Alex Oshmyansky | Cost Plus Drugs

Alex Oshmyansky, MD, PhD, is the Founder and CEO of the Mark Cuban Cost Plus Drug Company. He shares the catalyst that made him pivot from being a practicing physician to starting a pharmaceutical company.
In this conversation, he talks about the exorbitant costs of medicines along with Dr. Vincent Rajkumar, a hematologist oncologist at the Mayo Clinic, and the complicated and convoluted path from pharma to patient, and what his company is doing to offer drugs at the best prices possible.
The interview has been edited only for clarity.
Introduction
Alex Oshmyansky, MD, PhD: [I’m] a board-certified diagnostic radiologist. I have a PhD in applied mathematics. When I was a kid, I was going to be a string theorist, so a high-energy particle physicist. I was being fast-tracked into that. With all the wisdom of a teenager, I decided that wasn’t going to be impactful enough in the real world so [I] made a hard shift [in] my last year of college and decided to major in biochemistry instead.
I graduated at 18, went on to medical school and completed an MD-PhD program. [I] went on to do my internship in general surgery at Brigham and Women’s Hospital and then radiology residency and pediatric radiology fellowship at Johns Hopkins.
At Hopkins, I was working with a pulmonologist on a research project. One day, he came in infuriated because two of his patients died over the same weekend. They both needed a drug called Bosentan, which treats primary pulmonary artery hypertension — hypertension specifically of the big blood vessel that comes out of the heart and goes to the lungs — and they both needed it urgently.
At the time, the medication cost $10,000 for a month’s supply, despite the fact that it was long off-patent [and] was a generic product at that point. They were meant to apply to a patient assistance program set up as a nonprofit by the manufacturer who made the product, got caught in the red tape and both of them tragically died [on] the same weekend.
I had been angry about these topics for some time and you think that’d be enough to set me off. But what really became the straw that broke the camel’s back was Martin Shkreli.
In 2015, he was a social media villain-of-the-day type [of] guy. He was a hedge fund manager who took over a pharmaceutical company and increased the price of a drug called Daraprim — generic Pyrimethamine, primarily used by indigent patients or immunocompromised — by over 10,000%, hundreds of dollars a tablet.

I got very mad and some of my friends, who are also doctors, [also] did. We decided very naively, “Let’s set up a nonprofit pharmaceutical company that will make drugs [and] sell them at cost.” While working as a doctor, [I] went out for the better part of three or four years trying to raise funding for the nonprofit and did not succeed. Failed spectacularly — raised $0 beyond what I put in myself.
Eventually, [I] got talked into converting it to a for-profit public benefit corporation — but with a registered public mission with the state. [I] eventually sent Mark Cuban a cold email. I sent it on a whim and surprise, surprise! He reads all his emails. And the rest, as they say, is history.
Stephanie, The Patient Story: What’s really fascinating is Martin Shkreli became the symbol but what a lot of people didn’t realize was that he wasn’t the exception and he became the villain. There were so many other things happening.
Alex, Cost Plus Drugs: [He] seems to have a histrionic personality [and] likes attention. He’s really quite a small fish in a big pond of people who are much worse actors than he was. He took much of the blame because he seemed to enjoy it. But he was not the biggest actor in this space by far.
The path is incredibly complicated. It’s very convoluted and that’s by design.
Alex Oshmyansky

The path from pharma to pharmacy
Stephanie, The Patient Story: Which I think would surprise, still to this day, so many people. This is where there’s a lot of misunderstanding. I didn’t learn about the term PBM (pharmacy benefit manager) until fairly recently. There is this path that goes from the pharmaceutical companies — with the research and development of these drugs — to the pharmacies where you and I go to pick up the drugs and the prescriptions. Could you summarize what happens? What is in this path here?
Alex, Cost Plus Drugs: The path is incredibly complicated. It’s very convoluted and that’s by design. There’s a layer of financial engineering that takes place between you and actually purchasing the product.
Pharmacy benefit managers are firms [that] are outsourced to by insurance companies to decide which products are covered by insurance. They manage all the payments. Back in the 1980s, before computers were as widespread, they were initially there to literally process payments. They would get paid to do the paperwork when a prescription insurance claim was submitted.
What they (pharmacy benefit managers) realized was… the best way to make the most money was for the drugs to be as high a price as possible to start out with before they started negotiating down.
Alex Oshmyansky
What they realized over time was, since we’re paying for the drugs anyway, we can collectively bargain for the drugs. They turned into negotiators for drug prices. There’s a big to-do recently about Medicare negotiating for drug prices, which is a great thing, but we technically already have professional negotiators doing it. Those are the pharmacy benefit managers.
Eventually, what they realized was, The way we’re getting paid is we take a percentage of the savings. That’s how they structure their deals. The best way to make the most money was for the drugs to be as high a price as possible to start out with before they started negotiating down.
Imagine you wanted to buy a [car] but you hate negotiating at the car lot. It’s miserable. The guys are jerks. “Oh, I have to go to the back and talk to my manager.” Everybody hates that. Somebody comes up to you and [says], “Hey, I will do the negotiating for you and in exchange, I get 10% or 20%,” or whatever the amount of money they save you. You’re like, “You know what? That’s worth it to me. I hate negotiating.”
The negotiator comes back and says, “Hey, amazing news. I got you a great deal. I got you 90% off of your [car].” “Oh, my God, That’s amazing. How did you do that?” “I’m really, really good at negotiating.” Come to find out the sticker price on the [car] was $1,000,000 and you’re paying $100,000 for your [car] plus the fee from the negotiator, which is another $90,000, so you’re paying $200,000 all of a sudden for your [car]. That sounds like a crazy, over-the-top example, but it really happens.
That delta between $3,200 and $39 is being taken by somebody and it’s actually not the pharmaceutical manufacturer.
Alex Oshmyansky
The example drug that I use all the time — because it’s the most extreme edge case — is a product we offer called Imatinib, which is a chemotherapy product. It’s a tyrosine kinase inhibitor for chronic myelogenous leukemia and you need to be on it for many, many years. The list price, the so-called average wholesale price, is $10,000 for a month’s supply.
Now, if you get it through your insurance and you have a high deductible plan, it’ll be “adjudicated” at between $2,000 and $3,200 as the negotiated discount price plus the margin for the PBM. Meanwhile, if you get it from the Mark Cuban Cost Plus Drug Company, it’s $39 for a month’s supply. That delta between $3,200 and $39 is being taken by somebody and it’s actually not the pharmaceutical manufacturer. It’s the intermediaries and the pharmaceutical supply chain taking a percentage of the rebate. It’s just one of the many, many scams [that] has evolved over the past 30 years to take advantage of the sick and vulnerable and it’s absolutely morally repugnant.
Stephanie, The Patient Story: We know about pharma companies and the R&D that happens there. There’s a price set. Can you describe the path?
Alex, Cost Plus Drugs: Basically, the wholesalers do take a markup. On specific products, it can be a very, very high markup. Our initial product, Albendazole, an antiparasitic drug, is available from us for $30 for two pills and a complete course of treatment tends to be two pills. But, as far as we could tell, about $70 a pill from the pharmaceutical wholesalers if you purchase it directly from them.
There is a lot of inflation that happens at the wholesaler level. As a general rule of thumb, the price of a drug approximately doubles.
Alex Oshmyansky
There is a lot of inflation that happens at the wholesaler level. As a general rule of thumb, the price of a drug approximately doubles once you purchase from a wholesaler. That sounds like a lot and it is. It’s perhaps a bit too much but at least they serve a function. They send the products around the country.
The really egregious part of the payment processing comes from the pharmacy benefit managers who administer the payments to pharmacies on behalf of insurance companies. They also claw back payments from the pharmacy so the money goes both ways. They take money from the insurance companies, who in turn partially own them. They set up subsidiary companies called rebate aggregators in Switzerland that have more fees. There’s this spider web of interacting actors.
This is Adam Fein’s from Drug Channels. This is his famous slide, which is a simplified version of the way money flows in the pharmaceutical industry.
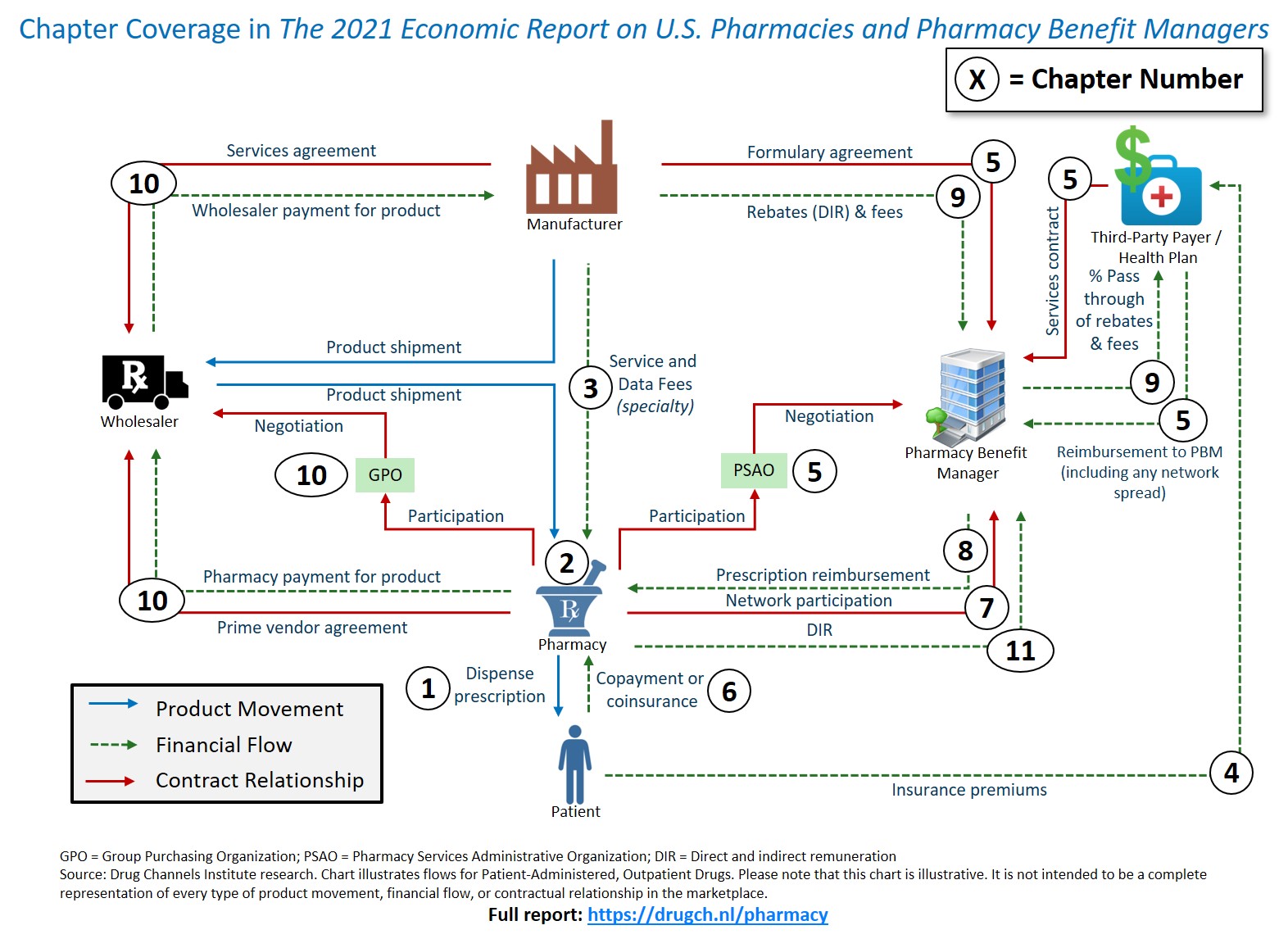
Stephanie, The Patient Story: This is simplified?
Alex, Cost Plus Drugs: Yeah, this is reductive. It’s an absolute mess, essentially.
The best way I can describe it is it’s basically a pile of spaghetti with lines going [in] every direction from all the various different actors — PSAOs (Pharmacy Services Administrative Organizations), GPOs (Group Purchasing Organizations), the insurance companies, the pharmacy benefit managers, patients — about the way money winds up flowing in the pharmaceutical industry.
The way I think about it is this is a feature, not a bug. When I was coming out of my PhD, I was recruited to be a quantitative analyst at a hedge fund. Back in 2007, I was interviewing for these jobs and they did technical interviews to see if you knew how to do [the] math. They showed me these incredibly complicated financial instruments — credit default swaps, collateralized debt obligations — and I remember saying out loud at one of the interviews, “Oh, so this is a scam.”
You start with bad debt. You add a layer of indecipherable, stochastic calculus on top of it and then magically, it’s good debt. No one can understand what’s happening so it lets you get away with the scam. Basically, the same thing is happening here. The system is so artificially complicated that it permits theft in the service of it.

Understanding drug pricing
Stephanie, The Patient Story: Okay, I know it’s very convoluted. Let’s just give an example for a $10 pill. Let’s say that’s what the pharmaceutical company has set the price on. Can you give an example of “roughly” what that could look like by the time it gets to us?
Alex, Cost Plus Drugs: On average, it’ll be about probably $20 from the wholesaler. Let’s say $10 just to keep the numbers round — it’s usually maybe $6 to $8. Let’s say at the pharmacy, it’s about $30. Then the price manipulation starts to happen and that’ll be the actual price at the end of the day.
There’ll be a number of artificial prices put on it depending on if it’s a brand name drug [or] a generic drug. Let’s say it’s a generic drug for the sake of argument. Generally, a generic drug is priced at a pharmacy benefit manager at about an 85% discount. They will say that the price of the drug is, in this case, $200 so that’ll be the price you see if you try to pay cash at a pharmacy without using a special program of some kind. It’ll be artificially inflated to $200 so they can negotiate it back down to $30 and then charge a little bit more for the service of negotiating.
Stephanie, The Patient Story: And there’s a rebate also involved?
Alex, Cost Plus Drugs: The manufacturer will have to pay a rebate to the PBM, who in turn takes a cut and forwards part of the rebate to the insurance company that’s paying the ultimate bill. But the insurance company had to pay the whole thing first. [Plus] the wholesaler, somewhere in the mix of all of this, holds the money for six months and makes money off of the interest. It’s a whole morass.
Finding the best price for your prescription
Stephanie, The Patient Story: The impact, of course, is not just these incredibly high, exorbitant costs to patients who, if they don’t have good insurance plans, are then left with the short end of the stick. They’re screwed over, honestly. Talking to Dr. Rajkumar, there’s all this confusion in terms of going to different pharmacies. Can you talk about that a little bit, too, and what Cost Plus Drugs is doing to try and help?
Alex, Cost Plus Drugs: As a general rule, the worst prices will be at your big national chain pharmacies. Usually, the best prices you get at retail tend to be from the supermarket chains because they’re hoping that the business actually drives traffic into the other parts of buying.
Obviously, I’m biased but generally, for most products, we tend to have the best price or at least close to it. We are a registered pharmaceutical wholesaler. We buy the products directly from the manufacturers at our flat 15% markup on top of it, a $3 dispense fee, and $5 shipping and handling at CostPlusDrugs.com. You can get any of about 1,000 generic products from our site as of today and we’ll be adding on brand-name products in the near future.

Always check with the manufacturer’s website. Discount card programs might be an opportunity.
Alex Oshmyansky
Stephanie, The Patient Story: What can people do? What about the people who don’t have their drugs covered yet by Cost Plus? I know you’re working on that. What can they do at home?
Alex, Cost Plus Drugs: There are a number of different resources. Always check with the manufacturer’s website. There may be a co-payment assistance card or other cash assistance program. They might not be the most convenient things in the world but, often, you can get the cash out of pocket. You have to pay down significantly that way.
Discount card programs, like GoodRx or SingleCare, might be an opportunity. They tend to be more generic-focused as opposed to brand-name products. I think those would be the two easiest things if you need a brand-name, on-patent medication.
Generally, the easiest way to know is if it has a really easy name to pronounce, it tends to be a brand-name medicine. Google the name of the medicine, check the manufacturer’s webpage, and see if there’s a program available to help you afford it.
If it’s a generic one, check CostPlusDrugs.com. But if we don’t have it, I would look for a discount card program; maybe there’s a discount available there. You can even ask your pharmacy, “Can I pay cash?” and see. Oftentimes, the discount cards are unnecessary and they’ll just sell you the drug cheaply.

The road ahead
Stephanie, The Patient Story: Thank you for the work that you’re doing. Obviously, people are seeing the benefits. How much work is there left to be done?
Alex, Cost Plus Drugs: Aside from the big three PBMs, there’s a host of small ones that are trying to do the right thing, be more transparent, [and] go back to the old model where they just take a small fee for doing the paperwork and electronic transmissions. And they see us as a real value add to differentiate themselves from the big PBMs who aren’t as open to working with us at this point.
The key is we work with them on our terms, which means no rebates [and] no spread pricing. The price you see on our webpage is the price everybody pays — [whether you’re] a single indigent patient on the street or [you have] a Blue Cross Blue Shield plan. Everybody pays the same amount.
Hoping long-term to change the status quo to something more sustainable… taking the pharmaceutical marketplace and making it like any other marketplace.
Alex Oshmyansky
Stephanie, The Patient Story: Between the brand name and the generic, has it been much harder with one than the other?
Alex, Cost Plus Drugs: The generic companies, it’s been easier to get ahold of those products just because there [are] more of them. There’s more competition and more people looking at ways to get their products across
The brand-name companies [are] not necessarily beholden to the PBMs but it’s a big risk to them to go outside of the PBM structure, which is not great. They’re not thrilled with it because, from their perspective, they do all the R&D, they take all the legal risks, [and] they take all the bad publicity from the public when people complain about high drug costs. And they’re like, Why are these companies getting a third of the revenue from our products? It’s insane.
At the same time, the status quo works for them. It’s a bit of a risk going with us. But I think in our conversations behind the scenes, they’re willing to take that risk at this point. They’re kind of sick of the status quo as well. We’ll be bringing them on in the near future.
Stephanie, The Patient Story: What is the next big vision of what this landscape will be like for people?
Alex, Cost Plus Drugs: Adding more and more products, brand-name products on a very tactical level. Beginning to work with insurance companies over the course of the next year — on our terms, of course.
Hoping long-term to change the status quo to something more sustainable based on taking the pharmaceutical marketplace and making it like any other marketplace — where you can see what the prices are and make rational, informed decisions as a patient and as a consumer based on real prices instead of make-believe numbers.