Cancer Survivor Stories
Brianna: Surviving Cancer is Why I Became an Oncology Nurse

The nurse told me, ‘Everything is different now. You’re just going to have to face it. Things aren’t going to be normal, but you can find a new normal. You can get through this. You’re young and healthy. You got this.’
That really helped me get into a positive mindset. That talk with her was what really put me on a path to getting something out of cancer. She was the nurse who inspired me to be a nurse. If not for her, I don’t know that I would be.
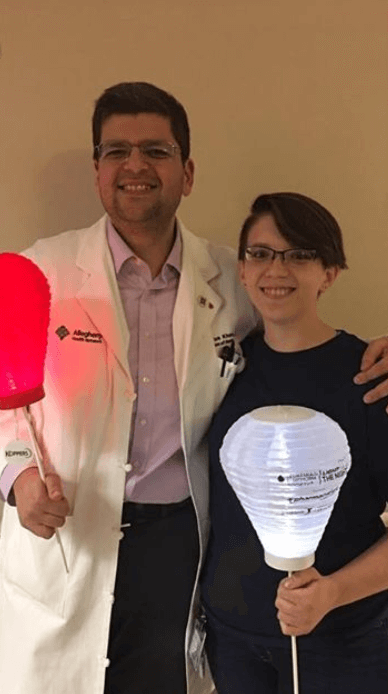
Brianna Banachoski, AHN West Penn Hospital
Becoming a Nurse
When did you know you wanted to be a cancer (oncology) nurse
I remember it like it was yesterday. It was the night I was admitted to the hospital. This was the night my abdominal wound opened, and I was due to start chemo the next day. I had a complete mental and emotional breakdown.
There was so much in front of me, and I didn’t know how to handle any of it. My mom was with me and was at a loss, so she went and got my nurse. I had requested chicken broth, so she brought that in.
The nurse told me, ‘Everything is different now. You’re just going to have to face it. Things aren’t going to be normal, but you can find a new normal. You can get through this. You’re young and healthy. You’ve got this.’
That really helped me get into a positive mindset. That talk with her was what really put me on a path to getting something out of cancer. She was the nurse who inspired me to be a nurse. If not for her, I don’t know that I would be.
That planted the seed. It grew over time. Once I was in remission, I didn’t want anything to do with cancer. I wanted to be far away from it and do a desk job with easy hours that wasn’t stressful at all. I’d just gone through two lifetimes of stress and didn’t want any more.
I kept going back to that moment and thinking, ‘I have to do something with what I went through. I can’t just put all that experience behind me and let it go to waste.’
I kept thinking about that moment with that nurse. I hoped I could be that person for somebody. There was one day when it just clicked. I wanted to make a difference with what happened to me.
Becoming a nurse
I did an accelerated program because I already had a bachelor’s degree. I got my bachelor’s in nursing in 16 months.
Now I work at the same hospital that I was treated at on the same floor. My supervisor who interviewed me was the nurse that gave me my first chemo.

Day in the life of a Hem/Onc nurse like
We give out meds. We administer a lot of blood products. Our patients don’t have immune systems, so if they spike a fever, we draw blood cultures and put them on antibiotics right away.
You have to have a sharp eye on our floor because things can go downhill very fast when your patients are sick like ours are. You have to know what to look for and how to react.
You have to know that abdominal pain could be a sign of a bleed instead of just a stomachache. You have to know what to do. You have to know how to relay your assessment to the doctors.
We do a lot of chemo. Not me yet, but we do a lot of chemo and blood products. Sometimes we’ll have a stem cell transplant, which I think is exciting. Some people call them glorified blood product infusions, but I think it’s neat.
What’s your daily schedule like
6:30am – Arrive to work early to look at patient charts and plan my day according to medications, need for blood and electrolyte replacements, procedures, etc.
7:00am – Clock in and get report on my patients from night shift nurses.
7:30am – Bathroom and coffee for me – you can’t take care of patients unless you take care of yourself.
7:45am – 10am: Morning assessments and med pass. This is when I see all of my patients (we get 3 or 4 patients per nurse on our unit), talk with them, assess them, tell them the plan for the day, and administer morning medications.
10:00am-11:00am: I try to get all of my charting done by 11. It doesn’t always happen, sometimes the morning is too busy. But on an ideal day, that’s what happens.
11:00am: On Mondays, Wednesdays and Fridays we have rounds with the treatment team. This is when the nurses take turns sitting with the doctors and discussing our patients. We tell the doctors what our patients need and ask for orders that we need so that we can do our job.
This is also a good time to ask questions, because all of the doctors and PAs, a pharmacist or two, a social worker, and the transplant coordinator are present.
I ask a lot about treatment plan and length of stay, so that I know what the game plan is for my patient.
11:00am-7:00pm: This varies depending on the day. During this time, I give meds when they’re due, check on my patients every hour, change central line dressings if IV team isn’t available to do them, administer blood products (I do this earlier if I can, but the blood bank usually doesn’t have them ready until at least 10), and handle any changes in status in my patients.
This is also when a good portion of admissions and discharges occur, although those can also happen at any time of day or night.
7:00pm-7:30pm: I give a report to the oncoming shift, and I go home.
Stem Cell Transplants
What is a stem cell transplant
You have to be in remission first. You get induction chemo, go into remission, get maintenance chemo to keep you in remission, then you get chemo that kills cells in your bone marrow, and then you get a transplant with new cells so the cancer doesn’t come back.
If it’s successful, that’s the cure for things like leukemia because your old cells can’t come back.
In the days beforehand, the patient will get chemo to wipe out their bone marrow. Most chemo wipes out peripheral cells, but this chemo wipes out bone marrow, and it doesn’t come back. You have to get a transplant afterwards or else you have no cells growing in your marrow.
If patients are younger and healthier, they might get total body radiation. It’s very intense, very high-dose radiation. The side effects are pretty severe. They might experience burning, nausea, diarrhea. or sores in their mouth and throat.
On “day 0,” they get the transplant. The days leading up to it are -3, -2, -1, etc. Day 0 is your new birthday.
After the transplant goes well, we bring the patient a small cake, and we all sing happy birthday. That’s my favorite part.
The transplant itself is like a blood infusion. It’s straightforward. It’s just a gravitational infusion.

What happens after the stem cell transplant (SCT)
In the days after, patients’ numbers will drop. They start to experience all the side effects from chemo and radiation. That’s when patients are the sickest and need the closest monitoring.
Around day 14, counts start coming back up and the marrow cells start engrafting, which just means the transplanted cells are taking hold and it’s working.
It’s about a 30-day process in total with the recovery and everything usually. We manage symptoms for them in the hospital.
Graft vs. host disease (GvHD)
Graft vs. host disease is similar to organ rejection in other types of transplants except it works in the opposite direction. Instead of the body rejecting and fighting against the transplanted organ, the transplanted stem cells attack the body’s organs.
GvHD can be acute and happen within the first 30 days after transplant, or it can be chronic which means it can happen later down the road. It can affect pretty much anything in your body. Mostly, we see GI tract issues and skin problems.
Emotional and Mental Impact
How does it feel being a nurse for patients who are going through something similar to what you’ve gone through?
It feels really good. It feels like where I’m supposed to be.
Even though these patients don’t necessarily have the exact same diagnosis and aren’t getting the exact same treatment, we still have a lot in common.
I have to read the room before I share my story with a patient because they can respond positively or negatively depending on their own outlook, but when I do get to share it with a patient, it makes our bond that much stronger. They usually open up to me more after that.
One of our marketing hashtags for our health system is #LivingProof. I have one patient who calls me his living proof. That makes me feel like I’m really making a difference.
Aside from all the nursing stuff I do every day, stuff like that is what makes me feel the most proud.
I didn’t set out to work in nursing with the intention of sharing my experience with patients to change their lives. I never intended on sharing my story with patients unless I felt it would benefit them or they asked to hear it.
I never thought I could make a greater impact than any other good nurse, but I do think that if I can use what I went through and my experiences to make a difference in at least one patient’s life, then I have been successful.
How does it feel to have a patient go into remission and get to go home
It feels great. We’ve had a lot of patients. The ones that come to mind specifically are the ones that were doing the worst because I spent so much time taking care of them.
To think about all the patients we see who have gone through remission and gone home is amazing.

Keeping work at work
It’s hard work. It wears on you as a new nurse even. You have to watch out for your own mental health because it can really wear on you.
It helps to have such an amazing team of nurses. I’m biased, but I really think we are the best. We’re all really supportive of each other and really care about our patients.
They say it takes a special kind of person to do our job, which sometimes I disagree with, but on the harder days, I really do agree.
When I see how we all come together and care for each other and our patients, it makes me think, “Maybe you do have to have a little something special to be able to do this.”
It’s a lot of self-care. Eating well and exercising helps. I try to do things I enjoy doing outside of work so I’m not always thinking about work even when I’m not there.
I like to go horseback riding, and I’m working on photography. I have little things like that to make me happy and get fulfillment outside of work.
Brianna’s Cancer Story
If you would like to follow along with Brianna’s photography or read her patient story, click here for Brianna’s Patient Story.

What Is a Clinical Trial Really?
Clinical trials can be confusing to navigate, so The Patient Story partnered with the Leukemia & Lymphoma Society (LLS) to discuss what a clinical trial is, the phases of a clinical trial, and figuring out the logistics of paperwork, scans, and finances.

Julie McFadden, Hospice Nurse
Hospice nurse: For last 5 years, helps patients and families understand end of life options
Experience: 14 years
Focus: Introduction to hospice, education

Jennifer Hagerty, Cancer Clinic Nurse
Clinic nurse: works mostly outpatient
Experience: 12 years
Hospital size: Large teaching institution
Brianna Banachoski, Hem-Onc Nurse
Nurse: works 12-hour shifts on blood oncology floor
Experience: was a lymphoma patient, became a nurse in early 2019
Hospital size: mid-range

Bernadette Lucas-Burch, Nurse Navigator
Nurse Navigator: help cancer patients and caregivers at diagnosis through treatment.
Experience: 35+ years
Hospital size: Mid-range but largest in the region