My name is Dr. Nina Shah and I’m a professor of clinical medicine at the University of California, San Francisco, or UCSF. That’s where I focus mainly on multiple myeloma clinically.
That’s what I see in my clinic, but on the inpatient side, we see everything including leukemia and lymphoma. I’m particularly interested in immunotherapy, as it relates to multiple myeloma and cellular therapy.
This would include things like chimeric antigen receptor T-cells, or CAR T-cells, as well as natural killer cells, dendritic cell vaccines, antibodies, and T-cell engagers. All those exciting immunotherapies that are coming down the line.
I also have a secondary interest in patient experience, including quality of life, patient-reported outcomes, and some life coaching applications that we’re trying to use to improve patient experience.
Understanding Multiple Myeloma
What is multiple myeloma in human terms?
Multiple myeloma is a cancer of a cell called plasma cell. A plasma cell is part of your immune system. Normally your immune system is made to fight viruses and bacteria and one of its soldiers is called a plasma cell.
Particularly, plasma cells are supposed to produce antibodies, which we’ve heard a lot about recently. COVID antibodies, antibodies to zoster, all these things.
These antibodies are proteins that help you fight and tag bad things so your immune system can know to kill those things.
In the case of multiple myeloma, one of these plasma cells goes haywire. It grows out of proportion to the other cells, and that’s really the definition of cancer.
When one cell gets selfish and replicates its own clone, it takes up the resources of the other cells. That’s what happens in multiple myeloma.
One plasma cell grows and it starts taking up the space in the bone marrow. It starts producing a protein that eats the bone around it and that’s why people can have holes in their bones, or lytic lesions.
Then the protein that it produces—that antibody is now one antibody. It’s not a variety of antibodies. It’s just that one clone.
That’s why you will often hear the term monoclonal protein or monoclonal or clonal protein, M protein. That’s something that we can use to measure how many plasma cells there are.
It’s like the petals on the flower; the more petals you see around, the more you know they have flowers and that’s what we often use to measure in the blood.
The proteins that are produced from these cells can be in such high quantities that they also can have detrimental effects. That’s why some people with myeloma will say, “Well, my light chains were really up.”
That’s part of that M protein, those antibodies, and they can clog up the kidneys.
You hear about multiple myeloma as a disease that affects almost every part of the body—the bones, the kidneys, the blood system, and it all comes from having this one immune cell get a little out of whack. It’s supposed to help you, but in this case, it’s harming you.
What are the chances of it relapsing or being refractory
Unfortunately, multiple myeloma is considered an incurable disease, but it is a disease that one person can live with for a very long time.
We have patients who’ve lived 10, 15 years with it. It really depends on where that myeloma is going and what it’s like.
Sometimes we can predict that and sometimes we can’t, but on average, our standard myeloma patients are living longer than 10 years, at least, because we have new therapies.
What I tell all myeloma patients I meet is that, “You’ve been newly diagnosed and we’re starting therapy on you. We’re hoping that we can stretch out this time as long as possible so that we can have this first remission, meaning the first time you have a response that lasts as long as possible so that you don’t have to worry about it and you get back to your life and start being a person and not a patient.”
First Line Treatment
First line of myeloma treatment
For anybody who’s been newly diagnosed with multiple myeloma, it is very overwhelming because there’s a lot of information about what this disease is, then what is your life going to look like, what treatments are there and how can you predict what’s going to happen to you.
Those are all unknowns and if we had a crystal ball, of course we would be able to tell you as best as we could, but we often don’t know.
Combination (induction) therapy
What I usually tell the patients is that we’ll start off with some combination therapy. This is called induction therapy, and it’s usually a three-drug combination.
The backbone of that usually is some steroids, like dexamethasone, the drug everyone loves to hate, and then two other drugs. We usually combine those three drugs and we give them for three or four-week cycles. Those are pockets of time.
VRd induction therapy
There can be a variety of choices that we may give upfront, and this is really dependent on what the physician’s style is. The standard treatment is VRd, or Velcade or bortezomib (they’re the same thing), Revlimid or lenalidomide, and dexamethasone.
VRd side effects and management
bortezomib (Velcade) side effects: neuropathy or numbness in hands and feet
lenalidomide (Revlimid): fatigue, diarrhea
dexamethasone: energy level changes
The major side effects from the bortezomib or Velcade are potential neuropathy, or numbness, tingling, and a weird sensation in your hands and feet. A lot of times patients will say it’s worse at night.
We’ve tried to get around this by changing the dosing schedule and doing it weekly instead of twice weekly, although it was originally approved in a twice-weekly fashion. Sometimes, for older patients, we may reduce the dose.
The Revlimid often can make patients experience fatigue or diarrhea, but it’s generally well-tolerated when you do it upfront and when newly diagnosed. I would say more of the Revlimid symptoms happen after the transplant.
The dexamethasone can make you nutty. It’s like people are cleaning up their house all day long on the first day, and then on the second day, they crash. Their spouses now avoid the dexamethasone day.
Alternatives
There are other alternatives to the first one. Sometimes instead of using Velcade or bortezomib, we’ll use a drug called carfilzomib. This also works in the same mechanism of action, but has been studied in later lines. It’s also a very effective drug that has another side effect. It affects the blood pressure and has potential slight effects on the heart.
For example, if a patient comes to me and they’re healthy, except they have diabetes and they have really bad neuropathy from their diabetes, maybe a better choice for them would be the carfilzomib and not the bortezomib with Kyprolis and not Velcade, as their trade names.
That’s how we go about thinking about the side effects of these therapies.
High-dose chemotherapy and autologous stem cell transplant
After several cycles, if you’re healthy enough, we often would take you to a high-dose chemotherapy autologous transplant, or just transplant for short.
Stem cell transplant is what I would consider to be part of the standard of care for newly diagnosed multiple myeloma patients. You may not hear that from every doctor, but I like to do transplants.
The reason for that is that while those three drugs at the upfront, the Velcade, Revlimid, and dexamethasone, are like the soap and sponge for cleaning a dirty pot.
But the melphalan, which is the transplant drug, is the Brillo pad. It really digs in and gets the deep myeloma cells that you couldn’t get. It’s another way of being smarter than the myeloma.
This process involves two things. Since we can’t give you a very high dose of chemotherapy without damaging normal cells, before we even give that dose of chemotherapy, we have first to collect blood stem cells so that your blood will recover from having that dose of chemotherapy.
We always initially do a stem cell collection. This is an outpatient procedure and can take about a few days. We put a big catheter, usually in your chest wall, or a big IV in your arm. Then we take out a bunch of blood and filter out those stem cells after having given you some medication to get those to your blood.
Usually about a week for it between the injections and the procedure. Then after that, we do part two, which is the actual transplant. That’s when patients are, in our case, admitted to the hospital, although you can do it as an outpatient.
They get one dose of this chemotherapy. Two days later, they get replaced with those stem cells. We thaw them and give them just like a blood transfusion; it’s pretty anticlimactic.
For the next two weeks or so, these patients recover from these traditional chemotherapy yucky side effects:
nausea
vomiting
diarrhea
hair loss
infections.
Of course, they need transfusions because we’ve completely obliterated the blood system and we have to take time for those stem cells that we gave to come back and grow and repopulate.
That’s the time that you’ll feel those traditional chemotherapy side effects that are less present with the newer Velcade, ReV/Dex.
Those are the new chemos, but this is like the old-school chemo. It does its job because we know that patients who get transplants early and get it upfront as a planned procedure actually do better as far as how long their disease is in control.
Maintenance therapy
After that people would generally go on to maintenance therapy, which right now is just one pill of low-dose lenalidomide, also known as Revlimid.
That pill and that factor can go on for five years or as long as they can tolerate the revlimid. It’s not always easy to tolerate it, but most of my patients can tolerate some of it.
You can go back to work, go back to having a life, go back to their family life.
As far as understanding what they should know and what they should ask their doctors, it’s important to know what kind of myeloma you have because you want to be able to follow your own labs.
Being able to follow your own labs when you get them is an empowering thing.
Sometimes it’s an anxiety-provoking thing, but I find in general it’s empowering because you and your doctor can have a really good conversation about trends and where things are going.
You feel like you’re really a part of the decision-making, which you always should be.
The second thing is that it’s important to know what your cytogenetics or FISH studies are. These are DNA characteristics of the myeloma cells and how those myeloma cells are prone to grow or not grow based on what we find in these studies. That can help us determine the risk.
When we talk about risk, it’s how aggressive the myeloma really is, how likely it is to come back sooner than later. These are all parts of the discussion that are important to have with your doctor at the time.
There’s also other parts of discussion you want to have like supportive care. Other things you should be doing, for example, to make your bones stronger and to make you stronger to go through this process.
Higher risk versus standard risk
When we think about high risk versus standard risk in general, that means the malignancy is more aggressive.
In the case of multiple myeloma, high risk is defined by factors like a staging criteria. This staging criteria is called the revised ISS (international staging system). We use the beta 2 microglobulin and the DNA characteristics as well as LDH to determine. That’s a lab value that’s often overlooked, but is useful to help us figure out how myeloma cells like to grow.
Then there’s what we call cytogenetic risk. These are very specific findings in the DNA studies, you’ll see most commonly called cytogenetics or FISH. That’s a short term to talk about how these pieces of DNA look.
When we find things like 17p deletion, or deletion 17p, or translocations, that’s when two pieces of DNA break off and hook back up with each other. You may see that there’s a piece of 11 with a piece of 14 or a piece of chromosome 14 with a piece of chromosome 16.
We often see that there are some patterns of high-risk cytogenetic or FISH findings. Then we can say to the patient, “Your myeloma cells are getting a genetic signal that tells them to grow,” or, “They’re not getting a signal that tells them to stop growing.”
Then we know that those patients may have more aggressive disease. That’s what we talk about risk—either by disease burden or by what propensity or likelihood it is for these cells to grow.
Is it standard that doctors pursue these tests
Thankfully, we have grown a majority over the past 10 years and it’s almost always standard. In fact, I can’t remember the last time I didn’t have a bone marrow test that had this. At least FISH is sent, sometimes cytogenetics. They’re two sides of the coin. It is very critical that it is sent.
Even for patients who may have had a biopsy done, for example, on a bone in their back, because there was something that was biopsied by a neurosurgeon that turned out to be consistent with myeloma.
I still insist on FISH being run either on that specimen if it’s possible, or repeating with the bone marrow biopsy. It is so critical to get that DNA information.
Describe how you manage the treatment decision-making process with patients
It’s really important for the doctor and the patient to be partners in this process. It must also involve the caregivers because they’re part of the story too.
What I do is I try to give the patient background information so they can understand the pathophysiology. It makes them understand what’s happening in their bodies. Then we talk about what to consider when picking one treatment over the other.
A lot of times treatment decisions are based on what the patient himself or herself looks like. Some people may have kidney dysfunction, some may be older and frailer. Some people may have preexisting conditions like diabetes, et cetera. This information helps us to understand what treatment will do the least harm.
Many of these treatments do equal good, but we want to do the least harm.
It’s really important for me to know a patient’s medical history and what are the symptoms that he or she has. I can understand what would be a good fit for treatments and I can explain that to the patient.
Oftentimes, the patient and I, having spoken about their symptoms and some of their medical history, can come to an agreement based on the choices.
It’s hard because sometimes you don’t want to ask for recommendations that you don’t plan on taking. But you should always feel free to do that because it’s our job to give you the choices that exist and make recommendations.
Ultimately, you have to be okay with the path going forward.
Newer Multiple Myeloma Treatments
Proteasome Inhibitors
It’s a very interesting thing that the proteasome inhibitors exist at all, because it’s one of the few times where you can take advantage of something going wrong in the cancer cell.
The myeloma cells—the plasma cells—love to make proteins. They make that one antibody which is a real problematic thing, but it is a way for us to measure it. Because of that, their protein machinery is on overdrive.
The proteasome inhibitors work by irritating the garbage disposal of fat protein machinery. That then makes the cell extremely mad and it makes it die because it can’t get rid of all its waste.
That’s why these proteasome inhibitors are particularly good for myeloma cells because those cells produce a lot of protein. You generally hear about these drugs specifically for multiple myeloma.
New CAR-T-cell therapy
This is the BCMA-directed CAR-T-cell therapy and idecabtagene vicleucel or ide-cel. The trade name is ABECMA. You can look at any of those, we call it bb2121. Everything has five names.
It’s a way to take a patient’s own T-cells and genetically engineer them so that they will express a protein on the surface. That protein will specifically target a protein on the myeloma cell that’s called BCMA. It stands for B-cell maturation antigen and it happens to be a very specific protein that is on the surface of the myeloma cells.
These T-cells are engineered to recognize specifically that protein and those T-cells see the myeloma cells and they think, “Oh, you’re an infection, I better kill you.” That’s what they do. We take advantage of the T-cell ability to kill things that they consider foreign and these T-cells will bind to these BCMA plasma cells and kill them.
That’s what’s so exciting about it—it’s taking your own immune system and repurposing it to do its job of killing its myeloma cells.
This product was FDA-approved just this March of 2021. We’re very excited to start rolling in our clinic to make this available for patients as a standard of care after having received four prior lines of therapy.
Abecma side effects and management that you have to offer to patients and caregiver
Acutely, Cytokine Release Syndrome, or CRS, does happen and is like the worst flu you ever had. It’s appropriate because your T-cells are having a party with all the myeloma cells and that’s good. That means the T-cells are trying to fight the myeloma cells as they would any infection.
You do have fever and potentially lower blood pressure. Over 84% of patients had this in the pivotal trial, but very low grade, manageable with a drug called tocilizumab. It usually happens within the first day or so of getting these cells for Abecma. After that, it’s boring in the hospital thereafter, which is good.
There’s also an 18% chance of having neurotoxicity or confusion that’s also very treatable with steroids. After the first two weeks, it’s actually much better.
There is fatigue and some low blood counts, but we’ve just had an analysis of primary and secondary quality of life measures.
It showed that over time, going from time zero all the way to 6, 9, and 12 months, patients actually had improved quality of life with decreased pain and fatigue, and increased emotional and social functioning. This is very important in maintaining who you are, not just what you are as a patient.
Patient Response
The pivotal KarMMa study, which is the study that ultimately got this product approved, had patients with very heavily pre-treated myeloma. Median, so at least half the patients, had six prior lines of therapy. That’s a lot of therapy that people have had.
Usually, drugs get approved by the FDA for myeloma with a 30% response rate. That’s the bar, but here you have something with a 70% response rate and it’s actually upwards of over 80%, for the actual dose level that has been recommended to go forward. We think we can get 8 out of 10 people to respond, hopefully.
For those people, they can have a year without getting any therapy. Again, the progression pre-survival for most drugs with FDA approval in this setting is like two, three months. It’s not very long at all. To get 12 months a year without any other therapy is something that we’re looking forward to because our patients definitely want a break. They’d love to see our faces, but maybe not at the chemo suite.
This is something that is unprecedented, but we’re hoping that we can even improve upon this with future products.
Wave of Therapies
I think what we’re going to see now is this wave of T-cell therapy and immune therapy, which includes bispecific T-cell engagers (BiTEs). Those are like antibodies, but they engage T-cells and these are really exciting drugs.
Both of these are going through a lot more clinical trials. Although we have one product approved for T-cells, we have another one coming down the line, and we have to also alginate, which would be off-the-shelf T-cells, so patients don’t have to go through a T-cell collection. That will be coming down the line, not this year or next year, but soon.
In a concurrent way, we’re also going to have these T-cell engagers, which are not cell therapies. They’re actual drugs but they’re off-the-shelf drugs that can be given. The first dose or two needs to be given maybe in a hospital or monitored setting, but after that, it’s very well-tolerated. People will be able to receive this at their local oncologist’s office.
As we get more data for all of these drugs and understand safety and what’s best for treating patients, these will hopefully get FDA approved. There are already ongoing clinical trials to look at these agents, including the CAR-T cells in earlier lines of therapy, so we don’t have to wait for people to be on their fifth line of therapy to reap the benefits from this particular treatment.
Clinical trials enrollment process
If they want to set up a consultation, they can get to our new patient consult service and we try to see everybody within a week or two. Especially now with Zoom, it’s much easier. We can plug them in and we’re starting a queue now for people to get ready for this treatment.
At first, there will be a big line of people because we have people waiting and have been waiting for a year now, but we’re hoping that as 2021 rolls out, we’ll have a better way to space everybody.
Soon, we’ll be able to be in line as patients have relapsed disease, taking them and quickly getting them set up for Abecma.
We are all limited by the same human things: time, cells, mutations, everything. I think this journey is one that has to be a journey of partnership between the provider and the patient.
It’s not anyone talking to you. It should be you having a conversation with your provider. The more that each of you is educated—and I get plenty of education from my patients—helps us understand each other better and ultimately make a better integrated and informed decision for your care path going forward.
Role: Hematologist-Oncologist Focus: chronic lymphocytic leukemia (CLL) & leukemia and lymphoma | CAR T, targeted therapy Provider: Medical College of Wisconsin
...
Role: Clinical investigator and professor of hematological oncology Focus: Multiple myeloma, Waldenström’s Macroglobulinemia, early screening, clinical trials Provider:Dana-Farber Cancer Institute (Boston)
...
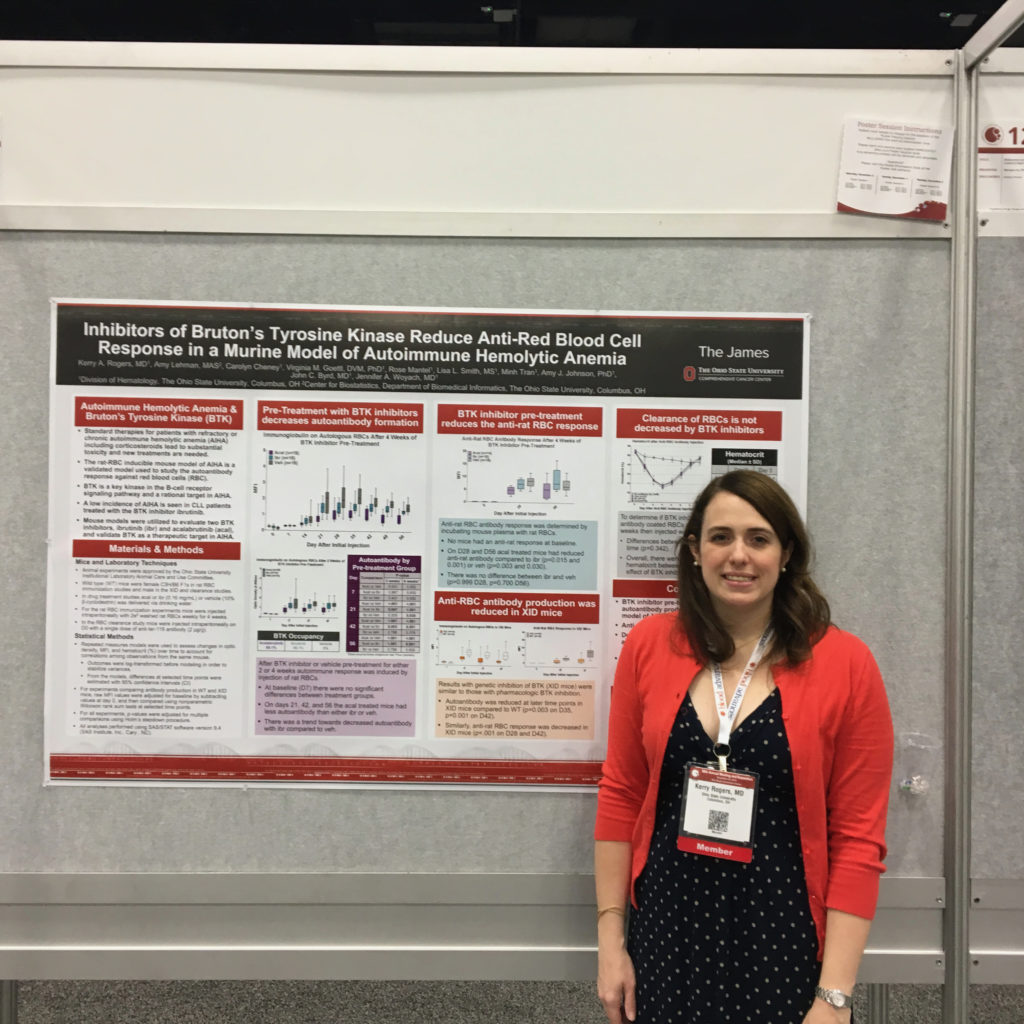
Lending her vast expertise and research experience as an assistant professor in the Division of Hematology at The Ohio State University (OSUCCC – James), specializing in chronic lymphocytic leukemia (CLL) and hairy cell leukemia (HCL), Dr. Rogers sheds light on participating in clinical trials and the community’s efforts to move the mark in the standard of care.
Explore below for Dr. Rogers’ insights on everything from the latest in CLL treatment, decision making throughout treatment, importance, and prospects of clinical trials. Full written version below the video.
I currently live in Columbus, Ohio, and I’m from the Midwest, but I grew up in the Chicago area.
I have a guinea pig, and I like college football. That’s huge at the Ohio State University, but I did my residency at the University of Michigan.
Don’t tell anyone, but I went to Northwestern for an undergrad, so that’s really my football team. That’s just a bit of me.
I work at The James (OSUCCC), and I enjoy taking care of people with chronic lymphocytic leukemia (CLL) and hairy cell leukemia (HCL).
My major interest academically is on improving targeted agents for the treatment of both these diseases.
Chronic Lymphocytic Leukemia (CLL)
What is CLL
Chronic lymphocytic leukemia or CLL is a blood cancer. It’s a cancer of cells called B lymphocytes. Don’t ask me why they’re called B lymphocytes! Those are white blood cells or immune system cells that have turned into cancer cells at some point over their lifespans.
They can go anywhere in the body that the blood goes to—you can find them in the bone marrow, lymph nodes, liver, and spleen, and in the blood, because it’s leukemia.
You can make a CLL diagnosis when there’s a certain number of these leukemic white blood cells or CLL cells in the blood. You can diagnose it with a blood test, and the most common way these days that people come to be diagnosed with CLL is when their white blood count appears too high and then goes through blood tests.
Many people diagnosed have no symptoms whatsoever and are sometimes somewhat confused about going to the cancer hospital to meet with me.
When thinking about CLL, it’s also important to realize that this is the most prevalent adult leukemia, meaning more adults live with CLL than any other type of leukemia.
People with CLL can expect to live a very long time, including their natural lifespan, and not everyone needs treatment. Because of that, it’s imperative to think about how well people are going to live with their CLL.
Categories and Stages of CLL
Unlike solid tumors like breast cancer or lung cancer, where the staging is based on how far it’s spread in the body, and if it’s left the site where it developed, which could mean the patient is in big trouble, we stage these blood cancers differently. Since they go over where the blood goes, which is everywhere, we can’t use the same basis.
In the United States, the most common staging for CLL is called Rai Staging. It was developed by Dr. Rai, a very nice man if you ever get the chance to meet him.
Rai Staging
Stage 0: CLL cells are in the blood
Stage 1: CLL cells are in large lymph nodes
Stage 2: An enlarged liver or spleen from CLL
Stages3 & 4: CLL cells are on the bone marrow that has caused people to have low hemoglobin, be anemic, or have a low platelet count from the CLL
How is CLL staged?
It’s staged simply by physical exam and looking at blood counts, and many people don’t need a bone marrow biopsy for staging. Some people need it to know why people’s blood counts are low, but it’s not always necessary.
The other part was the main forms of CLL and if there’s a slow-growing or a fast-growing type.
Everybody’s a little bit different. You’ll see some people diagnosed with CLL, and they’ve had it longer than I’ve been a doctor, and they’re doing fine with it. Their white count is the same as it has been for the last couple of decades.
But there are people whose CLL isn’t moving very fast at all. Then, some were diagnosed 18 months ago, and their white count has gone from 15 to 200 over that time.
Tests for CLL
The course of the disease can be quite different in many cases, and there are some tests that we can do to help better estimate if it’s going to be a slower or faster-growing CLL.
IgHV mutational status
One of those tests is called IgHV mutational status, or immunoglobulin heavy chain gene mutational status, where unmutated usually means a faster-growing, higher risk CLL.
I’d like to think of mutated as a special, low-risk slow-growing CLL, and that’s mutating your immunoglobulin as a normal process in B cells. This just says whether or not the CLL cells did that before they turned into leukemia cells.
FISH test for CLL
Some other tests that can help include FISH panel testing, which is just a fancy way to look at chromosomes in the CLL cells, not like the ones you pass onto your kid.
Things like deletion of the short arm of chromosome 17 or deletion of 17p can mean that we’d expect the CLL to be faster-growing, and deletion of 13q, which is part of the 13th chromosome, predicts slow-growing.
We can use a combination of these factors to guess how someone’s CLL will do.
Of course, sometimes we’re surprised. Sometimes, it looks like it will be slow-growing and it’s not, or people with some high-risk features really have an extended course but their CLL isn’t causing them any issues.
CLL in layman’s terms
One thing that really helps people that’s not necessarily fancy is knowing how to look at your own blood counts.
People get these complete blood counts all the time, and you’ll see your white blood cell (WBC) count, hemoglobin, platelets, and then below that, you’ll see a differential that tells you what type of white blood cells those are.
You always want to look at the lymphocyte count, because the CLL cells are counted under lymphocytes.
The other testing is something you do just on the leukemia cells.
It’s always very important to ask if this testing is done and what the results are so that you can know more about your CLL.
It helps you predict how much trouble you might have from the CLL in the future, the time before needing treatment, help in selecting a better course of treatment, how many treatments you might need in your lifespan, or if, at some point, a clinical trial might be appropriate for you.
The major ones are the IgHV and CLL FISH panel, which stands for fluorescence in situ hybridization. It is a chromosome analysis where they look at all the chromosomes because people with three or more changes in their chromosomes actually predict a higher risk of CLL.
They can expect to have more treatment and more difficulty with it in their lifetime. People with normal karyotype, like normal chromosomes, actually expect to have less difficulty.
First, it’s important to realize that the median age that people are diagnosed with CLL is in the mid-60s or almost 70. There’s a lot of older people who might have other health conditions.
It’s always important to think about what other health conditions someone has when planning treatment.
It has been a goal in the field of CLL medicine for a long time to make sure that some treatments are appropriate even for older people in their 80’s or even 90’s with other health conditions.
But here, I’m going to talk about more of the chemotherapy for younger, fit people because I think it’ll be easier to understand in that setting.
We’ve always had some chemotherapies that could lower the white count or improve symptoms. But the mark was moved on how long people are living with CLL or survival by combinations of chemotherapies with an antibody medication called rituximab.
Fludarabine, cyclophosphamide, rituximab (FCR)
The last several decades before my time working in CLL were spent developing a regimen called FCR (fludarabine, cyclophosphamide, and rituximab). Rituximab is the antibody and the other two are chemotherapies.
Bendamustine and rituximab
There’s a similar regimen you can use in people who might be slightly less able to tolerate chemotherapy called bendamustine and rituximab. These are highly effective chemotherapies that could be given to most reasonably healthy people and can control the CLL for years.
Targeted Therapy
ibrutinib and venetoclax
It’s important to know that as a first treatment, our new targeted agents, like ibrutinib and venetoclax-based treatments, were compared to these chemotherapies and had longer progression-free survival. This is a measure of how long people are alive without their leukemia returning.
We have found that these targeted agents were actually better than these chemotherapies.
That means people lived longer without their CLL coming back after they took the non-chemotherapy targeted agents. Also, they have a different group of side effects that are generally better than chemotherapy.
Choosing between Chemotherapy and Targeted Therapy
Some people choose to get chemotherapy because it’s different from these targeted agents, or they might have a health condition that makes the targeted agents inappropriate.
These days, the vast majority of CLL patients should be receiving treatment with a targeted agent and not with chemotherapy.
It’s very uncommon that you’d have to use chemotherapy to treat CLL. The one exception to that is young fit patients. IgHV mutated people and don’t have a high-risk feature such as deletion 17p can have 10 years or more of being alive with no detectable leukemia after getting FCR.
A group of younger people fit for chemotherapy treatment are those mutated and don’t have deletion 17p, called a TP53 mutation. But they might choose to get FCR because it might actually cure them.
I don’t know what else to call 10 years of being alive without detectable leukemia. We don’t usually say CLL is curable, but this is the one case where it might be.
However, there’s a lot of risks to doing FCR, like getting a different type of leukemia called acute myeloid leukemia (AML). That happens down the road due to bone marrow damage from FCR.
That is the one case where it could be very important to offer chemotherapy, especially to young healthy people that might want to do a treatment course of about six months and then potentially never need treatment again in their lifespan.
It’s not a guarantee that they’ll never have leukemia come back, but that is the one case where it’s important to think about it. But for the vast majority of other people, targeted agents are safer and more effective.
How long have the targeted agents been in use
The BTK inhibitors were developed in the last decade, and venetoclax shortly on the heels of that. When things are through phase III studies, that’s when they start being prescribed more commonly.
We—the academic centers—get to use all these drugs and people that come see us here might benefit from taking them as a participant in a clinical trial.
I’ve seen many people who did really well doing a research study to get a newer drug that later became approved. This becomes more widely available and used by general practice, hematologists, oncologists after phase III studies.
Continuous novel agent therapy vs. time-limited
For previously treated or relapsed refractory CLL once, it’s been about five years. In 2018, we had those randomized phase III studies comparing ibrutinib regimens to FCR or BR reported that ibrutinib had a longer progression-free survival, which is, again, being alive without leukemia. That really put those in very widespread use.
There is some resistance to it just because you have to take the pills for a long time. You take them indefinitely until either leukemia comes back while you’re taking them, you develop a side effect and have to stop taking them, or you have some other health condition that you have to stop.
In younger patients, compared to FCR, ibrutinib even had a survival advantage, meaning you’re more likely to be alive if you took the pills instead of FCR.
When you explain to them that, yes, it is not the first choice, most people decide that that’s better than something that has a shorter progression-free survival or doesn’t work as well.
Most people are more comfortable taking pills long term when they find out that it works better than chemotherapy.
In both people who have taken a treatment before or selecting a first treatment, there are two major standard of care options outside of a clinical trial.
Although I think participating in clinical trials is always something to consider if you can do it. I’ve seen a lot of people benefit from that. You won’t get a placebo without knowing that’s an option. From where I work, we have zero CLL trials with a placebo.
Treatment for relapsed/refractory (R/R) CLL
The two standard options are both highly effective. If patients haven’t taken either class of drugs, they’re both excellent, and you can pick based on preferences and side effects.
BTK inhibitors
There are BTK inhibitors, which are pills that target a protein called BTK. This blocks a cell signaling pathway called B cell receptor signaling. This makes the CLL cells not behave like CLL cells and die off over time.
The two main BTK inhibitors that are approved for CLL are ibrutinib and acalabrutinib. Ibrutinib is a once-daily pill. Acalabrutinib is more selective and targets pure things that ibrutinib does. It is a twice-daily pill.
Ibrutinib and acalabrutinib are both excellent options. They’re usually given by themselves, although they can be given with an antibody medication in some cases.
Venetoclax
The other option is another oral targeted agent called venetoclax. It inhibits a protein called Bcl-2, which is an anti-cell death protein. If you block an anti-cell death protein, that’s like a double negative, and it kills the CLL cells really fast.
The problem with this drug is that it has to be started slowly so people can be monitored. It can work so quickly that it can cause tumor lysis syndrome. It is usually given with an antibody and requires monitoring.
Venetoclax treatments are given in a shorter duration. If people are taking it as a first treatment, you give it with an antibody called obinutuzumab and take it for one year. If you’re giving it after people have already gotten treatment, you usually give it with an antibody called rituximab, and you take it for two years.
It’s whether or not they’ve taken treatment before it determines whether or not you take venetoclax for one or two years.
Venetoclax vs. BTK inhibitors
Venetoclax is like a time-limited treatment versus BTK inhibitors, which you take indefinitely till they stop working or you develop side effects and have to quit.
Some people have very strong feelings about if they want to take something and just get it done and stop, or if they’re just fine adding another pill to their pillbox. They don’t want to bother with antibody infusions. They just want to take some pills and go back to working or golfing or whatever it is they want to do.
Both are usually tolerable for the majority of patients. The ones who take long-term, obviously, for some patients have more chronic side effects.
Targeted Therapy Side Effects
Both these treatments are so effective, if you’ve never taken venetoclax or BTK inhibitors before, you can really pick based on your preference for treatment duration, and what side effects may or may not matter for your other health conditions.
btk inhibitors side effects
The main side effects of BTK inhibitors are:
Bleeding
Bruising
Cardiovascular side effects
Increase in blood pressure – high blood pressure can increase the risk for things like heart attacks and strokes. Overall, it can decrease cardiovascular health.
Abnormal heart rhythm called atrial fibrillation, or a-fib. A-fib is usually not life-threatening but is very irritating to deal with.
In addition, it can sometimes cause:
Joint aches or pains
Inflammatory arthritis
Diarrhea
Heartburn
Rashes – those usually go away or are less of a problem
Most people find the side effects from the BTK inhibitors tolerable, so they still go about their life with these things.
But for someone that has atrial fibrillation or is taking several blood pressure medications already, this might not be the best idea. People with bleeding disorders or who need warfarin anticoagulation don’t want to take this class of drugs if they have options.
Venetoclax side effects
Venetoclax, on the other hand, can cause tumor lysis syndrome at the start. All the CLL cells die so quickly it releases toxins into the blood. That’s treatable, but if you don’t watch out, it can be life-threatening or fatal.
You actually have to start the dose low and increase it slowly. People take a low dose, and over five weeks, they increase the dose every week to get to the full dose of venetoclax, which is 400 milligrams. They have to come for at least two days in a row for blood tests or monitor tumor lysis syndrome every time.
With this monitoring scheme, it’s very safe, and people developing tumor lysis syndrome can get that treated usually with medications. Things seem to go very well for people, but it’s a lot of hassle to do that.
To protect people from tumor lysis syndrome, they have to stay hydrated. People who have heart failure, take diuretics or have kidney impairment, which could make tumor lysis syndrome more common and more dangerous, might not want to go this path just because that’s a greater risk to their health.
Once people are at the target or treatment dose of venetoclax, it actually seems to have fewer chronic side effects than the BTK inhibitors. Some of them include diarrhea, lower neutrophil count or neutropenia (neutrophils are infection-fighting cells).
People can sit down and look at their health conditions. If they have severe kidney impairment, they probably want to take a BTK inhibitor. If they have abnormal heart rhythm problems, they would want to take the Venetoclax.
It’s a decision you make together with your treating physician.
I sometimes see patients considering their options for first treatment who ask me right off the bat, “Which one should I do?”
I say, “I don’t know, we just met. I need to ask you some things about you, and then I can tell you what you might want.”
I think these are really important, and the discussion is very similar for people picking a treatment that has taken before but never taken either of these classes of drugs before.
We always like to make treatment safer and better for our patients. So we had a study combining the BTK inhibitor ibrutinib, venetoclax, and an antibody, obinutuzumab, as a treatment for one year. It’s ongoing in follow-up, but everyone in this study has completed treatment.
When you give more drugs together, you get more side effects. It’s not a surprise, but the nice thing about this is it’s one year, and now we’re seeing how long people remain in remission at the end of that one year of treatment.
So far, we’re at about three years of follow-up, and it looks very good.
We’ve treated people with both relapsed/refractory CLL and people taking this as a first treatment. Several other studies are going on for BTK inhibitor and venetoclax combinations. We expect the response rates to be very high, but we are excited to know how long people remain in remission with this.
We hope to learn with longer follow-up who might most benefit from this combination and who’s going to stay in remission longer than with other things.
I’m just super excited that we really move the mark and get regimens into the standard of care in CLL and are able to do a randomized phase III trial, where you sign people to treatment in your treatment.
Again, there’s no placebo here, and usually, you know which one you’re getting to, after you randomize. You don’t know when you sign up, but you know before you get treated.
There are two ongoing studies, one through the Eastern Cooperative Oncology Group, or ECoG, and one through the Alliance. Those are both US Oncology Cooperative groups that do studies conducted on hundreds of sites across the US. They are both randomizing patients to ibrutinib and obinutuzumab.
You take the antibody for a limited time, but the ibrutinib indefinitely, and then the three-drug combination, ibrutinib, venetoclax and obinutuzumab given for a fixed duration. You don’t take it forever, and they’re looking at progression-free survival.
One study is for younger individuals, one’s for older individuals. They have a few small differences, but that’s mainly what they’re looking at.
I am excited to see over the next several years how that turns out, and I’ve also treated several people in that study who were really excited to participate in it.
You have to emotionally think it’s okay to be randomized, but a lot of people thought it was fun. They were like, “Oh, great, I’m going to get one of two great things, and I don’t have to pick.”
Metrics for these studies
When you pick a new standard, you compare standard treatment, which in this case is ibrutinib and obinutuzumab, to an investigational treatment, which is that three-drug combination.
The main goal is to determine progression-free survival: how long people are alive without leukemia and if one’s longer or shorter than the other. That’s a measure of how effective these things are.
Some studies use the overall response rate, but these drugs are so effective that they don’t really work out CLL because everyone responds to these things, which is great, by the way.
Then, when we look at the patients in the study who had high-risk features, low-risk features. Then we see how our high-risk patients did compared to high-risk patients with the other treatment.
For ibrutinib, some people have their leukemia come back while they’re still taking it.
Determining resistance to treatment
We have some neat studies going on at our institution and some other institutions across the country, looking at how we can identify who’s developing resistance to ibrutinib before they actually get sick.
We can look at mutations in BTK, which is the protein that binds at the drug binding target. Once people develop mutations in BTK, in particular spurts, we know that the drug will stop working.
We’ve offered them clinical trials to add a second drug like venetoclax to reduce this resistance and see if we can keep the leukemia from relapsing and be healthy for longer.
The CLL Community is looking at adding a second drug to people who are on ibrutinib and doing well. Remember, I said that ibrutinib, and actually, acalabrutinib II, which is the other BTK inhibitor, changed the way the CLL cells work and behave, but it doesn’t actually kill them off.
Lots of people still have CLL floating around, which is why we think they need to keep taking those drugs. We’re wondering if people can have another drug added to it to just knock out those residual leukemia cells. That way, they can be in off-treatment remission. If you do that, then they won’t be on it long enough to get resistance ideally.
Importance of clinical trials
It’s always good to know what your standard options are, and what your clinical trial options are.
For people who haven’t taken BTK inhibitors or venetoclax, those are good standard options. For people who are resistant to both those, usually clinical trials are your best option.
You always want to know what drug is being studied, how the study is going, who’s been in it, and what your doctor expects from the study.
Misconceptions about clinical trials and “placebos”
In cancer trials, you would know there was a placebo because you have to sign a consent saying there’s a placebo. But it’s usually considered unethical to give people who need cancer treatment a placebo.
It will explain if it’s randomized and what are the treatments that you would be getting. A lot of studies, especially the ones we have, are studying very new treatments. Sometimes they’re studying the dose of the drug.
You should know exactly what drugs you’re getting. It can feel really weird but you should consider your options.
With the state of cancer research these days, we actually have a very good feeling that these drugs are going to help patients before we give them to patients. Many of them have been studied obviously in the lab using CLL cells; cell lines have been studied in animal models of CLL.
We don’t start trials with new drugs until we’re fairly confident that it will help people. I’ve seen many patients benefit from drugs that they wouldn’t be able to get just because they’re not yet approved.
If anyone’s considering it and unsure if they have someone they know in the CLL community or peer support for someone that’s been in a clinical trial, it’s always good to talk with people who have done it just because the individual benefit to doing something like that can be significant.
People always tell me, “Oh, I feel like I’m your guinea pig.” I’m like, “Oh, you should be so lucky to be my Guinea pig, you know what that thing’s lifestyle is?” I was like, “My personal guinea pig is not an experimental animal. It’s my pet, has a super nice lifestyle. People would love to be my guinea pig.”
But really, people aren’t guinea pigs as much as you think. If you’re considering a research study, make sure you get to ask all the questions about what the drug is and why being in this study might benefit you or others, and your doctor should be able to answer those questions for you.
Up and Coming New Treatments
CAR T cell therapy
CAR T-cell is exciting. It’s still investigational for CLL, but I’ve seen it help a subset of patients, especially those that are resistant to these drugs I’ve been talking about. It can be very powerful for select people, but it is a hassle to do, and it is still investigational.
For people who have very good, other treatment choices, it’s usually not something we run to as a first treatment or even a second treatment. But it can be great for people that need that.
Reversible BTK inhibitors
The things that I’m excited about are some drugs that are hopefully going to move up to benefit more patients. We’re always trying to make treatment safer, more effective.
There’s reversible BTK inhibitors. Ibrutinib and acalabrutinib bind BTK at the same site and bind it irreversibly, meaning forever.
Reversible BTK inhibitors bind at different sites than the two approved ones and bind and unbind BTK, which seems to limit some of the side effects.
Also, for some reason, these drugs can work in people who are resistant to the BTK inhibitors, which you expect ’cause they bind to it at a different site but can work in people resistant to BTK inhibitors and Venetoclax. They seem to be very well tolerated.
A reversible BTK inhibitor such as LOXO-305 (pirtobrutinib) is now under study. LOXO-305 is the one that’s the furthest in development, and they just gave it a direct name.
It’s just exciting when I go to professional meetings to see what new types of drugs are being developed in CLL or things like cyclin-dependent kinase inhibitors that are coming back into play. These drugs, either alone or in combination, are likely to benefit patients.
Again, we keep moving the mark more and more towards safe, highly effective treatment, and it just keeps getting better.
New drugs with new mechanisms, drugs with the same mechanism but in a different way—these are the way we move the mark in CLL.
It seems to have fewer side effects, not no side effects. Anyone that tells you there’s are no side effects is lying. You never get anything for free or don’t do anything. But, that, and also because the mechanism is different from the irreversible BTK inhibitors, it can be used in resistance.
If someone takes ibrutnib until their leukemia comes back while they’re taking it, taking acalabrutinib isn’t going to work because they have the same mechanism. But taking a drug that binds the same protein but with a different way of doing it can work after your resistance.
This allows people to take two BTK inhibitors before moving on to a drug like Venetoclax or other treatment options. They’re just really effective, especially in people with really resistant CLL. It’s not just that there are fewer side effects, but also they seem to work great, which is awesome.
Treatments for Hairy Cell Leukemia (HCL)
Hairy cell leukemia vs. chronic lymphocytic leukemia
I love talking about hairy cell leukemia, which is another chronic B-cell leukemia. It also has very long survival rates, but it has some different features than CLL.
Unlike CLL, it’s very rare. It’s not very common to have people diagnosed with hairy cell leukemia.
HCL Treatments
Purine analogue chemotherapy
Over the last couple of decades, purine analogue chemotherapy was developed for hairy cell, and it’s actually spectacularly effective for the majority of patients.
People can take a single course of purine analogues and be in remission for decades sometimes. But there’s a group of hairy cell leukemia patients who don’t get decades of remission from purine analogues, or aren’t able to take them for other reasons such as side effects.
New drugs (cladribine, pentostatin, vemurafenib)
The hairy cell community has been working on new drugs for this group of hairy cell leukemia patients who aren’t expected to benefit from purine analogues like cladribine or pentostatin.
There are a couple of drugs in this area that are available and FDA-approved for people. But vemurafenib, which is not approved for hairy cell leukemia, has been very well studied. It can be used in people with hairy cell leukemia with a BRAF mutation which is found in the majority of people with classic hairy cell leukemia.
But there’s still a need for new drugs for this group of patients as those drugs don’t cover everybody.
We have actually conducted a phase two study of ibrutinib. It’s been FDA-approved for four different cancers. We’ve studied it in hairy cell leukemia, in a group of patients who aren’t expected to benefit from purine analogues.
People who have been previously treated or people with a variant of hairy cell leukemia have been found to have a very long progression-free survival. Around 73% of people are alive for three years without their leukemia returning.
The response rates don’t look quite as high, but that’s probably the response criteria we were using. You can really see how many people benefited by looking at progression-free survival.
It’s definitely a really important treatment option for people with this rare leukemia that aren’t expected to benefit from therapies like Purine analogues.
I think we published those results in a journal called Blood recently so that other doctors could find them and think about using that for their patients with a hairy cell that might need something beyond purine analogues.
Prognosis and findings so far
The prognosis for hairy cell, in general, is quite good. Most people can expect to finish their natural life span. Some people die of infection and rarely will someone die of leukemia.
Before purine analogues, survival was actually expected to be a couple of years, and not a couple of decades. When people don’t benefit from purine analogues, usually, they take more treatments, and their lifespan can be shortened by this. It’s still possible depending on what treatments you get to live for years.
It’s not like people had a very, very short survival, but certainly not the decades you’d expect from people that really get a lot of benefit from purine analogues, and other treatments like vemurafenib which is usually given for a fixed duration. Their relapse-free survival, or roughly how long it is before the leukemia returns in the majority of patients, is less than two years.
With this ibrutnib study, people are still alive without their leukemia returning for three years. Almost three-quarters of them are really quite good.
The study has been open since 2013. Some people have been in it a really long time, and I look forward to continuing to see how it benefits those patients. Some people are obviously quite sick and had taken 8 or 10 treatments before being in the study and probably wouldn’t be doing very well if they hadn’t been in a research study.
It’s also a nice example of how participating in a clinical trial can benefit people, because folks with hairy cell leukemia would not have had access to this if they didn’t decide to be in a research study.
Role: Center Director Urologic Oncology Focus: Urological oncology, including kidney, prostate, bladder cancers Provider: Cleveland Clinic
...
Dr. Babis Andreadis of UCSF shares his approach with patients, the importance of patient self-advocacy, whether to ask for a second opinion, and more on shared treatment decision-making...
Oncologist: Specializing in breast cancer | HER2, Estrogen+, Triple Negative, Lumpectomy vs. Mastectomy Experience: 30+ years Institution: Stanford Medical
...
Role: Radiation oncologist Focus: Specializing in radiation therapy treatment for all cancers | Brachytherapy, External Beam Radiation Treatment, IMRT Provider: Salinas Valley Memorial Health
...
Role: Clinical investigator and professor of hematological oncology Focus: Multiple myeloma, Waldenström’s Macroglobulinemia, early screening, clinical trials Provider:Dana-Farber Cancer Institute (Boston)
...
Role: Hematologist-Oncologist Focus: chronic lymphocytic leukemia (CLL) & leukemia and lymphoma | CAR T, targeted therapy Provider: Medical College of Wisconsin
...
Role:Hematologist-oncologist, associate professor Focus:Leukemias, Lymphomas, BMT Institution:UT Southwestern
...
Mark Lewis, MD, is not just an oncologist, he's a cancer survivor, himself. This gives him a unique perspective as both physician and patient. Hear more about his thoughts on second opinions and importance of self-advocacy...
Dr. Fonseca shares his insights on emerging T-cell therapies for multiple myeloma, describing the role T-cells play in our bodies and then focusing on chimeric antigen receptor (CAR) T-cell therapy and bispecific T-cell engagers.
...
Role: Executive Director, Mays Cancer Center; Prof. of Medicine Focus: Myeloproliferative neoplasms (MPN) Institution: UT Health San Antonio MD Anderson
...
Role: Director, Clinical Research Center for MPNs at MD Anderson; Section Chief, MPNs; Prof., Dept. of Leukemia Focus: Myeloproliferative neoplasms (MPN) Institution: MD Anderson
...
Dr. Ruben Mesa &Dr. Estelamari Rodriguez Dr. Estelamari Rodriguez and Dr. Ruben Mesa are respected oncologists in their fields, but in this video, they give a much deeper and personal look into their WHY for treating cancer. They also detail the importance of having representation and diversity both in doctors and in patients, especially when...
Dr. Saad Usmani, Chief of Myeloma Service at Memorial Sloan Kettering, talks about CAR T-cell therapy, bispecific antibodies, novel therapies and combination therapies.
...
Dr. Vincent Rajkumar, a hematologist oncologist at the Mayo Clinic, talks about drug pricing and the impact of high prescription drug costs on patients and families.
...
Long-time myeloma patient and advocate, Jack Aiello, leads the conversation with Dr. Joshua Richter, Multiple Myeloma Director for Blavatnik Family Chelsea Medical Center at Mount Sinai and Dr. Muhamed Baljević, Plasma Cell Disorders Research Director for Vanderbilt-Ingram Cancer Center.
Dr. Matthew Matasar, chief of blood disorders at the Rutgers Cancer Institute of New Jersey and RWJBarnabas Health, sat down with Dr. Samantha Spiegel, a Hodgkin’s lymphoma patient, to discuss some of the most exciting news coming out of ASH 2022.
The Patient Story founder and DLBCL advocate Stephanie Chuang leads the conversation with Dr. Josh Brody, who leads the Lymphoma Immunotherapy Program at Mount Sinai’s Tisch Cancer Institute, and Dr. Lorenzo Falchi, an oncologist at Memorial Sloan Kettering Cancer Center.
Top breast cancer doctors Dr. Paolo Tarantino with Dana-Farber Cancer Institute and Dr. Lola Fayanju with Penn Medicine discuss the big highlights from this year’s San Antonio Breast Cancer Symposium.
Multiple myeloma specialists Dr. Ajai Chari with Mount Sinai in New York and Dr. Sandy Wong with the University of California San Francisco discuss the big buzz at this year’s ASH: bispecific antibodies.
Dr. Serge Verstovsek and Dr. Naveen Pemmaraju discuss cutting-edge treatments and therapies, and combination therapy as a focus in treating myelofibrosis.
Patient advocate Jack Aiello and hematologist Dr. Shaji Kumar discuss what high-risk smoldering patients can do to delay or possibly avoid progression to active myeloma.
Dr. Chadi Nabhan shares how he got involved in the Monsanto trials, what he learned from the, and why he decided to write a book about the whole experience.
Patient advocate Valarie Traynham and Dr. Shakira Grant discuss the barriers many Black patients face, how it impacts their care, and what can be done to help improve their outcomes.
Medical oncologist Alok Tewari, MD, PhD, who specializes in cancers arising from the genitourinary tract, discusses what patients need to know about testicular cancer.
Hematologist Alfred Garfall, MD, MS, from Penn Medicine discusses with multiple myeloma patient advocate Jack Aiello the advancement of immunotherapy for multiple myeloma, the difference between CAR T-cell therapy & bispecific antibodies, and the role of bispecifics in the myeloma toolkit of immunotherapies.
...
Patients and doctors share their real-life colonoscopy experiences...
Cancer Survivorship Care Plan for Hodgkin Lymphoma Patients...
Nicole Lamanna, MD, from Columbia University Medical Center, Spencer Bachow, MD, from Boca Raton Regional Hospital, and CLL patient Lisa P. discuss the importance of building a strong support system and collaborating effectively with multiple doctors.
...
Leading experts Estelamari Rodriguez, MD, MPH, from the University of Miami Sylvester Comprehensive Cancer Center, Jason Porter, MD, from West Cancer Center & Research Institute, and Terri Conneran, founder of KRAS Kickers, discuss the latest in lung cancer treatments and ongoing clinical trials.
...
Patient advocate Cindy Chmielewski, experts Dr. Carl Ola Landgren and Dr. Caitlin Costello, together with clinical trial nurse Christen Hawthorne uncover groundbreaking insights on the latest multiple myeloma treatments and clinical trials.
...
Patient advocate Ruth Fein Revell, experts Dr. Angela Fleischman and Dr. Ruben Mesa, together with clinical trial nurse Melissa Melendez delve into the cutting-edge realm of myelofibrosis clinical trials.
...
Patients, care partners, and a panel of CLL experts including Dr. William Wierda, Dr. Nicole Lamanna, Dr. Adam Kittai, and Jackie Broadway-Duren share the latest in CLL research, clinical trials, treatments, and comprehensive care strategies.
...
Palbociclib Side Effects & Patient Stories Palbociclib, commercially known as IBRANCE, is a treatment for a specific kind of metastatic breast cancer, or breast cancer that has already spread to other parts of the body, known as HR+/HER2- mBC. Palbociclib may be able to renew patients’ hope and offer them a greater sense of possibility...
Patient advocates Cindy Chmielewski and Jack Aiello, and experts Dr. Rafael Fonseca and Dr. Susan Bal discuss promising multiple myeloma treatment options.
...
Dr. Matthew Matasar, chief of blood disorders at the Rutgers Cancer Institute of New Jersey and RWJBarnabas Health, discusses some of the most exciting news coming out of ASH 2023.
Dr. Andy Evens from Rutgers Cancer Institute discusses how to reduce the toxicity of Hodgkin’s lymphoma treatments so patients can live their best lives after cancer.
Self-Advocacy & Shared Decision Making in Cancer Treatment
Mark Lewis, MD
Dr. Mark Lewis shares his perspective on patient care and shared decision making during cancer treatment, not just as a top-trained oncologist and director of Gastrointestinal Oncology at Intermountain Healthcare, but as a former cancer patient and caregiver, himself.
Thank you for having me, this is a real thrill for me, too. I’m not just an oncologist, I’m also a person. I think we can start with the breaking news that oncologists are human beings.
Frankly, that’s not a foregone conclusion, we have a pretty nasty reputation that’s come about because people naturally associate us with our treatments, and our treatments have an unfortunate legacy of a lot of indiscriminate toxicity.
One of the reasons I’m happy to do this is I want people to see that doctors, especially oncologists, come to medicine for actually pretty compelling and emotional reasons, often more than their attraction to the science.
Describe your professional background
I practice at Intermountain, which is a beautiful description of where I am. I work in Utah, I’m licensed in six states in this region, and we cover basically a pretty vast expanse.
Once you go west of the Rockies, up towards the Pacific Northwest, and across Nevada, we cover that area. It’s actually really great that I’m talking to you because, in the last year in particular, we were already doing telehealth.
The pandemic has forced us to increase our bandwidth and our ability to be facile with this kind of technology. Now I can talk to people states away.
Is it exactly the same as being together in the same room? Well, no. There is a lot of oncology actually that is appropriately tactile. That aside, it really has been a very rewarding experience.
We’ve actually had people tell us if they hadn’t had access to telehealth and oncology, they would just stay where they were and foregone any treatment whatsoever. I can actually cite examples of people whose lives have been saved by Zoom, which is remarkable. That’s where I’m at.
It’s a very different practice environment. I came here from MD Anderson Cancer Center, which is a well-known research center in Houston, and the model there was you’re going to come to us. Obviously, it’s a major metropolitan center, we have patients literally from all over the world. Unfortunately, a lot of the people who came in there had exhausted conventional treatment options, and so they were willing, they were invested.
One term that is used for folks like that is medical tourists. Sometimes people say that almost as if they’re denigrating the patient, I don’t like that. I think what it’s pointing out is there’s this select group who are sick enough to need next-level treatment, not so sick that they can’t travel, and then also with some means at least to be able to essentially move to another city to get care.
While I found that very rewarding, I would actually much rather take care of people where they live. That is what we’re increasingly trying to do with tele-oncology.
Medical training
Working backwards in my career, I did my training at the Mayo Clinic in Rochester, Minnesota. There again, it was a center almost literally in the middle of the frozen tundra.It’s a remarkable place to visit because most people would drive down from Minneapolis–Saint Paul and you’re just going through cornfields and cornfields and it’s beautiful.
Then all of a sudden you see these glimmering towers in the distance and it’s Mayo Clinic. Boom, you’re in a world-class medical center. There again, almost by necessity where it was located, yes, we cater to the local community. Next to my Minnesota farmer was someone who might’ve traveled from Saudi Arabia to get the latest cancer treatment. It was an amazing place to train, but again, it wasn’t really representative of the American public.
Adolescent Young Adult (AYA) Cancer Patient Care
What is the AYA cancer patient population
The reason I came to Utah is two-fold. I’m part of a dual physician couple, so my wife’s a pediatrician, and this is the youngest state in the nation. The average age here is 30. I think one in four people is between kindergarten and 12th grade.
That also means, for me, there’s this really compelling, if troubling, problem here of young adult cancer. There’s various definitions for that.
The most conventional one in the US is people affected by cancer, either a liquid tumor like leukemia or a solid tumor on the colon or breast, anytime between age 15 and 39.
This has been an amazing place to deal with that particular demographic because everyone here is, or not everyone, but many people are young. One in seven people in my practice to fit that demographic.
I think hearing them can be heartbreaking, but it can also be super satisfying, because if you can cure someone like that, that’s decades of life that you’re giving back to them.
That, in a nutshell, is my oncologic pedigree and how I got here.
Awareness of AYA cancer patient care
It’s been an amazing movement. It really has only existed for, at the most, 30 years that we’ve had this recognition that this is a group apart. Unfortunately, in that 30 years, while there’s been a lot of progress, there’s also been a lot of growth in that demographic and not in a good way.
One thing that I deal with as a GI oncologist is colon cancer, which we used to think of as a disease largely related to senescence. We used to set the screening age 50 or older; it’s happening in younger and younger people.
The example I give, which is tragic and extremely well known, is I was sitting at home last summer watching Black Panther with my son on a Friday night and my cell phone starts blowing up. It’s all my friends, many of whom are nonmedical, asking if I had known that Chadwick Boseman died of metastatic colon cancer.
I was just absolutely floored. I was watching the guy be a superhero on the screen. He’s a perfect example actually of you can be young, you can be healthy, you can be incredibly fit, you can have resources, and you can still get cancer.
Misplaced blame on (young) cancer patients
One of the things I want to touch on is the false shame and blame that is placed on cancer patients. It’s a disease that has actually long suffered from stigma for decades.
I think The New York Times actually had a ban on the phrase “breast cancer.” This was decades ago, but regardless, it goes to show you that we haven’t entirely come away from that.
Especially online, there’s a lot of unfortunate finger-pointing, especially when someone young gets cancer. The assumption is, “Oh, you must’ve done something wrong.” Far from it, it’s usually not anything the patient did, it’s some unfortunate combination of genetics and circumstance.
Personal Connection to Cancer
Your first experience with cancer
The reason I went into oncology, so not just medicine but oncology, is when I was eight years old, my father was diagnosed with cancer. The circumstances, while they’re never going to be ideal, were particularly almost Kafkaesque because what happened was we were moving to the States. When you immigrate here, you have to get a chest X-ray as a public health measure to exclude tuberculosis.
We got this call from the government saying, “There’s good news, bad news here. The good news is you don’t have TB,” talking to my dad and he’s a 42-year-old at the time. “The bad news is there’s something occupying your entire right lung. When you get to America, you should probably have that investigated.” On the phone. Click.
That’s a lot to handle when you’re moving countries. There’s some ranking of stressors and one of them is moving. I think the other is getting a major diagnosis. This was both at once. Frankly, at that time, we hadn’t learned the American healthcare system. The National Health Service in the UK is far from perfect, but one of the things it’s really good at is avoiding or minimizing financial toxicity for patients.
We got here, thankfully my dad had a job, but it was still tens of thousands of dollars out of pocket for his care. He required his entire right lung to be removed. He required radiation and chemo after that. I know this sounds like, “Boy, after all this, why would you want to go into cancer medicine?”
It’s because his oncologist was so good and my dad didn’t pass away.
His oncologist took me under his wing. Then every summer in high school and college, I had other jobs, working in the movie theater and stuff, but I knew I had a job that I could go to as a medical assistant at this clinic, and it was the same clinic where my dad had been treated.
First, I felt a little strange going back there, but sooner or later everyone got used to me, didn’t treat me any differently than any other employee. I learned by following and shadowing this guy, how he did oncology.
Special care in patient relationships
One of the things I loved about it was I sensed how close he got to his patients. In this era, it sounds almost improper to say that, but it’s true, you get a really deep kinship, I can say that, kinship with your patients. I stopped saying “friendship” because I know there’s a power dynamic, and I know when you’re the oncologist and the other person’s the patient, it’s difficult to ever quite erase that imbalance.
Regardless, I saw what he did. This back in the era of paper charts. Before he went in the room to see a patient, and he let me follow him, he had written all the relevant medical stuff in the center, but then in the margins, you have all these tiny little details, grace notes of someone’s identity.
Then he would remember to ask them about their child playing a baseball game or, “How was this trip that you took?” I was like, wow, he’s really taking the time to learn about these people. They’re not just the host for a tumor, which is how some patients in oncology are made to feel. They’re people to him.
It took seven years for my a book my dad wrote to get published. It got published posthumously, and his friend actually showed up, completely to our surprise, on the book launch. That was seven years after my father had passed. We were just absolutely blown away. That was just the kind of connection he had.
Your own cancer story
Fast forward, I started my oncology training. Day One, I woke up with this horrible bowel pain, which naturally you could attribute to nerves. It’s overwhelming to be at Mayo and starting, embarking on your fellowship.
When I went to get checked out, one of the other things I thought it might be was appendicitis because it felt like it was in the right lower quadrant. It wasn’t. It was a high calcium level and why is that relevant? My dad had suffered from that his whole life.
No one had ever really figured that part out, and people told him, “Oh, you’re eating too much dairy.” Again, this whole shifting the blame to the patient. My dad fastidiously eliminated all that stuff, still suffered from high calcium, kidney stones, GI issues.
When I realized I also had that, the way I describe it, and I don’t think it’s hyperbolic, is you can look at the stars for a long time and then, all of a sudden, you can see a constellation, you can see a pattern. That’s what I saw.
I was lucky enough to be in the right place at the right time, with just enough training, to know that there are really only a couple conditions that give you consecutive generations of high calcium. One of them is a neuroendocrine tumor syndrome called multiple endocrine neoplasia type 1.
When I realized there was this connection, it all fit. I was starting my cancer training at Mayo, which is famously a wonderful place to be diagnosed with something esoteric, though I didn’t think I would be doing it for myself.
I went to my internist, and frankly, I don’t blame him, he thought I was a hypochondriac. Day One of oncology training, coming, and saying I have a tumor syndrome, claiming all kinds of outlandish things about my family tree.
I realize how lucky I am because if I was any other patient, if I didn’t have the ability to play the card of professional courtesy, I think it’d be written off, at least for a while.
Also, you can’t ethically order things on yourself, so I needed someone to do the diagnostic work for me. I basically twisted his arm, I said, “Hey, listen, just take a bet on me. If I’m wrong, I’m wrong, but I think I’m right,” and sure enough, I was. I disclosed that to the people who were running my training program because I thought it was important that they knew, and they could not have been more supportive.
In hindsight, it explained everything about my dad. Again, his oncologist was wonderful, and I clearly idolize the man, but he never put two and two together about what was causing my dad’s cancer. It was always dealing with what we had to confront, but no one ever got to the bottom of why it happened.
In fact, the reason I bring that up again, is my father was a Protestant minister and a theologian. He thought a lot about guilt and sin, and I wonder if in that framework, he didn’t end up blaming himself far too much.
For instance, as I mentioned, the mass started in his chest, so sometimes described to us as a lung cancer, it wasn’t really. Then he wondered, “Oh gosh, I’ve never smoked, but did I spend too much time around secondhand smoke?” Anyway, there was all this retrospection he went through and among other reasons.
I miss my dad. I wish I could tell him, “It wasn’t your fault.”
Theory: many oncologists are driven by something personal
I have a pet theory that oncologists are more likely to have dealt with cancer, themselves, than almost any other specialty.
The way I inherited my disease is called autosomal dominance. There was a 50/50 chance I was going to get it from my dad, but lightning is not always quite that strong.
My point is, many of us come to this field because, yes, the science is amazing and the pace of research is absolutely mind-boggling, but most of us come to it because we’ve known someone with cancer. Sometimes that’s a friend; more often, it’s a relative. If it’s a relative, that means there’s some blood linkage, and presumably, some even slightly heightened risk that you might deal with it yourself.
What I want patients and caregivers to know is I was at Mayo dealing with these world-class oncologists, and so many of them, I won’t reveal their identities, took me aside after I disclosed my own problem and said, “Yes, I’ve dealt with cancer, too.” It just blew my mind.
Obviously, it’s emotional what we do, dealing with people who grapple with their own mortality, and sometimes at a very young age. I think that a lot of us do this because we’re trying to help other people when maybe we couldn’t even help our own relatives. I know I feel that way about my father.
The Patient-Doctor Relationship
Old paradigm of patient-doctor relationship
There’s a paradigm that still exists in some places. It’s paternalism, where the doctor has all the power. It used to be someone in a white coat, very stern, comes in, first appointment, “You got cancer,” we brush that aside very quickly, and then we tell you what you’re going to do.
That used to be the exchange, and it felt very unidirectional. What I would tell patients now is we live in the information age, we have more access to information than we’ve ever had before. I realize, again, the playing field is not perfectly level.
Patient access to good data
One of the things that frustrates me even as a self-advocating patient is when I try to get really deep in the weeds and research things, I sometimes come up against paywalls. A lot of research, even publicly and federally funded research, ends up being put in journals that are financially inaccessible.
It’s not uncommon and if you’re trying to get a single article, one article, it might cost you $60 just to get your hands on that one piece of paper. That really, really frustrates me.
Honestly, some of our research findings are necessarily behind closed doors. What I mean by that is they’re not ready for primetime yet. Unfortunately, oncology is littered with examples of things that have been biologically plausible or even look very promising in very early phases of drug development, but then they don’t actually work when you put them out and study them either in human bodies, or going from a test tube to a person or in large groups of people, especially in a randomized clinical trial.
Those two things aside though, I would argue that most patients have access to the same information the doctors do. The question is, how do you filter it because as you all know an engine like Google is incredible, but it’s also gameable. Google is not it’s not a completely altruistic organization. There’s a reason you get this in exchange, the transaction is you, it’s your information.
Regardless, where I want to empower patients is I’ll say, if you feel there’s something wrong with you and you feel like your doctor is not helping you deal with it, you are entitled to a second opinion.
The importance of getting a second opinion
One of the things I say is if you ask for a second opinion and your doctor says, no, that is a reason to get a second opinion.
Any doctor these days who thinks they know it all, especially in oncology, is absolutely kidding themselves.
There is so much to know. I don’t know. I know a lot of smart people, I don’t know anybody who knows everything, even in cancer. The reason I do only GI oncology now is the field is massive and unwieldy. There is no physician, there is no specialist who can possibly know everything.
The risk of getting misdiagnosed
What I would say to patients is, and I guess this is just different phases, there’s the part where you’re getting diagnosed and then there’s a part where you’re going through treatment.
I actually think the diagnosis part can take quite a bit longer. I’m not alone in that it takes on average something like seven years or even a decade for someone with a neuroendocrine tumor, which is my tumor type, to get diagnosed. The reason is it looks like so many other things.
One of the classic ways this presents is something called carcinoid syndrome, which broken down means cancer-like syndrome, and even that’s a misnomer. It can be a real cancer.
Regardless, these patients have a very classic constellation of findings. They’ll get very, very flushed, they might wheeze, and then they have horrible diarrhea, the latter of which is not easy for people to disclose.
Here’s the problem, there’s that whole parable about the blind men feeling the elephant and each feeling a different part and concluding it’s a different animal. Depending on which specialist you go to, they have anchoring bias on their discipline.
If you go to a pulmonologist with the wheezing, they might diagnose you with adult-onset asthma. If you go to a gastroenterologist with diarrhea, they might say it’s irritable bowel syndrome (IBS). For women in particular, and there’s a lot to dive into here, there often misdiagnosed with the flushing. They’re told, “Oh, it’s perimenopausal hot flashes.”
Because you start accumulating all these different and wrong labels, it can be very, very difficult to expunge those from your chart to finally arrive at the right diagnosis. What I’m getting at here is patients like me tend to have a history of either misdiagnosis or delayed diagnosis.
During this whole process, no matter how long it takes, you’re still inhabiting your body all the time. You know something’s wrong and you just can’t put your finger on it. Then presumably all of these treatments that are being assigned to you are probably also not helping as much as it’s supposed to and that’s very frustrating.
I give patients a lot of credit. I tell them, “Listen, you are you all the time. At the most, I get to see you once a week.” Most of my folks, I see every other week on treatment.
Shared Decision Making in Treatment
Practice of medicine vs. business of healthcare
Another statistic that’s amazing or scary is if we halted all oncology research today, just stopped experimenting and just applied what we already know, we’d probably save close to 100,000 lives a year.
What that tells you is the science is awesome, but there’s a huge lag in implementation, and some of it also comes down to payment. The trap I sometimes fall into is I’ll come back from one of these conferences and I’ll be giddy with enthusiasm about some new treatment, and I sometimes over promise to my patients or over disclose and I can’t actually get it to them.
One thing I say all the time is there’s the practice of medicine, which is what I do and what I’ve trained to do, and there’s the business of healthcare, which is this whole other incredibly complicated often Byzantine infrastructure.
The two are not the same at all. The training to go into one or the other is completely different. I have friends actually who have been so invested at understanding the business that they’ve gone and gotten a master’s in health administration. Those people are the exception, not the rule.
Most of us who do oncology have absolutely no idea. When we prescribe something to you, we don’t know how much it’s going to cost, we don’t know often if your insurance is going to approve it upfront, if we’re going to have to appeal, if that’s going to take time, and time is the ultimate currency.
I don’t care who you are. I don’t care if you’re Jeff Bezos, you can’t buy time. Especially with oncology, it drives me crazy because there’s that initial encounter with the oncologist. I don’t know about you, but a lot of my patients tell me they don’t really hear or retain much of that first visit beyond just the confirmation that there’s cancer.
Then the last thing you want to do once you have cancer is to wait, right? There’s this fierce urgency that comes with the diagnosis, “Oh my gosh, we know this now, let’s act on it.” Frankly, it breaks my heart sometimes because I have told someone, “Okay, we need to do X, Y, Z,” and I’ve cited this amount of evidence. But if I can’t get that to you, that is just beyond frustrating. It’s frightening.
That’s the part that makes me the most angry. I hope I don’t come across as an angry person, but I have a righteous indignation when it comes to my patients because once you’re my patient, again without sounding paternalistic, I’m very protective that I now have taken on a responsibility for you.
Medicine sometimes involves fighting with insurance companies. Now, not all insurance companies are bad, and I’m not going to name names here. I just have some I like more than others, but it is difficult for the insurance companies, give them credit, to keep their policies going at the same pace, the same tempo as the discoveries. The biggest problem in modern oncology, in my opinion, is getting the stuff we know works to the patient in a timely enough fashion.
Risk-benefit in choosing treatments for patients
One thing I’ve been very interested in is sometimes you get to a crossroads in someone’s treatment and there is more than one option that you can reasonably pursue. What I’ll often do is spill out to the patient, “We could do A, B, or C,” and I try to build in a risk-benefit calculus, if you will, to each option. It’s very interesting because it’s almost half and half.
I’ve got some young patients, but the average age of my patient is 68, and it’s probably from the generation that’s more used to the doctor telling them what to do. Some of my patients tell me, “Listen, you pick, I don’t want the burden of picking.”
Others are deeply interested in researching which path they’re going to be on, and I give them the time and hopefully the information so they can do that. It’s really fascinating. We want to offer autonomy, but we don’t want the weight of that to be too hefty.
Patient research on clinical trials and treatments
I see a lot of patients coming in and they’ve done a lot of homework online, but one of my favorite things that happens these days to really flip the script around is a patient will tell me about a trial that I haven’t even heard of.
Again, no oncologist knows everything, and because there’s new studies opening up all the time, even those of us who really try to keep our finger on the pulse, we don’t know it all.
Occasionally a patient will come in and they’ve gone to clinicaltrials.gov, the central clearinghouse for all this, and they’ve put in an appropriate search string. They’ll say, “Hey, Dr. Lewis, would this be right for me?” Then we read over it together, and it’s either yes or no, but it’s a really cool process.
Get to the point where you can have a true dialogue, not be worried about offending your doctor’s sensibilities or whatever.
Importance of patient self-advocacy
Here I will invoke older generations. My Scottish grandmother, bless her heart, was in her 90s had a heart attack on a Sunday, a crushing chest pain. She didn’t call anybody until Monday morning and survived. When we asked why, she said, “Oh, you don’t bother the doctor.” I often say to my patients, “You very much bother the doctor, that’s what we’re here for.”
In my group, we’re fortunate we have a system where we trade-off, but we cover our clinic 24/7. If you’re having a heart attack, we want to know about it. The other thing is there is a lot we can tell about you from labs and scans, but as I mentioned earlier, you’re the ultimate surveillance system for your own body. Without making it too onerous on the patient, there are certain side effects I just can’t see.
The classic one, and this is appropriate across a variety of different tumor types, is neuropathy. A lot of the drugs that we give in oncology, unfortunately, have a really nasty downside, which is potentially permanent nerve damage. The problem with it is usually once it happens, it is not reversible.
It is a case where an ounce of prevention is a pound of cure, and the only way we can mitigate it often is to be extremely careful with our dosing upfront. All my patients know, I’m on them constantly, “How are your nerves this cycle? How are they now?” The reason I do that is I know that some of these drugs, I just can’t take back.
Mayo is a world-class center for multiple myeloma, a plasma cell disorder, and classically the drugs that they use in multiple myeloma can cause neuropathy. I’ll never forget this. You tend to remember your mistakes more than your successes.
I was in training, I was presenting to, if I’m honest, a pretty fearsome myeloma professor, he was the chair of the department, and he’s a very opposing man. I suppose I was trying to placate him. I described to him that a patient quote, my exact words, “Only had grade two neuropathy,” and he stopped me. He said, “You will never say that again. You’ll never say ‘only’ about someone’s side effect.”
He’s absolutely right because on this scale, grade two neuropathy means you have constant numbness and tingling. It’s not anything that you would want.
The importance of acknowledging side effects
The other thing I’ll point out as a patient, phrases that drive me the craziest in oncology, are the rhetoric that tries to minimize side effects. The phrase that I hate the most if I’m very honest is “manageable toxicity.”
Often what you’ll find in a scientific conference is a drug might actually work very well, it may be highly effective, but as we hinted at the very beginning, might also be really toxic.
What’ll happen is you’ll see these researchers, understandably they’re excited to share their findings, but sometimes they tend to sugar coat whatever this new treatment is. They’ll throw that phrase in. The reason I find it so objectionable, it’s almost sophistry, is when they say that, my retort is always like, “Well, if it’s so manageable, would you want to take this drug yourself?”
It’s really interesting. If you poll our oncologists, I think this has actually been done sort of formally, but you can do it informally and say, “Hey, would you be willing to take x, y, z?” Many people would say no.
At Mayo, in myeloma, I came across this chemo recipe we were giving. I’ll be honest, I thought it was a misprint. It was seven drugs put together. I was like, “There’s no way. There’s absolutely no way this is an accurate acronym.” Sure enough, it is; it’s a seven-drug regimen.
There are many of us who, if you really put our feet to the fire, would not accept the very things that we have been trained to prescribe. That kind of, I guess I’ll say it, hypocrisy has also not served as well in terms of our public image.
The goal, and I tell my patients this all the time, is to marry effectiveness to tolerability. Especially if you’re a young person and I think you can live for decades, I want you to live for decades with a good quality of life.
The tough part is sometimes to get to cure, you have to basically put the patient through just the most exquisite rigorous procedures, like a bone marrow transplant or something. If you can get them out the other side and they’re relatively intact, that’s the goal.
Your personal treatment decision-making process (Whipple surgery)
This was what my pancreas used to look like, and now I’ve lost basically the part that I’m covering with my fingers. I’ve got the back half but I lost all this. Unfortunately, this is the more important half.
Because I diagnosed myself right as I was starting my oncology training, I saw my entire process of being a fellow. Three years I was learning the field, then ever since I’ve been an attending, I’ve always seen it through the lens of being a patient, too.
I was very lucky. I still have tumors in my pancreas, but the most bothersome tumors I had were slow-growing and in a tricky place, which is the head of the pancreas. If I flip this model around, you can see there are tons of blood vessels. The common bile ducts, it’s very high-value real estate. It’s the Manhattan of the abdomen. I didn’t want to intervene on it until I absolutely had to. Here again, I empathize with patients because I was at Mayo and I got three different surgical opinions.
Depending on which expert you go to, you’re going to get a different answer. I went to one guy, he said, “Oh, this is easy. Let’s take the whole pancreas out.” Well, okay. Surgically, actually, that would have fixed the problem, but talk about quality of life.
At least at the time there was an estimate that that would have taken over a decade off my lifespan because your pancreas does some important things. Rather famously, it makes insulin. Now we’ve come a long way now with insulin pumps, and so there are people who live without a pancreas, on an artificial pancreas, and they’re able to have insulin infused almost continuously should they need it.
What many of them can’t do though is bring their blood sugar back up. High blood sugar is bad in the long run, low blood sugar is acutely life-threatening. They live in this very, we actually used the term, brutal existence, brutal diabetes. I didn’t want that.
I knew option A, I didn’t want that. I’m genetically mutant so my whole pancreas is weird, but regardless, the biggest ones were up here in the head. For Option B, they said, “Well, we can do the Whipple procedure, so we can just cut this part off.” I asked if that was going to affect my training. They’re like, “Oh, yes, you’ll be gone for months.” I was like, “Well, I don’t really want to do that.”
Then the final option, which is what I took at the time, was observation. This part appealed the most to the logical part of my brain. They said, “Two points make a line, so rather than jumping right in and doing surgery, why don’t we just see how your tumors grow?”
That came with its own risk that these tumors were going to explode, they were going to become inoperable, they were going to spread. Based on what I understood, that seemed unlikely, and so we watched. I was able to watch for eight years before a tumor in the head of my pancreas did exactly that and exploded in growth. Then I knew it was time. I knew it was time for surgery.
By that point, I was already working here. I had a very supportive employer. They said, “Of course, you can do this and you can take medical leave.” I took the right amount of time and then I came back.
Having the patient perspective as a physician
What’s been really funny for me, I say funny and really has been rewarding, is because I was so open about going through that, it’s actually enriched my practice. I actually have people who seek me out because they have pancreas problems, which I can totally relate to. They’ll say, “We came to you because you get it.” I kind of do, but in some ways, I don’t because I have the less typical form of pancreas cancer.
The more typical form is more aggressive than what I have had to deal with, almost always requires chemo and can require radiation. I have not yet needed those things. Again, I know not quite what I say when I talk about chemotherapy and I tell the patients that when they’re like, “Oh, you get it, you empathize.” I’m like, “Well, I can to a limit,” I can empathize with dealing with the diagnosis, dealing with something that is genetic.
Interacting with Patients
Importance of real-time doctor-patient communication
Frankly, one of the huge advances in the last couple years has been real-time communication with patients. There’s a really famous study, you might actually know of it, but it was presented at one of our meetings in 2017. As is often the case at oncology conferences, it was a survival curve.
What that means is you’ve got two lines and one line shows you how people are doing with intervention A and the other with intervention B. What I’m telling you is if you put up just the slide, just this, the curves, and you saw the separation between these two groups, you’d be like, “Oh my gosh, whatever drug they’re giving to group A, this is a billion-dollar product. This is going to be like blowing the doors off and changing the standard of care.” It wasn’t a drug.
It was a computer program based on people’s cell phones where they could just note in real-time when they were having symptoms and then fed back into a system involving nurses and doctors where they could respond in real-time.
That was the survival difference. My point is just listening to people as close to their present experience as possible, that is so powerful.
The power of social media
There’s a lot of fire for further conversation there, but I’ll just say in my career, which has not been that long, I’ve seen social media go from something that was considered frivolous and unprofessional for a doctor, and certainly oncologists, to something that’s almost become, not mandatory, it’s strongly encouraged. There are a couple of reasons for that.
I did a Google search where I let the search engine auto-complete the phrase “oncologists are,” and what came up, at least for me, was oncologists are murderers, oncologists are criminals, oncologists are poisoners, all this stuff. I was like, “Holy smokes, these are the top answers on Google?” I was like, “I got to do something about this.”
You feel like a tiny drop in a big ocean, but I thought one thing I could do is be open.
Now with that, I’ll say a couple of things. Vulnerability is the right word because you do make yourself potentially a target. It’s very seldom, thankfully, but I’ve dealt with trolls, dealt with death threats at one point, dealt with pedophilia towards my children, and all these really, really horrible things. Thankfully, that is the tiny, tiny fraction of my social media experience. Some of my peers look at that and they want nothing to do with it. I don’t blame them.
However, it’s also become a tool, if I’m being very honest, for oncologists’ professional development because as I mentioned earlier, there is so much to know. What we can do as doctors is use it to refine our own information stream.
If I just sat and tried to read every cancer research article that came out, I wouldn’t be able to do it. I certainly wouldn’t be able to practice at the same time. There’s some point where you just get oversaturated and frankly, it’s not all equally meritorious either.
One of the things that’s good about Twitter, and this may not be not so visible, is using it as a curation tool for us. Also is important because it lets you see what matters to patients. If you listen to advocates, you learn a lot. We have almost countless other metrics that we like to use to say, “Oh, treatment X is better than treatment Y.” Very few of them matter to patients. At the end of the day, they’re often just very poor surrogates, if they’re surrogates at all, for living longer and living better.
Then there’s the tone on Twitter. I tweeted about that this morning. It is really, really hard because there’s no font. You can’t really broadcast clearly when you’re being sarcastic versus being genuine, so I’ve learned to try not to be the former. The tone is really tricky.
One of the things I’m told is sometimes I tweet about heavy stuff, “People are dying.” Then people are like, “Oh, you’re so serious.” Then I try to be comical and get, “Oh, you’re being far too glib for an oncologist.” You can’t please everyone all the time. I love the conversations that happen there, I love the fact that you and I met.
Dr. McDrea— Lewis used this picture as his original Twitter profile picture!
The importance of patient stories
Your platform does an awesome, awesome job of storytelling. Again, this might actually be the central tension I think between patients and oncologists. We love numbers, we love data, and the way our studies are set up, we’re supposed to look for statistical power, right? We need big enough numbers to be sure that our conclusions are generalizable.
In the process though, we discard individual experiences, so N equals one (n = 1). There are very, very few studies that you’re going to predicate just based on the experience of one person. Unfortunately, what that’s led to is we get all myopic about the numbers and the graphs. We forget about the people.
One of the things that I’ve also tweeted and written about is that survival curve I mentioned earlier. Every time it notches down, we’ve lost somebody. We need these graphics to be able to visualize the data, but sometimes I stare at them, especially when they plunge, you’re like, “That was people dying.”
That’s where stories are so important. Joseph Stalin, a weird person to end with, I know, said, “A single death is a tragedy, a million deaths is a statistic.” That’s so powerful, and I actually talk about that a lot because he’s right. We are narrative creatures, a story resonates with us. Most of our entertainment is about narrative.
When you hear someone’s experience the way that your platform allows, it’s so resonant. Then when we take that and put it in numerical form, it’s like we’ve cut away the human husk and we’re left with this kernel of information, but we can’t discard that person’s humanity in the process. That’s the disconnect, especially when I go to these meetings.
That’s where I feel really lucky because I’m occasionally given a podium or a microphone, and I get to speak up as a patient.
Again, I’ve been very demonstrative on Twitter. I love it when someone said I was performative, I was like, “Well, I didn’t go through pancreas surgery to gain clout.” I think anybody can call you performative, and you can say your virtue signaling. These are often very telling accusations about the person who’s slinging mud at you, regardless.
I feel very privileged. I feel privileged to talk to you. I also feel privileged to talk to my peers. I am the furthest thing from the world’s greatest researcher, I’m actually not very good at the really, really rigorous clinical trials that are going to move the field forward.
What I can do, what I try to do, is speak up if I see us focusing so much on effectiveness or some metric by which we assess it and forget about the patients. Again, that goes back to toxicity and what you were saying earlier about balancing out longevity and quality of life. That’s the whole point, is that we want both. We really want both.
Role: Center Director Urologic Oncology Focus: Urological oncology, including kidney, prostate, bladder cancers Provider: Cleveland Clinic
...
Dr. Babis Andreadis of UCSF shares his approach with patients, the importance of patient self-advocacy, whether to ask for a second opinion, and more on shared treatment decision-making...
Oncologist: Specializing in breast cancer | HER2, Estrogen+, Triple Negative, Lumpectomy vs. Mastectomy Experience: 30+ years Institution: Stanford Medical
...
Role: Radiation oncologist Focus: Specializing in radiation therapy treatment for all cancers | Brachytherapy, External Beam Radiation Treatment, IMRT Provider: Salinas Valley Memorial Health
...
Role: Clinical investigator and professor of hematological oncology Focus: Multiple myeloma, Waldenström’s Macroglobulinemia, early screening, clinical trials Provider:Dana-Farber Cancer Institute (Boston)
...
Role: Hematologist-Oncologist Focus: chronic lymphocytic leukemia (CLL) & leukemia and lymphoma | CAR T, targeted therapy Provider: Medical College of Wisconsin
...
Role:Hematologist-oncologist, associate professor Focus:Leukemias, Lymphomas, BMT Institution:UT Southwestern
...
Mark Lewis, MD, is not just an oncologist, he's a cancer survivor, himself. This gives him a unique perspective as both physician and patient. Hear more about his thoughts on second opinions and importance of self-advocacy...
Dr. Fonseca shares his insights on emerging T-cell therapies for multiple myeloma, describing the role T-cells play in our bodies and then focusing on chimeric antigen receptor (CAR) T-cell therapy and bispecific T-cell engagers.
...
Role: Executive Director, Mays Cancer Center; Prof. of Medicine Focus: Myeloproliferative neoplasms (MPN) Institution: UT Health San Antonio MD Anderson
...
Role: Director, Clinical Research Center for MPNs at MD Anderson; Section Chief, MPNs; Prof., Dept. of Leukemia Focus: Myeloproliferative neoplasms (MPN) Institution: MD Anderson
...
Dr. Ruben Mesa &Dr. Estelamari Rodriguez Dr. Estelamari Rodriguez and Dr. Ruben Mesa are respected oncologists in their fields, but in this video, they give a much deeper and personal look into their WHY for treating cancer. They also detail the importance of having representation and diversity both in doctors and in patients, especially when...
Dr. Saad Usmani, Chief of Myeloma Service at Memorial Sloan Kettering, talks about CAR T-cell therapy, bispecific antibodies, novel therapies and combination therapies.
...
Dr. Vincent Rajkumar, a hematologist oncologist at the Mayo Clinic, talks about drug pricing and the impact of high prescription drug costs on patients and families.
...
Long-time myeloma patient and advocate, Jack Aiello, leads the conversation with Dr. Joshua Richter, Multiple Myeloma Director for Blavatnik Family Chelsea Medical Center at Mount Sinai and Dr. Muhamed Baljević, Plasma Cell Disorders Research Director for Vanderbilt-Ingram Cancer Center.
Dr. Matthew Matasar, chief of blood disorders at the Rutgers Cancer Institute of New Jersey and RWJBarnabas Health, sat down with Dr. Samantha Spiegel, a Hodgkin’s lymphoma patient, to discuss some of the most exciting news coming out of ASH 2022.
The Patient Story founder and DLBCL advocate Stephanie Chuang leads the conversation with Dr. Josh Brody, who leads the Lymphoma Immunotherapy Program at Mount Sinai’s Tisch Cancer Institute, and Dr. Lorenzo Falchi, an oncologist at Memorial Sloan Kettering Cancer Center.
Top breast cancer doctors Dr. Paolo Tarantino with Dana-Farber Cancer Institute and Dr. Lola Fayanju with Penn Medicine discuss the big highlights from this year’s San Antonio Breast Cancer Symposium.
Multiple myeloma specialists Dr. Ajai Chari with Mount Sinai in New York and Dr. Sandy Wong with the University of California San Francisco discuss the big buzz at this year’s ASH: bispecific antibodies.
Dr. Serge Verstovsek and Dr. Naveen Pemmaraju discuss cutting-edge treatments and therapies, and combination therapy as a focus in treating myelofibrosis.
Patient advocate Jack Aiello and hematologist Dr. Shaji Kumar discuss what high-risk smoldering patients can do to delay or possibly avoid progression to active myeloma.
Dr. Chadi Nabhan shares how he got involved in the Monsanto trials, what he learned from the, and why he decided to write a book about the whole experience.
Patient advocate Valarie Traynham and Dr. Shakira Grant discuss the barriers many Black patients face, how it impacts their care, and what can be done to help improve their outcomes.
Medical oncologist Alok Tewari, MD, PhD, who specializes in cancers arising from the genitourinary tract, discusses what patients need to know about testicular cancer.
Hematologist Alfred Garfall, MD, MS, from Penn Medicine discusses with multiple myeloma patient advocate Jack Aiello the advancement of immunotherapy for multiple myeloma, the difference between CAR T-cell therapy & bispecific antibodies, and the role of bispecifics in the myeloma toolkit of immunotherapies.
...
Patients and doctors share their real-life colonoscopy experiences...
Cancer Survivorship Care Plan for Hodgkin Lymphoma Patients...
Nicole Lamanna, MD, from Columbia University Medical Center, Spencer Bachow, MD, from Boca Raton Regional Hospital, and CLL patient Lisa P. discuss the importance of building a strong support system and collaborating effectively with multiple doctors.
...
Leading experts Estelamari Rodriguez, MD, MPH, from the University of Miami Sylvester Comprehensive Cancer Center, Jason Porter, MD, from West Cancer Center & Research Institute, and Terri Conneran, founder of KRAS Kickers, discuss the latest in lung cancer treatments and ongoing clinical trials.
...
Patient advocate Cindy Chmielewski, experts Dr. Carl Ola Landgren and Dr. Caitlin Costello, together with clinical trial nurse Christen Hawthorne uncover groundbreaking insights on the latest multiple myeloma treatments and clinical trials.
...
Patient advocate Ruth Fein Revell, experts Dr. Angela Fleischman and Dr. Ruben Mesa, together with clinical trial nurse Melissa Melendez delve into the cutting-edge realm of myelofibrosis clinical trials.
...
Patients, care partners, and a panel of CLL experts including Dr. William Wierda, Dr. Nicole Lamanna, Dr. Adam Kittai, and Jackie Broadway-Duren share the latest in CLL research, clinical trials, treatments, and comprehensive care strategies.
...
Palbociclib Side Effects & Patient Stories Palbociclib, commercially known as IBRANCE, is a treatment for a specific kind of metastatic breast cancer, or breast cancer that has already spread to other parts of the body, known as HR+/HER2- mBC. Palbociclib may be able to renew patients’ hope and offer them a greater sense of possibility...
Patient advocates Cindy Chmielewski and Jack Aiello, and experts Dr. Rafael Fonseca and Dr. Susan Bal discuss promising multiple myeloma treatment options.
...
Dr. Matthew Matasar, chief of blood disorders at the Rutgers Cancer Institute of New Jersey and RWJBarnabas Health, discusses some of the most exciting news coming out of ASH 2023.
Dr. Andy Evens from Rutgers Cancer Institute discusses how to reduce the toxicity of Hodgkin’s lymphoma treatments so patients can live their best lives after cancer.
A Conversation with a Personal & Professional Caregiver
My dad passed away in May 2019 from cancer. Part of me wanted to just crawl into bed and not get up. There was another part of me that was incredibly driven, though, because I know firsthand why this work that we’re doing is so important.
I knew why somebody needed someone to answer those phone calls and emails.
Kris Curl Johnston
As a professional caregiver, there’s a line. Essentially, the line is that you don’t matter. You are there for these individuals. That is a part of the professional code. ”
Name: Kris Kurl Johnston
Title:
Sacramento Citywide Oncology Phase I program (SCOPE)
Program manager
Philosophy: There is a line between personal and professional. Kris takes her personal caregiving experiences and uses them when helpful and relevant in her professional caregiver position.
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Background
Your work as a clinical program manager
We have a very unique program where we work very closely with our community oncologists in the region. They all perform clinical research themselves, but they’re not equipped to do the very early stage clinical trials. We are their phase I center and I am their primary contact.
We also have the Scope website. Some oncologists will call about a trial, but others will just have their patients call or go to the website. When working with the physicians, I’m their primary contact for the inquiries that come through the website.
I also have many other duties including program development and triaging and overseeing clinical trial inquiries.
Your background
After I graduated from UC Davis with my bachelor’s degree, I got a job doing medical records for pediatric oncology. I worked my way up. I started training for clinical research.
Pediatrics was very challenging. My hats are off to the pediatric oncologists and nurses.
I jumped to adults. I continued my training here at the UC Davis Cancer Center. At that time, clinical research coordination was very low-paying. My student loans were coming due. Then, I got recruited into the pharmaceutical industry. I really enjoyed it, but it got to the point where I was on planes every day.
When I decided to get married and have a kid, that wasn’t really an option anymore, so I came back to UC Davis, and I’ve been here since.
Being a Personal Caregiver
Can you talk about your experience as a personal caregiver
I went with my aunt to her appointments when she was diagnosed. We got her medications and went over all the antiemetics (drugs) and how to take them because I was going to have to be out of town all weekend.
There are very specific directions to how you take those drugs that keep you from throwing up constantly, so I wanted to make sure she knew how to take them.
She was nodding and saying, “Yup. Yep. Okay. Yeah.” I had absolutely no idea to what degree she was not getting it. I set up a nurse friend to be on call in case she needed anything while I was gone.
I came back to town on that Monday, and I got a call from my aunt. “Are you back in town?” She sounded awful. I said, “Yeah, what’s going on?”
She didn’t get any of it. She didn’t take any of her medication right. She had been so sick all weekend and didn’t call anybody because she didn’t want to be a bother.
Helping a patient
As a caregiver, even though you have this amazingly competent person you’ve watched and admired all your life, when it comes to their own diagnosis and medications, they might not be on top of it.
You have to watch out for that and make sure they understand what to do.
Caregiving a second time
Right after my aunt finished her treatment, my dad was diagnosed. I work with all these oncologists in the area, and I have all their cell phone numbers because we’re texting back and forth about their patients.
When my dad ended up with a recurrence, he was hospitalized at a smaller rural hospital. They kept saying, “It’s just a bowel obstruction, don’t worry.” I said, “There was a scan that was just done. Can we get that?”
They didn’t even know where to go to get it. I needed answers. I was getting frustrated.
I thought, “I know the oncologist downstairs. I should go get them.” I didn’t though. I called the oncologist down here in the valley, and I let her know what was going on in a message. She essentially scolds me for not using her cell phone and for not walking downstairs to get that other oncologist I knew.
I felt like I was going to be taking advantage of those professional relationships. I was scolded for not taking advantage of it, and I thought that was amazing.
Navigating the caregiving relationship as the child of a patient
The other thing I realized was just how much my dad wouldn’t tell me because I was his daughter. I had to tell him, ‘Dad, I’m going to cry sometimes. You still have to tell me what’s going on.’
I had to make him understand that I needed to know what was going on so I could get him the help he needed. That’s very common and very difficult in adult child caregiver dynamics.
Advice for other adult child caregivers
It’s a very individual thing. My aunt, who had cancer and is my dad’s sister, had things she knew she couldn’t handle hearing regarding her brother. She avoided them.
We can all take a lesson from her. You have to know yourself well enough to know what you can and can’t take. If you can’t take hearing something painful, get another family member or friend involved.
In my case, with my dad, I could take it. I knew I could handle it. I just had to assure my dad that even if I cried, it didn’t mean I wasn’t handling it. You have to know what you can take in the moment.
Be very open and honest with the professional caregiver. I was very open with my dad’s oncologist and nurses. I said, ‘Look. He may not tell me everything. He may not tell you everything. Let’s compare notes.’
Asking for help outside of the oncologist
Remember that the oncologist is only going to treat the cancer. If the patient has pain, depression, or anything else going on, they’re not treating that. Ask for a referral.
The oncologist doesn’t specialize in other areas of medicine and sometimes they forget to ask. Speak up. They’re happy to refer you to someone who can help.
An extremely important question you can ask is, “Is there any other support we can seek out here?” Most institutions have social workers, navigators, and support programs.
Professional Caregiving
There’s a line between personal and professional caregiving. Can you talk about how it blurred for you?
As a professional caregiver, there’s a line. Essentially, the line is that you don’t matter. You are there for these individuals. That is a part of the professional code.
The challenge is that the professionals end up burning out because we get so good at pushing ourselves to the side in order to keep a clear head, that we lose ourselves.
My dad passed away in May 2019 from cancer. Part of me wanted to just crawl into bed and not get up. There was another part of me that was incredibly driven, though, because I know firsthand why this work that we’re doing is so important. I knew why somebody needed someone to answer those phone calls and emails.
I found that I went from never drinking to drinking every day. I was tempted to take some of my son’s ADHD medication so I could keep the necessary pace of our days. Early stage research is only for people with advanced cancers, which means every phone call is an emergency. We have to move quickly.
There’s this weird mix of personal and professional conflict within myself because I am a professional, but this work affects me personally. So, I’m taking these calls from people who are saying, “You have no idea what we’re going through.”
When I decided to breach that professional line just enough to say, ‘No, we do know exactly what you’re going through,’ I found that they could breathe again.
Cancer doesn’t discriminate. It can impact anyone personally. It’s very important for patients and caregivers to remember that we’re all in this together and we understand. ”
How can caregivers combat burnout?
It was monumental for me to recognize burnout and to label it. I had to realize I’m not a wimp, and it’s a real thing. The mechanism by which it happens is forgetting that you exist as a human being.
Remember that you are an individual, no matter how much or how often you put yourself on a shelf to care for other people.
Then, it’s about keeping little goals just for yourself and celebrating every moment. Labeling it, remember I am an individual who is important, and maintaining little goals just for me are the three things that brought me back.
Always keep a little bit of you whether you are a personal or professional caregiver. It’s okay to blur the lines a little to make a human connection. That will help you navigate this more than anything else.
Recognizing burnout
I was trying to come back from the edge. I found myself having a drink at lunch and hoping no one smelled it on me when I got back to work. I knew something had to give.
I coordinate some of the professional education for our group, so I had requested the chief wellness officer for the health system to come in to speak to us. He usually talks to physicians, but he was happy to come talk to us because he was curious to see how burnout in physicians translated to us.
He came in and discussed it. It was not only an “a-ha!” moment for me, but for so many of us. Afterwards, I went up and talked to him and some others. The feedback I got was, “Oh my god, I’m burnt out,” from so many of us.
We all learned we have to bring ourselves back a little bit more every single day.
Advice about clinical trials
Clinical trials are not just for people with no other options.
Without clinical trials, we have no new treatment. Many clinical trials actually require no prior therapy or only one prior therapy. There are eligibility requirements, so it’s important for patients to discuss trials with their physician.
The most important thing is to realize that clinical trials are simply another treatment option. Once you realize that, it’s about talking with your oncologist who’s treating you. Ask. ‘What about clinical trials?’
A lot of times there are clinical trials going on with the doctor who is treating you. If not, start at the biggest academic center near you. Find the phone number for clinical trials. Call. Go to their website. You don’t want to be flying somewhere and having to find a place to live if you don’t have to. Find one near you where you can live at home or with a relative.
There are websites and services out there like the American Cancer Society and other organizations with clinical trial matching programs. It’s important to speak with someone to ensure the information is up to date.
Dr. Irene Ghobrial is an experienced hematologist and oncologist who specializes in myeloma. In this interview with The Patient Story, Dr. Ghobrial talks about treatment for those with MGUS, smoldering, and active myeloma, and where she thinks research is headed.
Name: Dr. Irene Ghobrial, MD
Roles
Clinical Researcher
Professor of Medicine
Experience: ~15 years
Professor of Medicine, Harvard Medical School
Director, Clinical Investigator Research Program
Fellowship
Mayo Clinic, Graduate Medical Education, Hematology & Oncology
Residency
Cairo University School of Medicine, Pediatrics
Sinai-Grace Hospital of Detroit, Internal Medicine
MD – Medical School Education
Cairo University School of Medicine
Approach with patients: Unique approach for each patient in order to prevent disease progression
We’re trying to develop better targeted therapies so we’re not just using myeloma drugs earlier.
We’re actually trying to develop what’s called prevision intervention which are new therapies, vaccines, and other ways to make the immune system stronger so it can prevent progression without any chemotherapy.
My name is Dr. Irene Ghobrial. I’m a professor of medicine at the Dana-Farber Institute and Harvard Medical School. I’ve been here for about 15 years.
Over the last few years, we’ve said multiple myeloma is a cancer where treatment doesn’t start until a patient is symptomatic. These symptoms are lytic lesions, fractures, anemia, and kidney failure.
It didn’t make any sense. We were all trained this way. But for any other cancer, it’s not like that. If you have a woman with early breast cancer, you never tell this woman, “Wait until you have metastasis everywhere.”
At Dana-Farber, we’ve said, “Why don’t we change that?” We are finding better biomarkers and developing clinical trials for earlier intervention and prevention of precursor conditions like Monoclonal Gammopathy of Undetermined Significance (MGUS) and smoldering myeloma.
Can you talk about The Promise Study?
We expanded that to start the first screening study. It’s called The Promise Study. We got 10 million dollars to start the first screening study in the US that looks for myeloma in individuals who are at risk.
Those at high risk are African Americans and first-degree relatives of those who have myeloma.
We’re screening 50,000 individuals. We’re trying to encourage people to sign up online. It’s really simple. They get a kit, and take it to a lab. They take care of the rest. If they’re positive, we call them and help them. If they’re negative, of course, we let them know.
The hope is that we screen early, prevent early, and in the future, we don’t even diagnose myeloma. The goal is to always prevent it early.
What does the treatment look like for someone with MGUS?
If they are low-risk, we don’t want to treat them. We just observe them, and we try to figure out why their myeloma isn’t progressing and learn from that to help others.
Maybe there is something in their immune system that is so good that it’s preventing the disease? Is there something in the early tumor cells that we can understand?
For higher risk MGUS, we have an antibody treatment called Daratumumab. We have more studies coming along.
What about treatment for smoldering myeloma?
For smoldering myeloma, we have multiple clinical trials including active myeloma treatment, but we’re just starting it earlier. If someone is extremely high-risk, then we go ahead and start them even if they have smoldering myeloma.
Are you curing people before they have active disease?
The word cure is very hard. We don’t have evidence that we have cured anyone, but we are definitely delaying progression.
Instead of having fractures in two years, can we maybe prevent them for 10 to 15 years. In that case, hopefully we’ll have even better drugs and options at that point. The hope is to cure people, but we’re not there yet.
What does it mean for someone to be high-risk?
Currently, the markers are all tumor markers, meaning your M-protein is very high, your light chain ratio is high, or your cancer cell count in your marrow is high. Of course if your tumor cells are high, you are at high risk, but there are people whose numbers aren’t that high who progress really fast.
We’re developing better genetic markers to find out just how high someone’s risk is based on more than just tumor cell count, but more biologically.
We’re trying to see if they have a bad cytogenetic abnormality or bad DNA changes that predict whether the cells like to proliferate more quickly.
We already did something called next generation sequencing with 200 patients. We have data already that shows those patients who have certain markers would progress much faster. We’re ready to put that in publication.
We’re hoping this would be a test we can provide clinically so people can find out at their own physician’s office if they have those markers and be labeled as high-risk in the future.
What other tests are you working on?
We have something called liquid biopsy where instead of doing it as a bone marrow biopsy, we test the blood sample. You can test all those markers in the blood.
That would be much easier because the last thing you want is multiple bone marrow biopsies for patients. Hopefully, we can just use the blood in the future for testing.
Because MGUS and smoldering myeloma have minimal DNA in the blood, we’re working on better technologies that can detect in a much more sensitive way. We still have some work to do before those tests and screenings can be launched to patients.
Can you make a distinction between MGUS, smoldering myeloma, and active myeloma?
Active myeloma is characterized by four criteria. Those are hypercalcemia, anemia, lytic lesions, and renal failure. We have a few more now like having a high tumor burden or having lesions on the MRI. Something like this would be considered active myeloma and should be treated.
Anything before that would be a precursor condition. The difference between MGUS or smoldering myeloma is having 10% of plasma cells in the bone marrow. Less than 10% is MGUS, and more than 10% is smoldering.
The chances of progression are very different. For MGUS, it’s a 1% chance per year. For smoldering, it’s a 10% chance per year.
Where do you see the research going next?
First, we need to develop better biomarkers. We’re not there yet. This is just the first step. We’re trying to understand a lot of different things.
We’re trying to develop better targeted therapies so we’re not just using myeloma drugs earlier, but we’re actually trying to develop what’s called prevision intervention which are new therapies, vaccines, and other ways to make the immune system stronger so it can prevent progression without any chemotherapy.
The hope with that is that they will preventative and non-toxic. We’re hoping to make the screening study the standard of care where you go to the doctor at age 40 or 45 and get screened for myeloma.
We’re trying to understand why certain families have a higher chance of myeloma, why African Americans have a higher chance, and whether what we eat and the microbiome plays a factor.
What’s your advice for someone who is newly diagnosed with smoldering myeloma?
First, I would say go see a specialist. Not everyone knows smoldering myeloma. Do your homework, research, and look into clinical trials. We’re happy to assist everyone. This is why we have a whole center for prevention of progression.
Having patients engaged and empowered is important. Patients can play a huge role in research, so get involved. If you have been diagnosed, get qualifying immediate family members to enroll in the Promise Study.
If everyone is involved and excited about the research, we will move much faster.