you would need on site at this particular hospital because it is a research institution, so they were able to get some of that staining back quickly.
They were able to get a deeper understanding of how many blast cells, but with the type of work that they’re doing, they also do a couple different other stains that take more time to develop. Then I would receive more information later in the week, if not the following.
That’s when they were able to tell me pretty much this is AML leukemia, based on what the cells looked like. They were able to tell me my percentage of blast cells, which really didn’t mean much to me at the time, but that it was aggressive.
There’s no stages for leukemia. There’s no Stage 1 and Stage 4. There’s nothing like that. It’s percentage of disease.
It’s not a cancer that is often found very low levels. It is in the 20+ percentage of these abnormal white cells that are overcrowding and hacking your body.
For me, learning that it was like 20 or 30% didn’t mean a lot. But knowing that you’re not supposed to have any, that it’s considerable, meant that they needed to move and act quickly. Once the body starts replicating the cells, it’s just going to continue and continue until it destroys your body.
How did you tell your daughter about your cancer diagnosis?
When I was first diagnosed, my daughter was 3 and was pretty clueless beyond, “Mom is sick.” She’s a smart young lady. She is inquisitive to the nth degree, so there was no keeping things from her.
I brought her to doctor’s appointments. When she was able to visit the hospital, we brought her. We didn’t shield her from much. We didn’t go into big, long details if something was going on. But if something was happening with my heart, I told her.
We had many medical supplies at home. My lines had to be cleaned. Infusions at home happened at some point, and she learned how to do all that stuff when she was 3 and 4. She’s probably a future doctor.
Over time, when I’ve had major mobility issues and issues with syncope and things like that, she is a caregiver. Her capacity to take care of other people is well beyond her years, and well beyond what anyone would expect from a child.
It breaks my heart to think that I’ve taken part of her childhood and innocence away from her.
But I don’t think we could have survived any other way.
She has very close relationships now with my mom, her grandma, and my husband’s mother (her other grandma) that would have never ever happened if cancer didn’t come into our world.
Luckily, I was at the University of Chicago. They have an adolescent and young adult clinic for blood disorders and specifically leukemia, so I was able to be with the foremost experts, not even knowing it.
I was starting to talk to people in my research and my husband’s research like, ‘I have the option of having one of the top experts, Dr. Wendy Stock, as my oncologist.’
It was an interesting process because she wasn’t rounding when I first came in, but she learned about my case through the weekly transplant meeting.
She came to my bedside and asked if she could be my main oncologist, which was just so cool. It was very patient-facing and very warm to have someone say, “Can I be your oncologist? Here’s my credentials, and this is why I’m interested in you.”
Induction Chemotherapy
What were the treatment options?
They had already presented some clinical trial options, mainly just different dosages of different chemo agents that they thought might be better for me, because I was in my 30s.
Typically people who get leukemia, if you look at the percentages, high amounts would be infants and very, very young children, as well as older adults over 70.
There’s a very, very small group of young adults, who would be classified between 18 and 40, that would develop this disease. It’s not unheard of, but it’s pretty rare.
What was your chemotherapy treatment regimen?
First off, it’s called induction chemotherapy. I believe it’s a 3-1. There are 3 days with a certain cocktail of drugs. I was only given very, very high doses of chemo over 2 weeks.
You had 3 days of chemo but stayed in the hospital for 6 weeks
The reason I was in the hospital for 6 weeks is because you cannot leave until your blood counts are at a level where if someone coughed in your vicinity, you wouldn’t get that. It would become pneumonia.
You need your immune system to be functional in the smallest amount possible. When you’re given this very, very heavy, high-dose chemo, it just destroys your immune system, as well as destroying the cancer.
That’s a major side effect, and they don’t want to release you back into the world, even if that is isolation in your home, until you’ve reached a certain standard with your blood counts. It took a while for mine to go back.
Describe your PICC line
I had a PICC line installed in my arm, which was a bedside procedure. [It was] somewhat uncomfortable, but not terribly.
I’ve had 2 PICC lines. That’s basically a line that goes directly into your heart from your arm. That would be a way for them to easily give you medications and drugs without having to start an IV each time.
It’s semi-permanent. You don’t have PICC lines for terribly long; 6 months is typical. I was hooked up with that.
What were your chemo infusions like?
Once a day, I would be given a drip bag of those chemo agents. That was typically a couple different bags hanging from an IV pole. The first couple days of that regimen, I was able to watch TV and be up and about.
They said walking the floor was okay, but I was not allowed to leave the hematology-oncology floor, go to the food court in the building, or anything like that. I was wearing my normal clothes. I was able to take a shower. I was able to do kind of my normal things the first few days.
After that, the side effects of chemo, where it really is starting to ravage your body, kind of took over. My blood counts dropped; red, plasma, and all those things were problematic. I started to be on that IV pole a lot because I was receiving platelets, red blood product, and I was receiving fluids as well.
As the weeks went on, they added potassium and magnesium because your body is really being depleted of a lot of the essential things that it needs to run.
Describe more of the chemo side effects and what helped with them
Main chemo side effects from the first induction round were really poor appetite, things started to not taste right, and just overall fatigue. Upset stomach was another thing, sometimes diarrhea, sometimes constipation back and forth with that.
Not only was I starting to feel poorly around the third day. No appetite. I did get a rash, which they think was from the red blood product. That happened once and never again. I was very uncomfortable.
I think initially it was the huge rash, head to toe, just itchy, and felt yucky. As soon as I presented with that, they had dermatology come and check me out.
When you do have a rash on the outside of your body, there’s something going on inside as well. You want to make sure that that can be looked at and dealt with quickly.
We realized at that point that you can get calamine lotion in a spray form. It was super helpful to have my mom, my husband, and some close friends who could run to CVS or the drugstore to be able to pick up little things you need.
I also packed a bag for one night. I had no clue that I would be needing my family to make sure I had clean socks and underwear and that I had the comfy kind of pajama-type clothes. That was really helpful. That first week or so, it was kind of like, ‘Well, what do you need?’ Setting myself up to be pretty self-sufficient.
Most everything was well controlled with medication. I was given any opportunity I wanted to be able to take anti-nausea medication, which was helpful.
I needed to figure out which ones again would be good as far as still letting me be somewhat conscious, because many of them will just knock you out and make you very, very tired.
You can sleep through all of this if you want to, but realizing that I was going to be there for a few weeks, I wanted to do something. I want to actually spend my time a little bit better, especially since family had flown in to be with me.
Figuring out ginger ale was very helpful. Ginger candies were helpful for an upset stomach. The main thing that has helped me over time has been heating pads.
In the hospital, a nurse can give you a little packet that they shake together and pop. It’s a nice hot, a little kind of a pillow that you can put on whatever is hurting you. That for me, especially while you’re waiting for other medications to kick in, is a lifesaver. It can also be very soothing if you’re trying to get to sleep.
Those were always things that I noticed. The nurse came and did her rounds. First thing in the morning, she’d load me up. She’d say, “Here you go, here’s 3. You’ll be good for the day.’
When I’m home, I use my heating pad that plugs into the wall. Those things were helpful.
I think still being active. Trying to get out of the room to walk around was helpful for digestion, for appetite, and for overall fatigue.
The fatigue is going to hit you. You’re going to take a nap, you’re going to go to bed early, you’re going to feel like watching a movie or TV or doing something quiet, and you’re probably not going to want to entertain a lot of guests.
Luckily, maybe once a day I would have some folks come over for maybe an hour, but the rest of the time I spent mainly alone.
Describe the routine while you were inpatient after the chemo infusions
I was just stuck at the hospital. I’m stuck in my same room. It became a typical routine that I would be woken up at 6 a.m., and they would do a blood draw, weigh me, and take my temperature, my blood pressure, and all that good stuff.
I could snooze a little bit after that. It may have even been like 4 in the morning. I’m not sure. It was crazy early. Depending upon the day of the week or the weekend, I may not see a doctor at all, but during the week, I would then see a doctor sometime between 9 a.m. and 1 p.m.
It was very vague when that team would be rotating through doing rounds. They would say, ‘Here’s your blood counts. Here’s what’s going on. Specifically, looking at the panels, you need potassium today or you need this today.’
Then asking me, “What are you feeling? What do you need as far as mitigating side effects and symptoms?” That just became the routine.
I watched the first 2 seasons of “Scandal” and talked to a lot of the nurses and the nurse assistants about all of that!
White blood cell count recovery took longer for you
After 2 weeks of chemo, I was still in the hospital for 4 more weeks because we were waiting for my blood counts to recover. It was unbelievably boring and stressful because I was a bit of an outlier.
Typically it takes a week or 2 for counts to come back, but my body really fought against that. I was not a candidate at that particular time, [because of ] the regimen that I was on, for something like Neulasta that would enable that to happen. It would cause more cancer cells to grow at that juncture, so I was just kind of stuck there.
What was next after 6 weeks in the hospital?
I was able to go home, be with my family, and rest my body a little bit. I was still going into the outpatient clinic at least once a week, sometimes more, depending upon side effects and symptoms. [I was] getting an understanding of what’s going on with my body.
How did your body react to the first chemo?
They realized after those 2 weeks that [my body] was responding to chemo and could put me in a temporary remission.
Bone Marrow Match & Transplant
Describe the bone marrow matching process
They began the process through the bone marrow biopsy and a million and one blood samples to find out what my biomarkers are, [as well as] what’s unique and special about my genome and my specific cancer to provide personalized care.
They would also look to see all the different special things about my bone marrow to be able to find a match in the registry. I don’t have any siblings, so I didn’t have any family to go to for that. It’s a very long and arduous process to find a match.
A good match takes a month sometimes, so they begin that process very early to see if that was going to be a possibility for me.
In a perfect world, if you had a donor lined up, you would have heavy-duty chemo and then immediately have a transplant.
That’s not how the world works. It takes a lot of time to get your donor in place, to make sure that you have a good match, and that all the legality is put together.
What’s “consolidation chemo”?
The initial chemo is to really test your body to see if you can get into remission. During that process, you’re waiting for that donor and that time to be set up for your insurance to approve everything.
Your body will start to probably make cancer cells again, and most patients that I’ve spoken with and that I know have all had something called consolidation chemo.
You may even have multiple rounds of consolidation chemo, and that is another couple days-stint of heavy-duty chemo agents that will keep your cancer down and your white cells at a more normal level.
It’s not as intense as induction, but it’s still a heavy-duty dose. For me, I went inpatient. By that point, my body was like, “Oh, okay, so I’m supposed to suppress everything, and then I’ll make some more cells.”
I didn’t have to spend 6 weeks in the hospital. I was very, very fearful of that. I only spent a week in the hospital for my consolidation.
Describe the consolidation chemotherapy regimen and side effects
It was 2 days, and side effects were a sort of mini version of the induction chemo side effects. The only big difference in side effects at that point is we had realized that I had become menopausal, so I was going through hot flashes. I was going through just feeling out of it and weird. My period had stopped.
I was also going through this really quick month of just drenching my pillow every night and being very unhappy. That was my very sped-up version of menopause. For women, it’s typically over the years.
Mine was over about a month, so it was intense.
Also, I had a lot of upset stomach. My skin was uncomfortable. I think I was having some dryness, and part of that is just being in a hospital environment and being hooked up to things. My skin was very fragile.
Nausea, upset stomach loss of appetite. Food tasted weird. I started eating just a lot of very plain food. Salt was helpful. Hot sauce was helpful if I could tolerate it.
How many bone marrow transplant matches did you end up having?
They had realized that I’m the whitest person alive and that there are many matches for me. They found out that I certainly had some matches that were potential in the system.
It was very vague at that point. They said there’s about 5 or 6 people that are a possibility worldwide, Germany being the biggest donor pool. Those are European folks. A lot of your bone marrow and your makeup has to do with your race.
For me, [I have] European origins on both sides of my family, pretty much English, Scottish, German. I was not a big mutt, so it was easier to match me, which is very unfortunate for many people who have much more varied lineage or come from other nations. I was able to be matched up.
At first, the doctors really wanted to consider and look very closely at each potential match. They were looking at things on a chromosomal level because much like a heart transplant or kidney transplant, the body may reject something foreign.
To mitigate that, to make sure that the chances of that are low, the matching factors — I believe there are 10 to 15 of these parts of your chromosomes that they’re looking at to see if they’re going to match with that donor. It’s called a match donor.
You can also get an unmatched donor, where they’ve got half of the chromosome. It’s much more risky, [and there are] way more complications after the fact. The closer the match you can get, the better outcome you’re looking at.
I found out later they were coming from Connecticut, but just because someone has registered themselves within the bone marrow registry doesn’t always mean that they will follow through with giving you their cells.
They have to narrow it down to the best matches and reach out to those individuals to see who is willing to move forward with a medical procedure to save someone else’s life.
What was the transplant process?
The beginning of November, I was brought back into the hospital for my transplant. I was given a day’s worth of heavy-duty chemo just to make sure everything was suppressed so that when the new bone marrow came into my body, it would be able to have space and room to replace mine.
There were a couple of intense but exciting days leading up to that transplant. It’s a risky process. Before the transplant, I needed to get a Hickman line installed, which is a central line that’s in your chest wall that is a better multiple line into the heart and circulatory system to be able to deliver drugs. It lasts longer than a PICC line.
They require a 3-1 Hickman for transplants so that you can get hooked up to a bunch of different stuff at the same time. That was my first process, going into Interventional Radiology to get that put in. Then I was brought up to my room and given heavy-duty chemo. The transplant happened on November 6.
It seems like any other blood donation. You’re getting a bag of plasma. It’s yellow.
You know how far it’s come from because if it has a preservative in it, it smells a little bit like chicken soup. You can smell down the hallway when someone’s getting a transplant if it’s from Germany (or comes from farther away) and had to be couriered over in a slower process.
Mine was fresh, so I didn’t have any of those smells. We knew this is good. The only thing I knew about my donor was that he was in his 20s and was young. That’s also a good factor. I didn’t know the name.
I didn’t know where [he was]. I didn’t know if I would even find out those details till later. You have to wait a number of years, so it seemed just kind of like a regular donation coming down the line.
We knew that these were magic. These were special stuff. We’re all excited, and it’s a birthday, too, so they sing ‘Happy Birthday’ to you because your immune system is brand new. It’s just been born.
I think my mom brought a balloon. We weren’t allowed to have fresh flowers or anything like that. I did not want any cake. It was tricky because for the transplant process, the cold and flu protocols were put into place by that point in the year, so children under 14 were not allowed to visit.
I was not allowed to see my daughter during that time, and I feared that I’d be in the hospital for 6 weeks or more based on previous experience. That was really hard. We’re doing FaceTime and all that kind of stuff. I missed out on Halloween that year, so they sent pictures. It was hard.
What was it like after the bone marrow transplant?
After you receive your stem cells and they’re going through your body, it’s really a waiting game to see how your body’s going to react. There’s many mitigating things that drugs can give you, steroids and things like that.
They begin this protocol the day before the transplant. Pills you’re taking, so you’ve got antivirals, antibacterials, drugs to prevent pneumonia, steroids to help your immune system. All these different things get put into place that also inform you that your body is heavily at risk, because you have a new immune system.
How did your body react to the bone marrow transplant?
The side effects were very similar to the chemo. More than anything else, that was the chemo that I was feeling side effects for more than the transplant.
Very intense fatigue. The steroids also made me feel a little bit weird. I was on a pretty high dose of steroids. Lots of upset stomach. I did not want to eat. I did have mouth sores, which with high-dose chemo and many other types of chemo is common.
They did give me one type of chemo that is very much known for creating mouth sores, and I had mouth sores all the way down inside my throat. I couldn’t speak, and I had a very difficult time swallowing. It resolved itself.
After about a week, it got slowly better. It was unbelievably frustrating because the 3 things that doctors are constantly telling you to do after transplant is to move around, go for walks, and eat and drink water. They are measuring how much water and food intake and exercise I’m doing every single day.
I was not able at some points to do what they needed me to do, but I worked really hard at it.
Even if it was, “I can’t eat, but I certainly can get my husband to pick me up the highest calorie banana smoothie he can find with full fat ice cream in it.” I’ll have a couple sips. That’s better than nibbling on a cracker. It was also difficult because being vegetarian, there wasn’t a lot of food on the menu, so I ate a lot of peanut butter and jelly.
A very scary thing was [with] the main doctor who was on call — not my oncologist, but the main transplant doctor I was working with. For those particular weeks, when it was time for me to go home and my cells had recovered enough for that to be safely done, she was not comfortable releasing me since I had a preschool-age child at home.
It took advocating for myself and working with my nurses to figure out what other doctor I could ask to see. I realized and did some of my work talking to the nurses, realizing that the doctor that I was working with was rather young, didn’t have children, and didn’t really understand that the whole reason I went through this process was to be a mom and to be with my family.
So I ended up meeting another doctor, who was wonderful. He has 5 children, so he got it. He understood, and we ended up making a deal.
We pulled my daughter out of school for the first 100 days after my transplant [because] the first 100 to 120 days are meant to be high risk.
Patients are in isolation at home or in the hospital. You can’t really go anywhere. You could wear your mask and gloves — very similar to this pandemic. Very strange.
A lot of that is because your immune system is being suppressed by immunosuppressant drugs so that you do not reject the new cells.
They can slowly wean you off of that if you are not having graft-versus-host acute symptoms and reactions. I was able to be weaned off of those pretty quickly in a number of months.
What should people know about that high-risk recovery period after the bone marrow transplant?
It’s also critical to have a caregiver during those 100 days. They would not allow me to have a transplant unless I had a 24-7 caregiver with me at my side monitoring me for any issues that may arise.
I also was not allowed to be further than 30 minutes away from my hospital.
My husband needed to take care of my daughter and needed to work, so we brought in my mom.
Were you able to have any visitors outside of your husband, daughter, and mom?
Yes. You just basically had to interrogate everyone like, “Do you have a cold? Does someone in your life have a cold?”
Where there any other steps you took to help protect yourself and weaker immune system?
I made my husband stop going on public transportation. There’s certain foods you’re not allowed to eat. You’re not allowed to eat fresh berries. You’re not allowed to touch soil. You’re not allowed to be around flowers. You’re not allowed to clean a litter box or pick up dog waste or anything like that. You’re not allowed to do the dishes.
There’s a lot you’re at risk for: viral, bacterial, all sorts of things. Fungal can actually kill you. It’s insane. When your immune system is that suppressed, you’re under some pretty strict protocols.
Any other tips on how to best isolate at home?
Figure out how you can connect with your community, whether that be a community of cancer patients, your community at church, friends, family — through the phone or through social media (if you’re comfortable with it), through email — to really make sure that you are making sure those relationships continue.
I think finding other people who are maybe 6 months or a year out from what you’ve been through is unbelievably helpful. You’re going to have a million questions. To be able to go to some of these communities online and ask those questions from informed people that speak in plain English not in “doctor-ese” is really comforting and really helpful.
You developed chronic graft-versus-host disease (GVHD)
I developed graft-versus-host disease a number of months after my transplant. This is typical. Oftentimes patients have some sort of acute graft-versus-host directly after transplant. It can impact any part of your body.
It’s truly your immune system saying, ‘Hey, there’s some old immune system here.’ It’s fighting it out, so it can fight it out in your kidneys, your skin, your muscles, your eyes, what have you.
I had some dry eye after my first transplant and was able to handle that with basic use of eyedrops. The main factor for me that was an issue was it really felt like I gained arthritis in my hands, and they were very sore. It was difficult to do knitting or crafting things that I regularly did, and that was due to graft-versus-host in that kind of muscle skeletal area.
How did you determine it was graft-versus-host disease (GVHD)?
I needed to see a number of different doctors to kind of eliminate all the possibilities that it could be before, because there’s no test for graft-versus-host.
It’s about observing over time and eliminating all the other things it could be.
What helped with the GVHD?
I was able to go on to Celebrex, and that was very helpful. Did physical therapy, but was not helpful. Didn’t do the job, but Celebrex was helpful.
I still get fatigued. I still have times when I need to massage my hands, put warm packs on there, or do different kinds of stretching.
Being at a teaching hospital, I was often presented with opportunities to do clinical trials. Some of those were as simple as a 1-page questionnaire about my mental health.
One that was much more involved was the WT1 study, which was a vaccine, looking at a particular mutation that I had and trying to prevent relapse from cancer. It was an intense undertaking.
How was the main clinical trial you underwent?
The drugs were completely covered by the research study, so all I had to do was just show up on a staggered basis. First, 3 times a week for the first month, and then 2 times a week for the next month, and so on and so forth until it was every 3 weeks. I would receive an infusion. It was actually an injection, but it was very thick, so it was more like an infusion.
I would have to be at the hospital for 4 to 5 hours. They would not make the drug until they saw the whites of my eyes because it cost $10,000 per injection. But I did relapse. It was not a successful study.
Were there any side effects from that infusion?
It did not have many side effects for me beyond taking my time. I learned to make my clinic room into my office. I brought my laptop, and I would work from there on those days. It worked out for me.
It was a good transition emotionally and mentally away from very intensive getting blood counts every couple of days back into a life that isn’t totally structured around cancer.
Resuming Life
When did you decide to go back to work?
When I felt like it was time for me to go back into the office, I actually started at home. We did a trial period of a month where my daughter went back to school; I was healthy enough to have her bringing germs home. We tried that out to see how that was going to work.
I worked from my home office, which kind of worked and kind of didn’t. I just had the type of job that was difficult to work from home based on a lot of meetings, and the tech wasn’t in place. So I did return to the office.
How did you feel when you physically went back to the office?
I will say that I had a lot of fatigue. I had a lot of brain fog, ended up going on more intensive anti-anxiety medication, and started a stimulant to help with the fatigue, which was helpful for a short amount of time.
I was able to transition back to the workforce, and it was very gradual. Every month or so, I would feel a little bit more like myself and a little bit more like myself. I would say after a year after transplant, I felt like my old self.
I was definitely a different person, mentally and physically. My get-up-and-go was back and my ability to focus on other things had changed, but I was able to do the things that were meaningful to me.
Relapse
When did you find out the cancer was back?
In August a couple years later, I had my yearly appointment with my oncology team. That’s a physical, as well as taking blood samples. They typically take 5 or 6 vials, and they’re testing for a whole host of different things and comparing it to your last visit.
I felt fine. I thought everything was great. I was moving on with my life, and things were going pretty well.
Unfortunately, 2 days later, I received the call that I needed to come in for a bone marrow biopsy because my blood samples too didn’t look good.
They weren’t sure, but they needed to get more information. I came in for a bone marrow biopsy just a couple days later and quickly received the results that a very low level, almost unheard of, of disease was found in my bone marrow and that the cancer was back.
There was a very low level of disease
It was strange because I was so used to the AML process with my experience and many survivors that I’ve talked to and their experiences. If you have AML, you’re immediately in the hospital, and you’re getting treatment.
I relapsed with I think 9% disease, which was a big complicating factor in a number of ways. That is unheard of. It doesn’t make any sense to give someone with that low-ish level of disease heavy-duty chemo and put them on the transplant train. There could be other things at play there.
I was just lucky that I had a scheduled appointment, so they found it very early. They were actually able to take some time and look at a number of different ways to treat this.
How did they treat the relapse?
I was treated outpatient for the first little more than a year of relapsing. We tried a number of different drugs. We tried a drug called azacitidine, which is often used for pre-blood cancers. MDS is that blood disorder.
How did your body respond to the azacitidine?
It was successful for me that it was able to keep me at that 9%. My body had very little side effects. I didn’t lose my hair or anything like that from this particular drug. It is a low-dose chemo.
What adjustments did you have to make at home and at work?
I did have to go in for those treatments, but I was able to live my life at home. I did know at that time that a second occurrence of leukemia does not have great odds. I immediately quit my job and went on disability.
The disability process takes 6 months or more, even if it’s fast-tracked, so I knew from my experience working with other survivors that I needed to do that and do that quickly.
How long were you on azacitidine overall?
I was on azacitidine for a little over 6 months, and then it stopped working. They were starting to see more development of disease.
Describe the clinical trial for venetoclax
They decided to try a clinical trial for venetoclax, which at that point in time was only approved for another type of cancer, CLL (chronic lymphocytic leukemia or small lymphocytic lymphoma), and it was in trial to be seen if it was an immunotherapy that was effective for AML.
That I received directly from the manufacturer. The manufacturer paid for it. It was unbelievably expensive. You would receive a pack of pills, kind of like a booklet. I took that at home, and there was a very specific way I had to take it.
I had to do weekly check-ins with the pharmaceutical company and weekly check-ins with my doctors.
How did your body respond to the venetoclax trial?
It didn’t really do anything. For my particular case, it didn’t have many side effects either. They really wanted to give it a good go because it had been successful with other patients.
They wanted me to take it for at least 4 months before they would abandon this treatment regimen. I took it for a while, and then we started going back down the transplant route.
How did you get off the drug?
It was once a day, but when it was time for me to get off of that particular pill, it had to be stepped down in a certain way.
2nd Bone Marrow Transplant
Describe the preparation before your 2nd transplant
Since I did have a low level of disease, my trajectory towards transplant the second time around was quite different. I did not have to do induction and consolidation.
That was compressed all together before my transplant. Once my donor had been picked, all of that paperwork was put together, and the schedule was put forward, we could move a little slower.
November, I checked back in into the hospital and began high-dose chemotherapy for the week before my transplant.
They added radiation to the regimen
They added full marrow radiation. It’s not quite full body radiation. I had 3 of those visits. That took a very long time. They tattooed parts of my chest and my stomach, and that’s where they aimed the radiation.
That is just like an extra thing. They wanted to do something different than they did the first time around, which was just standard protocol. They wanted to add some bigger guns to try and have my transplant be more successful long term.
Describe the radiation process
The radiation therapy was pretty hard mentally, having to be still, having to have casing over my face, this web fitted to my face. Having doctors move in and out of the room because of undergoing something really toxic was very scary.
I didn’t know how to prepare myself for it. I didn’t really know much or anything about that process. My previous treatments had been pills or infusions, and you have a little bit more control over your body, your surroundings, and how you distract yourself.
You are completely in the moment when you receive radiation. I think being unable to distract myself, even though they played good music and things like that, was difficult.
How many times did you have to undergo radiation?
Just 3. It was a couple hours each time, but there’s so much positioning and moving. I don’t know how much of that stuff was actually receiving the radiation, but it was hard. You had to go to a separate room for that.
I was transported from my inpatient room to the basement of a nearby building because they want to keep the radiation away from most people.
Were there any side effects of the radiation?
I did have major side effects from the radiation. My adrenal system failed. I actually lost consciousness the last time I did radiation. Trying to get on the table, I collapsed, and they called the cart and all that sort of stuff.
I did come back, and I didn’t injure myself. I had some bruises, but they did go through with radiation because I needed it after that, which is just bizarre. But the radiation has done some considerable damage to all parts of my body.
How soon after the radiation did you undergo the bone marrow transplant?
I believe I had my last dose of radiation in the morning and then had my transplant later that day. It was a really rough day. It wasn’t this “happy birthday” type thing because I had started to lose consciousness and had blood pressure issues.
I was up all night with tests. I was taken for CT scans, MRIs, and all sorts of neurological examinations to try and find out what was wrong. Everything was inconclusive. It was very difficult to try and figure out what was happening.
What were the side effects of this second round of transplant and chemo?
I was losing consciousness a lot and was put on bed rest. At that point, all the side effects of the chemo kicked in. I had vomiting and diarrhea all the time and could not take care of myself.
I was really at the mercy of wonderful nurses, who took care of me and cleaned me up a million times a day.
It was a totally different experience because I really wasn’t really able to advocate for myself very well. I’m a medical marijuana user, and that had very much helped me the year before my second transplant mentally to deal with all the depression and anxiety.
I wanted to use that in the hospital during my second transplant. I didn’t smoke or anything; I just used edibles, but they really discouraged that. They didn’t want that to happen, and I understood.
I was given the synthetic version of marijuana, which is called Marinol. It’s a pill. I hallucinated for days on end, and it was terrifying. We realized that was what was going on, so they took me off of that. It was really, really hard.
2nd Recovery
How was this round of recovery?
I was in the hospital for 6 weeks. That’s long, but my family lost their minds when they did decide to let me go home because we live in a brownstone building with a big staircase.
I was collapsing constantly; I was this major, major fall risk and needed so much care. [I’m] someone who doesn’t have an immune system [and] is totally isolated.
At that point, my body stopped making magnesium and potassium, so I needed to be taken to the clinic every single day, sometimes twice a day, for hours at a time.
That was at least a little bit of a relief for my family to be like, “Okay, she can go and be with that team of nurses and be taken care of [to] give us a break and take care of [her] daughter while all of this is going on.”
We’re all on super high protocols at home. You come home, you sanitize, you leave your shoes outside, you were constantly washing clothes at high temperatures, and all that sort of stuff because I was very much at risk.
I physically was more vulnerable looking and acting than I ever had been. I really came home as a very different person. Then I started to have some cardiac issues that would come and go.
We think it’s due to one of the chemo agents that I had in 2014. There has to be a heart failure that has to be managed. It’s not a considerable amount of heart failure.
The other thing that’s really important after transplant is monitoring pulmonary, because it can go down very quickly.
Graft-versus-host disease of lungs is common. If it’s caught early, it can be dealt with. I was doing great pulmonary-wise during all my testing monthly, and then my pulmonary function just dropped with any exertion.
This is right when we were kind of figuring out how to repair my adrenal system. I was not having to use a walker all the time or a wheelchair. I was starting to make my own cortisol. Then my pulmonary function just tanked, and they put me on oxygen 24 hours a day.
What helped with your pulmonary recovery?
I worked with the most amazing pulmonary specialist, and she was able to to really work with me and figure out that this one particular anti-pneumonia drug that I was on called dapsone was just destroying my pulmonary function.
Literally, after struggling for months, my pulmonary function was completely normal.
How are you doing after the second transplant?
We’ve been able to manage a number of the aftereffects of my transplant. Some are ongoing. I’m one of the healthier people in the oncology office, but I have a new primary care physician, and I’m like the sickest person she’s ever seen.
At this point, heart, lungs, and sexual side effects are managed by treatments and therapies.
I go to the doctor more than the average person. I’m able to lead a pretty normal life. Fatigue is still a major, major factor, and I will have days where I just need to go back to bed. That’s becoming less, but it’s still there.
Once my adrenal system came back, many of my symptoms and the constant dizziness and verge of collapse resolved. Now when I have fatigue, I’m very dizzy and need to really remind myself so that I don’t lose consciousness.
How often do you have to go in for blood tests?
I’m on a monthly basis right now, though things are totally out the window. They have to closely monitor. I’m on every 3 months with the endocrinologist and a cardiologist.
What is life like now after treatment and transplants?
I do a lot of work on my mental health. I have a therapist. My daughter has a therapist. My husband has a therapist. We have family counseling. We’re all very upfront with each other about what we need.
I totally take antidepressants and anti-anxiety medications and for chronic pain. Medical marijuana has been a game changer and lifesaver for me. I’m a big advocate for that. My life has definitely taken a big step back [with] the financial hit of going from being a dual-wage earning, professional household to one income and some disability money.
Also, during the time, my daughter was diagnosed with profound dyslexia and needed to be in a very different educational environment. I mean, we’ll never be able to retire! I don’t know. I think we’re still kind of in denial about some of that.
What is your status now?
I’m in remission.
You could call me NED if you want to — no evidence of disease. All of those things are good.
Mental, Emotional, and Sexual Impacts of Cancer
How did you manage the flux of messages and visits from supporters?
It’s really tricky to figure out. I’m a pretty open book, so I shared on Facebook. I contacted my employer and let them know.
The director of my department at the college came and my assistant came, and that was very strange. In hindsight, I would not have permitted that. I think having people see you at your lowest moment is private. I learned a lot after I had my daughter. I did not need to have my best friend in the delivery room or my mother-in-law, but you live and you learn.
I did not have that in place. I did not have someone to filter all the people coming into my orbit at that point at all. I was kind of managing that myself.
And it was it was difficult. It was hard.
In some ways, it was like reliving the diagnosis all over again every time you had to tell someone what what you had, what cancer you have, and what’s happening. Also, the leukemia journey is quite different than breast cancer journey or the treatment protocols for colon cancer or anything like that. There’s much more inpatient.
It’s much more high risk. It’s very fast moving. The thought of even getting a second opinion… it’s just not possible. I think the majority of people I was talking to — unless they were someone who was already in the medical community — were just confused. They just were perplexed. That that was difficult, and I think it did make me kind of accept my circumstance faster than I would have if I would have kept everything private.
Any advice for people on what can help maintain energy while communicating with supporters?
I think setting up some sort of a website that is private, such as Caringbridge. There’s a number of other ones out there. Your social media, calendar, your email can be really helpful as far as scheduling goes. If you would like to, you can update and have a blog. I started with that process.
It got exhausting very quickly. Some people have their spouse or a family member updating that information about you. It’s truly up to you what you would like to share.
I think for many of those websites, there’s a way to schedule food delivery, set up if you need to raise some money, or if you need someone to offer to clean your house or walk your dog.
For us, it was really helpful because we wanted to create as much normalcy for my daughter as possible. We didn’t want her just hanging out at the hospital all the time. That’s just not realistic.
Even if she really didn’t know what was going on. [She] thought it was just this fun thing to go meet all these nurses who thought she was adorable and get all dressed up to go see mom. What we were trying to create was some normalcy for her.
We used Caringbridge to make playdates [and] to request food. Being busy professionals, we often had our groceries delivered through a service before cancer came into our world. [We were] letting my coworkers who live all over the place know that would be something that would be helpful beyond just delivering us food.
We’re a little complicated. My husband’s vegan and I’m vegetarian, so many people who don’t eat that way were kind of confused as to what do I bring them?
The grocery gift cards, which could be done through email, were just absolutely wonderful because we were also dealing with a pretty quick, significant loss of income. Feeding people is important.
How did you deal with the mental struggles?
The mental health side effects are significant as well. It changes perspectives. It changes your anxiety level and all sorts of things. It’s really important to shine a light on people who are still struggling, but making their life as positive as possible.
Even if you’re stuck in bed most days of the week, if you’ve got that one day where you make an amazing dish or spend really quality time with someone who’s important to you, that’s still a life. That’s still important. You still matter.
I think that’s very, very much an important thing to center in your world — that we don’t know what’s going to happen. That’s very hard, but we’re stronger than that. We can find a way to make a new life.
How do you keep perspective?
My story is beautiful and easy compared to a number of people I know who are in their 30s and 40s and are so permanently disabled [they] will never walk again. They’re losing their sight because of transplant complications. I’m fortunate that I already had a husband and a kid.
I’ve got a friend who’s trying to figure out how to date with all of this, and it’s hard.
How did your cancer experience impact your personal relationships?
When I was initially diagnosed and again the second time, a lot of friends fell away.
Friends that I had known for years and years and years, and for many reasons that I will never know. I think for some people, it’s just difficult to face cancer if they’ve lost someone or to face a friendship that is not just getting coffee and enjoying each other’s company. It becomes much more serious.
There’s still a lot of play in my world, a lot of fun, but it became smaller. It became my mom, my husband, my daughter, and a couple close friends. Sometimes those friends would shift and change month to month, because it is really exhausting and taxing. I think to have friendships that you can in some ways find an escape from cancer.
I have people in my life that I know I’m not going to sit down with and go through all the awful things that are going on with me when they say, “How are you?” I’m going to say, “Hey, let’s talk about this book we both just read or this movie,” or, “What are you cooking?” All of those kinds of things to compartmentalize things in a healthy way.
You can also realize that you are more than cancer and that this is just a huge mountain to climb. For me to be the advocate that I needed for myself and my family, cancer was really just the be-all end-all. [It was] everything that I was focused on. Everyone was focused on it, and it was hard to take myself out of that to be able to have a regular conversation.
It felt like I was living in some sort of alternate universe, and I couldn’t connect with anyone. It took time and patience to be able to figure out how to be authentically me. Angry about cancer, advocating for myself, still being hopeful, but also having friendships that were maybe a little more surface level, and that’s okay.
There are going to be people who leave your life, and it doesn’t make any sense to dwell on that. You can be sad. You can feel those feelings but move forward. I’ve met so many amazing cancer patients, survivors, doctors, and researchers that fill that void 10 times over.
Speaking of personal relationships, what were the sexual health impacts?
Having gone through menopause in my 30s rather early, I had all of the side effects of menopause that people think about, such as hot flashes and irritability. Down the line, I suffered from vaginismus, as well as a very dry tissue.
I was able to reach out through my regular gynecologist to a special group at the University of Chicago that works with women at every stage of the cancer process dealing with sexual side effects. You can also get graft-versus-host disease of the vulva or vagina. I did not have that. That was ruled out.
Primarily, the side effects that I was experiencing are very common for people who have gone through any sort of cancer treatment, which was very dry, very irritated tissue, and to be able to engage in a successful sex life with my husband.
I needed to go through some physical therapy, which I was able to do at home using dilators and trying lots of different lubricants. My cancer was not a hormonal cancer, so I was able to use hormonal creams. It was helpful and resolved things, but it was a multi-month process to slowly introduce moisture to my body to make sure that my body didn’t poorly react to being uncomfortable, in pain, and things like that.
It took time. You have to dedicate an hour of your day to working through that. Cancer often impacts intimacy in relationships. It can take work to get it back.
For women and men who go through cancer treatment, sexual health is a part of having to work at it again. I think the message there is sometimes it takes some work to refocus on that part, but it’s important.
I’m on a patient board, and I’ve helped them with a number of their materials and spoken at conferences. I’m very open about that sexual piece of side effects from cancer, particularly for people who are in marriages where you’re used to having regular sexual activity, you’re used to going on date nights. Cancer changes a lot of that — the fatigue and side effects from treatment.
For many people, they stop having sex. They stop engaging in anything sexual for years, months, depending upon the person. You have to kind of restart that relationship and those aspects of it.
You’re probably great with your partner as far as getting dinner on the table, hopefully paying the bills, and working together with childcare. But the thing that gets cut out of many people’s relationships is that. Intimacy is what brought you together in the first place, those connections, so you really do have to reeestablish them.
For myself and my husband, it was working with a great gynecologist, who was able to help us with the fiscal aspects. It was also working with a marriage counselor to be able to reestablish a lot of those things and to resolve some of the conflicts and issues that came up mentally for us both through treatment.
What has helped uplift you most?
For me, things that were just surprisingly helpful were these close relationships — that were sometimes fraught — with family that have really grown in new ways. My mom and my husband are now very good friends, and that just makes my heart sing.
My spiritual community and my church have been very important to me in that I was very active and involved before cancer. I worked with all the youth in my Unitarian church, but now I’m not able to do that. I’m able to support in different ways and had to learn how to be supported, which was hard but necessary.
The other things that are really helpful for me have been nature and finding ways to go outside. I was stuck for so long in hospitals and in my own home. I could just walk to the park or Lake Michigan here in Chicago. It’s just unbelievably important to me to be standing outside, even if it’s with a mask and a hat. Just feeling the sun is life changing, as well as creating and making things.
I make jewelry. I paint. I write. I share my story. I think those are ways that I feel like I’m still contributing to the world. I’m still able to be part of something and make something.
In the same way, music, reading, and audio books really, really have helped bring meaning to my life. My first transplant, I was so scatterbrained, so all over the place. I could just kind of watch junk food TV, and that was about it. That gets old fast.
Especially someone like myself, who loves books and loves literary fiction and poetry and things with a million footnotes, finding audio books and very wonderful narrators the second time around just fed my brain in a different way. That was really life-giving.
How have you been able to move forward with life?
I don’t think I’ve moved on. I think that I’ve learned how to manage the uncertainty. The side effects. The future. Not knowing if things will come back, and also just acknowledging that the support system that you think you had isn’t always there. Your world gets pretty darn small sometimes.
But there’s a lot of beauty in that.
Any guidance for people on how to handle life after cancer treatment?
Going through the cancer experience, for many of us, society expects for us to go through treatment, reach remission, and everything goes back to normal.
I don’t think that’s the case for anyone who’s had a cancer story or cancer journey.
Many of us have lifelong chronic conditions. Many of us, after years of getting back to normal, will have a setback, recurrence, new cancer, or a later effect.
It’s difficult for people to understand because it’s not communicated in the media, and it’s not always supported within the cancer nonprofits in those communities. People heavily focus on that time of intensive treatment, and then you’re supposed to be done. That’s really not how it works.
What’s your overarching message to those reading your story today?
The best piece of advice that I was ever given: I asked my doctor, “Should I stop drinking coffee now that I’m a cancer patient and all of this?”
He said, ‘Absolutely not. You should continue drinking coffee and doing your morning routine because you have a new job. Your job is being an advocate for yourself.’
That I have taken to heart time after time. It really structured my world and made me realize that I’m not a victim. I am advocating for myself, and I can make a difference in my own health and the health of others.
Cancer details: Most common type of acute leukemia in adults 1st symptoms: Painful hives on legs & migraines Treatment: 3 cycles of chemo, total body radiation & stem cell transplant
Cancer details: Most common type of acute leukemia in adults 1st symptoms: Severe fatigue and excessive bleeding after oral surgery Treatment: Chemotherapy, bone marrow transplant
Cancer details: Relapsed but in remission after 2nd transplant 1st symptoms: Extreme fatigue, upset stomach, bad & persistent headaches Treatment: Chemotherapy, radiation, 2 bone marrow transplants
1st symptoms: Bruising, tiredness, shortness of breath, itching
Treatment: IV chemo, 2 stem cell transplants, targeted chemo pill
Acute Myeloid Leukemia Patient Stories on AML Diagnosis, Treatment & Side Effects Acute myeloid leukemia or AML is one type of leukemia, a cancer of the blood and bone marrow that happens when the bone marrow makes an abnormal type of white blood cell called myeloblasts, red blood cells, or platelets. It’s the most common
Sean was diagnosed with chronic lymphocytic leukemia (CLL), the most common form of adult leukemia. In this story, he shares going through a clinical trial, how cancer impacted his relationship and living with cancer as a chronic illness.
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
CLL Diagnosis
Why did you go to the hospital?
We have some really nice neighbors, and the dad had gotten sick with cancer, so I was shoveling snow for him. I have a snowblower, but it was wet and slushy, so I went out and shoveled for him. I came inside, and I said, “I pulled something in my shoulder.” I felt it while I was shoveling.
My wife said, “Which shoulder?” I told her it was my left, and she said, “You’re having a heart attack. We need to go to the hospital.”
I said, “I’m not having a heart attack. I just pulled my shoulder.” She just would not stop about the heart attack. I said, “Okay. Just so you’ll stop talking about it, we’ll go to the hospital.”
We get to the hospital, and I’m feeling so stupid. The nurse asks what’s wrong, and I explain that I pulled my shoulder, but my wife thinks I’m having a heart attack. They sent me to the ER. They gave me a bunch of tests.
Receiving the diagnosis
After waiting for all that to come back, a doctor walks in and says, “How long have you had blood cancer?”
I said, “What? What are you talking about?”
He didn’t realize I didn’t know already. He said, “No one’s been here to talk to you?”
I said, “No, you’re the first doctor I’ve seen.”
He turned white. He didn’t know what to do.
He started to explain. It was so awkward because he had no idea I didn’t know. I think he was told that the attending had come and told me, but she hadn’t yet. Maybe she got side-tracked or something. I don’t know.
He admitted me to a room. Then Dr. Roy, who is the oncologist, came and had me put into my own room. They didn’t know what kind of leukemia or what it was.
How did they figure out the subtype?
They did a bone marrow biopsy the next day. Dr. Roy came in the next day, and she told me she was almost positive it was CLL, but they needed the biopsy results to come back to be 100% certain. We got those back the next day.
For about 36 hours, I didn’t know what it was, so I was pretty scared. Once they knew it was CLL, they kept saying it was the ‘good kind.’
If you’re going to have leukemia, apparently it’s the one you want. I felt a little bit better after that.
How did the doctor tell you about the biopsy results?
Dr. Roy came in with a big smile and said, “You’ve got the good kind.” At that point, I was a little relieved, but it was all an issue for me. My son played baseball in college, and it was his senior year. He took a trip to Florida every year, and we were booked to go. It was his senior year trip, and I said, “I don’t care what kind I have; I’m going. I’m not missing this.”
She said, “Look, if you follow these precautions, you can go. When you come back, you gotta come to my office and talk.”
I had to wear a mask on the plane, I had to wipe everything down, and all that. It was a bit of a strange conversation because I knew I wasn’t going to miss his senior trip. She wound up being great about it. She was okay with it.
What’s a bone marrow biopsy like?
You always hear that it’s going to be painful and terrible, but it really wasn’t. They laid me down on my stomach. They gave me a shot to numb it. I felt nothing. I heard tapping like a woodpecker. I felt nothing, but I kept hearing the tapping.
Then the guy was like, “I can’t get the needle in. I’m on my second needle, and it won’t go in.” He decided to try the other side. They numbed that side up, tried again, and it wouldn’t go in.
They had to get a couple of nurses, and they eventually got the bone marrow out. I felt nothing.
The next day, I was a little sore. It’s like when you work out a muscle you haven’t worked in a long time, but that’s about it. People tell me they can’t believe I didn’t feel anything, but I really didn’t.
I thought the doctor had the wrong patient. He even second-guessed himself. When he realized no one had told me yet, he went pale. I was shocked, but it’s strange because then things started to fall into place and make sense.
I had been trying to lose weight, and my wife was getting so angry because it was coming off so fast. I just thought I was doing great. She doesn’t need to lose weight, but she was trying to lose a little weight, and it wasn’t coming off.
I was also getting a little bruising here and there, which I didn’t think anything of. I never put the symptoms together until I got the diagnosis, but then it all starts to make sense.
If I had never gotten the diagnosis, I probably never would’ve put it together. I probably would’ve just thought I had the best diet in the world and tried to write a book or something.
My immediate family was at the hospital with me when I got diagnosed. I didn’t let my son tell any of his coaches or anyone on the trip. I just wanted to go have a normal time for him. I didn’t want us to get treated any differently.
I got back from the trip. I went to her office, and this is when I realized she’s an angel. She said, “The only thing I can offer you is chemo.”
I said, “That’s a strange way to put that. What do you mean?”
She said, “I have a colleague named Dr. Barrientos. I used to work with her, and she had a spot open in a study. You have an appointment tomorrow at 10:00 a.m.”
She didn’t try to keep me as her own patient. She knew there was someone who could potentially treat me better, and she admitted it. I find that absolutely incredible.
The day I get the remission confirmation from Dr. Barrientos, I’m going to bring Dr. Roy like 2 dozen roses or something because she could’ve just said, “You’re my patient. It’s chemo time,” but she didn’t.
The next day, my wife and I went to the appointment with Dr. Barrientos, and I got enrolled in the study. I got the last spot in the study, and I’m the last patient in the study.
It’s venetoclax and ibrutinib. Ibrutinib came first, and then we did venetoclax. That started in April of 2018. I took the ibrutinib every morning for 3 months.
Then after the 3 months, you can start the venetoclax, which is the chemo part of it. To do that, though, you have to do what they call a ramp up. You have to be in the hospital for 3 days for 5 consecutive weeks while they up your dosage.
One of the side effects of venetoclax is tumor lysis syndrome, so they monitor you every 4 hours.
They start your fluids on Wednesday. Thursday morning, they start you on the first dose and monitor your blood every 4 hours for 24 hours. If you have no issues, they let you go home the next day.
They do the same process every week while upping the dose all the way to 400 mg. The dosage goes 20 mg, 50 mg, 100 mg, 200 mg, and then finally 400 mg. Each week, they’re monitoring the ramp up in milligrams.
I started on the 20 mg dose. I was fine, and everything was great. I went back in the next week, and we started the 50 mg. They gave it to me, and my phosphorus went through the roof. I didn’t even know what phosphorus was.
Apparently, tumor lysis syndrome comes from a rise in uric acid and in your phosphorus. They gave me allopurinol to keep my uric acid down.
I had a dangerous level of phosphorus for the trial.
The nephrologist kind of laughed because it wasn’t high enough to be of concern to them normally, but for the trial, it was too high. Dr. Barrientos was crazy on top of it, like she should’ve been.
They checked my blood every 4 hours for 4 days instead of just for 24 hours. I had to be in the hospital for 5 days that week so they could monitor me. They had me on Renagel (sevelamer) and Phoslo (calcium) to keep the phosphorus down. They finally got it down, and I got to go home.
I went back the next week for the 100 mg, and I had the same issue. It was such a battle with the phosphorus each time.
Changing diet to lower phosphorous
They had the nephrologist come in, and they said they wanted to change my diet and asked what I had been eating. I said I’d been eating so healthy and losing weight.
They asked me what I had for breakfast. I said plain oatmeal with almond milk. They said almond milk is twice as high in phosphorus than regular milk and oatmeal is incredibly high in phosphorus. I couldn’t eat that anymore.
They asked me what I’d been snacking on. I told them I’d only been snacking on raw almonds. They said nuts are incredibly high in phosphorus. Can’t do it anymore.
They asked about lunch. I’ve had the same lunch every day for 2 years. I have a peanut butter and jelly sandwich on whole grain bread. I use no-salt and no-sugar peanut butter. It tastes like crap. I use no-sugar jelly because I’m trying to lose weight.
They said I couldn’t eat peanut butter. Incredibly high in phosphorus. Couldn’t eat whole wheat bread. I had to have white bread.
They asked about dinner. I’d been eating lean hamburgers or something. Apparently, those are totally high in phosphorus too.
They seemed to have come to the conclusion that my healthy diet, which certainly might’ve been healthy in other circumstances, was packed with phosphorus and not healthy for that situation.
The problem is there’s not a diet that’s low in phosphorus that’s not high in sugar. The white bread and all that is high in sugar. All the sudden my blood sugar is up, and they ask what I’ve been eating.
We go through this round and round, and finally I’m like, “So what the hell can I eat?” This has been the battle.
Vision problems
I finally get through the venetoclax and changed my diet. I’m eating nothing but white rice, grilled chicken and grilled vegetables. I never want to see that food again, but it’s still what I’m eating.
I stayed on the phosphorus drugs. I’m not on the venetoclax full dosage at home 3 or 4 days, and my vision changes dramatically. I could see. I still had my vision, but everything was blurry. I had never had a floater before, and I had a floater.
I called Dr. Barrientos. She wanted me to come in. She sent me to the eye doctor. My baseline vision was 20/30. In under a week, it jumped to 20/60. The eye doctor said I had macular edema. I had swelling. I just wanted to know if I was going to be able to see again. I couldn’t drive. I couldn’t see the license plates in front of me. He said it was completely treatable.
Dr. Barrientos took me off the venetoclax. That was upsetting because I had done all this work to get on the venetoclax, and now I had to get off of it.
Improving vision
My eyes went from 20/60 back down to 20/40 in like 10 days. That was very reassuring, but Dr. Barrientos wanted to wait until the swelling was down all the way. The eye doctor said he had been to a conference where one of the panels was venetoclax’s effect on the eyes. He wasn’t sure the swelling would go all the way back down.
I was the first one in Dr. Barrientos’s trial who had this problem.
She finally found one article on one other patient with my issue. I had blood tests every week and had an eye doctor appointment once a month. My progress stagnated a bit, but we eventually got the blood work and vision where it needed to be.
It took a year and a month to get back in the hospital. It took that long to get back to the levels I needed to start the ramp up again. In August of 2019, I went back into the hospital.
One of the side effects of ibrutinib is that it can raise your blood pressure. I hadn’t had any of those issues, and I was ready to go back on venetoclax before August, but I started having blood pressure problems. I started on blood pressure medicine.
What other side effects did you get from the medications?
At one visit with Dr. Barrientos, I went to sit up after an EKG and got really dizzy. She told me I had to go back to the hospital. They diagnosed me with what they thought was vertigo. They ran all kinds of tests.
During the CT scans that are required for the surgery, they found a small mass on my pituitary. They did a scan at the beginning. They didn’t notice it on the first scan, but they noticed it on one of the later scans. It hadn’t changed since the first scan. She put me on a drug I can’t pronounce. One of the side effects was dizziness.
I stopped taking the drug that was meant to shrink the little mass on the pituitary. I felt better. That’s when I was finally ready to try the ramp up again.
At present, the only side effect I experience is being tired. The venetoclax can kind of knock it out of you, but it’s not bad. That’s really the only lasting side effect I experience.
How did the ramp up go the second time?
I had zero problems with the first week. We talked about doing the second week outpatient. We decided to go ahead and do it inpatient just to be safe. I did all 5 weeks, and I didn’t have any issues. I didn’t eat the hospital food. I stayed on my changed diet.
I’ve been on the venetoclax ever since, with no blurry vision or anything. Everything is going great. Everyone should see Dr. Barrientos. She is on top of everything. It took a while to get everything fine tuned, but it’s all going well.
They haven’t figured out why I had such a hard time compared to the other trial patients, but they’ve pretty much decided it was because my original healthy diet was too high in phosphorus.
What do you do through the clinical trial period?
I’m getting blood work done once a month. I have a bone marrow biopsy and a CT scan scheduled (in 6 months). They’re required for the trial. Again, at the end of the trial in June, they’ll do another biopsy and scan. That’s when I’ll be able to hear them say I’m officially in remission.
She can’t say remission until I finish the full trial protocol and bone marrow biopsy. All my numbers look great right now. Everything is going in the right direction. If I went to get life insurance and they took my blood, they wouldn’t know I had CLL unless I told them.
What are the next steps after the trial?
It’s remission. Beyond that, that’s the part of the trial they don’t know yet. They don’t know how long people from the trial are going to be in remission. It could be a year, 5 years or forever. They don’t know.
At that point, I’ll do blood tests every 3 months with Dr. Barrientos to see how things are going.
If it comes back, we’ll just treat it accordingly. If I ever need the trial drugs again, they’re provided to me for free for the rest of my life. That was part of the trial, which is great because they’re 15 grand a month for the drug.
Why did you choose to go on a clinical trial?
My mom had ovarian cancer a couple of years ago. She was older, but the chemo just destroyed her.
For the 4 or 5 days after, she was just out of commission. I didn’t want to go through that. I thought if there was a way to avoid that, I wanted to.
If the trial didn’t work, I always had chemo as an option, but once I had chemo there was no going back. I wanted to give the trial a try.
I trusted Dr. Roy. I have a really close friend who has a sister that’s a nurse at Sloan Kettering. I called and asked if they could ask the sister who I should see. She called me herself, and she said, “It’s not someone at Sloan. It’s Dr. Rai at Northwell.”
That’s the doctor who Dr. Barrientos works with. It’s Dr. Rai’s office that I go to. I told her, “Wow, it’s crazy that you’re telling me this because that’s the doctor I’ve already gone to see.” It just made me feel so good about my decision.
Helping patients in the future
I experienced immense frustration at a certain point because of all the complications. I was never mad at the study or Dr. Barrientos.
Other than that, nothing really threw me for a loop. The vision stuff was scary. Nothing has thrown me for a loop or been too much to handle, but it’s definitely been frustrating at times.
I’ve had some friends and coworkers say I’m a guinea pig. I say, “Yeah, I am. That’s what I signed up for.” They’ll ask, “Well, are they more interested in getting their information, or are they interested in you?” I’ve never ever once felt for a second that they were not interested in me.
I’m sure they’re very thrilled to have all the information they got from me and my complications, but they’ve never once made it feel like they were learning at my expense.
I think about the people who came before me in earlier phases of the trial. Some people died from tumor lysis syndrome. Some people died from the blood pressure issues because they didn’t know it could raise it too high.
Think of how they helped the people after them. Think of how they helped me. Now I can be that for the next people who need these drugs. If I can do something to help someone after me, I think that’s great.
What advice do you have for other patients about clinical trials?
I would say 100% go for it. Do you research and make sure it’s the right one for you, but go for it.
Could I have been done in 6 weeks with chemo? Sure, but I would’ve had to have done chemo. I didn’t want to do that. Again, think about the information that my frustration and experience is going to provide.
For example, Dr. Barrientos did a lecture for the Leukemia & Lymphoma Society in Manhattan, and I went to hear her speak. She’s so impressive. She’s unbelievable. My wife and I went, and the room was packed.
The questions she was asked were amazing. Her knowledge is just incredible. She gave her presentation, which was great, but the questions got me. She knows the slides, but she didn’t know what the questions would be. We sat in awe watching her answer these complicated questions with such skill.
The point is, though, there were 5 patients at that lecture who had the eye issue I had. 5. Not only did they have the issue, but their doctors had no idea what to do with the eye issue and had no idea it even existed.
After the lecture, I gave all the patients the information Dr. Barrientos gave me.
I emailed them, and they emailed their doctors. Some of them contacted Dr. Barrientos. My issue with my eyes was scary, but when you share it with other areas, there were other people out there.
Now, these other people are going to know how to treat this issue because of me, my experience and Dr. Barrientos’s help.
Creating a win-win for patients and doctors
That’s the kind of information that’s so invaluable to the doctors. I’m allowed the opportunity to not have chemo and still achieve remission, and the doctors are getting the information from my experience to help other people. It’s a win-win all the way.
It’s frustrating, and it’s a longer process than the chemo probably would’ve been, but even after knowing everything I went through, I’d do it again. I wouldn’t change a thing.
I was worried they were going to throw me out of the trial. Dr. Barrientos fought like hell for me and kept me in.
Reflections
How did the experience affect your relationship with your wife?
I’ve tried to just be status quo like nothing has changed. I’m sure I’ve fallen short, but I’ve tried to just be the same old me through this. My wife and my kids have been so supportive of me through the whole thing.
I would say it’s probably made us closer. My daughter has said that she thinks this whole thing has made the family closer.
My wife gets anxious sometimes, but I try to talk about something else when she’s feeling that way. I just try to show her that I’m okay, and everything will be okay.
I don’t think my case is like most people. Not that the cancer part is different. That’s the same, but I’ve never felt sick. I’m sitting in a hospital room watching TV or surfing the internet on my laptop. I’ve always felt fine. It’s been strange. I’ve never considered myself “sick.”
I just think of this as something that I have, and we’re treating it. I think maybe if I didn’t feel well, it would be a different story.
It’s not hard to remember I have cancer, but it definitely is weird. I’ll go do something and be exhausted. I’ll be like, “Why am I so tired?” Then I remember, “Oh, right. I have cancer.” Those moments are when I think about it for a second, but usually I just try to be me.
Every morning, when you pull out 8 pills that you have to take, that sucks, but it is what it is.
What advice do you have for someone who has just been diagnosed with CLL?
Get the proper doctor. If you can get Dr. Barrientos, no matter where you are, do it. Even if it’s just a consult, I would do it. She has a patient who flies in from Wisconsin to New York just to see her.
It sounds crazy because it’s cancer, but with CLL, don’t worry. It sucks. It sucks to have it. It sucks to say you have cancer. If you do get cancer and it’s CLL, just know you have the ‘good kind.’ Don’t worry.
Get it diagnosed. Get it taken care of. Get the right doctor. Make sure you’re on a regimen that you’re comfortable with. The ibrutinib and venetoclax is the gold standard right now, so if you don’t have a doctor that is going to at least explore that, find someone else. It’s a wonder cocktail. It’s absolutely amazing.