Lynn’s Small Lymphocytic Lymphoma (SLL) Story
When Lynn received his small lymphocytic lymphoma (SLL) diagnosis in 2013, he felt like he had lost his future.
Lynn saw a specialist at MD Anderson for treatment options. He is a strong proponent of seeing a specialist, especially after being a caregiver for his son when he was diagnosed with cancer in 1977.
A decade after diagnosis, Lynn reflects on his first symptoms, treatment and side effects and living life with a glass half-full mindset.
- Name: Lynn B.
- 1st Symptoms:
- Prolonged fever
- Night sweats
- Diagnosis:
- Small lymphocytic lymphoma (SLL)
- Non-Hodgkin’s lymphoma
- Tests for Diagnosis:
- X-ray
- Chest CT scan
- Bone marrow biopsy
- Treatment:
- Rituxan (rituximab) and Revlimid (lenalidomide) combination for 3 months
- Rituxan (rituximab) and Imbruvica (ibrutinib) combination – ongoing
- SLL 1st Symptoms and Diagnosis
- Introduction
- Symptoms and Tests
- The Diagnosis
- Receiving the diagnosis
- Processing the diagnosis
- Did you feel like you were losing things you had been looking forward to?
- Can you describe what you meant by feeling "marked"?
- Processing what it means to live with chronic cancer
- Can you explain the power of your doctor saying you could manage the cancer?
- Treatment and Side Effects
- Being a Caregiver and Lessons Learned
- More SLL & CLL Stories
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
SLL 1st Symptoms and Diagnosis
Introduction
Tell me about yourself
I’ve been married to my wife since 1970, so that makes 52 years. She’s a long-suffering lady, and we alternate being caregivers. I couldn’t have done it without her. We had five children and when you have children, you’re a hostage for the rest of your life. Every day she’s got to check on them!
I worked for an electric utility for 40 years. My training was in electrical engineering at a school in South Texas, and that was growth out of my hobby, which was ham radio. This has been an interest of mine for all these years.
In some senses, I was bi-vocational because when I went to work for the electric company, I also was a youth minister, served in several churches, and then later on was a volunteer music minister directing choirs and leading music in a church.
Music is one of my real loves, having grown up singing in choirs, playing a trombone in the band, and picking up the guitar. It should be no surprise that my wife, I love to hear her sing, and her voice has lasted much longer than mine has.
It all started with sitting by her as she waited to be picked up at high school. Of course, I had been trailing her for months, getting up the nerve. I was about to graduate, so I had to make my move. She left her [sheet] music there as we were sitting and visiting. When her dad drove up, she left the music, so I didn’t say a word. Of course, I knew where she lived. After her dad took her home, I followed about 20 minutes behind and handed her the music.
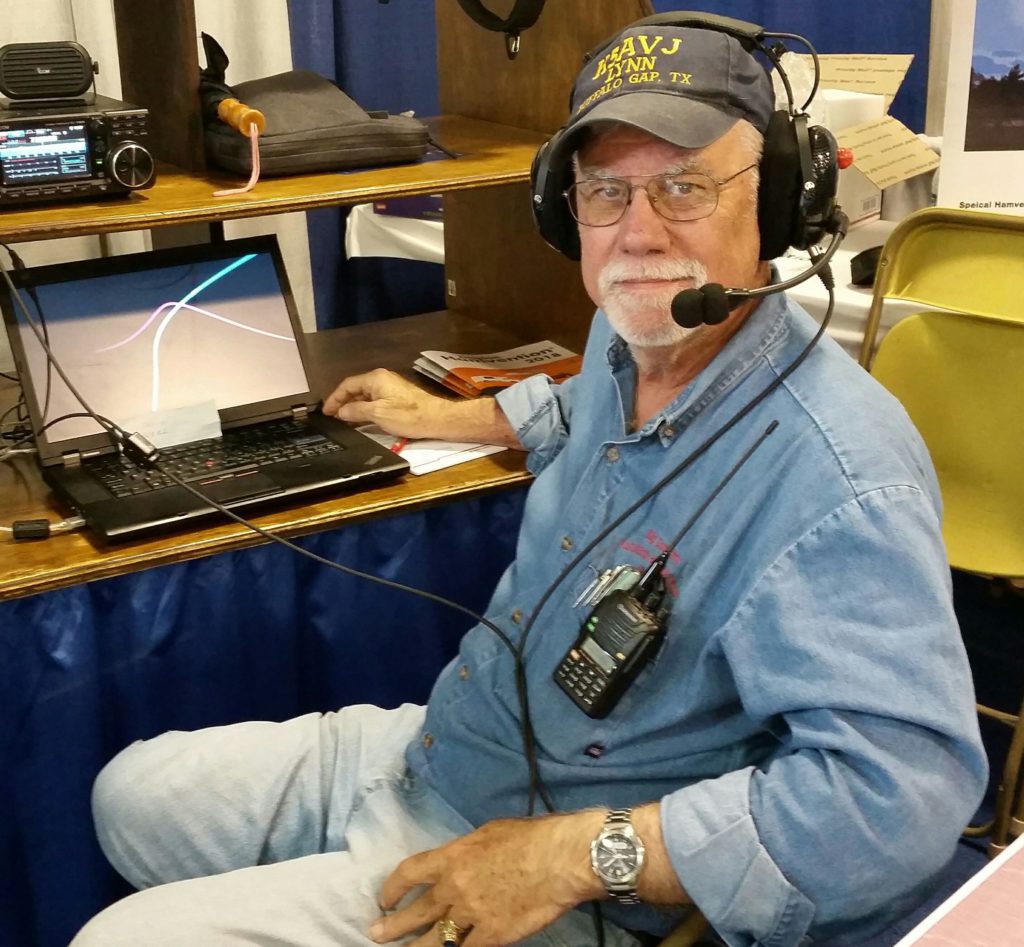
Ham radio
[One] morning I had insomnia about 2:00 a.m. I knew some guys were talking, and I went out into my ham shack and talked to them. First time I’d actually talked to them, but I told them I had been listening to them for 10 years.
I said, “When I was diagnosed with blood cancer, it meant a lot to me to be able to get some normalcy by listening to you guys in the middle of the night when I was lying awake worrying about my disease.”

That meant a lot to me to bring some normalcy into my life. You just longed for that. Your life has changed for forever when you’re diagnosed with cancer. That was my chance to say thank you to those guys that morning.
They said, “Hey, everybody out there, this is Lynn’s first time. Say hi to him.” I was hearing voices and people giving their call signs from different locations. I certainly did feel welcome. I had witnessed their companionship, the type of camaraderie. Anyway, the friendship that they have, their camaraderie.
My wife has put up with it, like they do with hobbies, whether your hobby is radio or fishing or whatever. She’s put up with it. I appreciate that. It’s not all time consuming, but it varies.
Cancer’s impact on who you are
When you’re diagnosed with cancer or you go through a hard time in your life, it can put you in a very dark place. My normal personality is a very optimistic-type person, but I got into a real dark place. It was hard to come out of.
I’ve shared with you that in ’74, our son was diagnosed with cancer, and I lost 20 pounds just within just a short time. People react differently to depression, but I did the same thing when I was diagnosed with cancer.
One of the side effects of this cancer is weight loss, but I think it was as much for me as having that diagnosis hanging over me and not knowing what it meant. That it might mean I have 2 to 3 months left to live or maybe a year or 2 or 3, hoping to be a granddaddy, things like that. It’s a tough time to deal with.

Symptoms and Tests
What were your 1st symptoms in 2013?
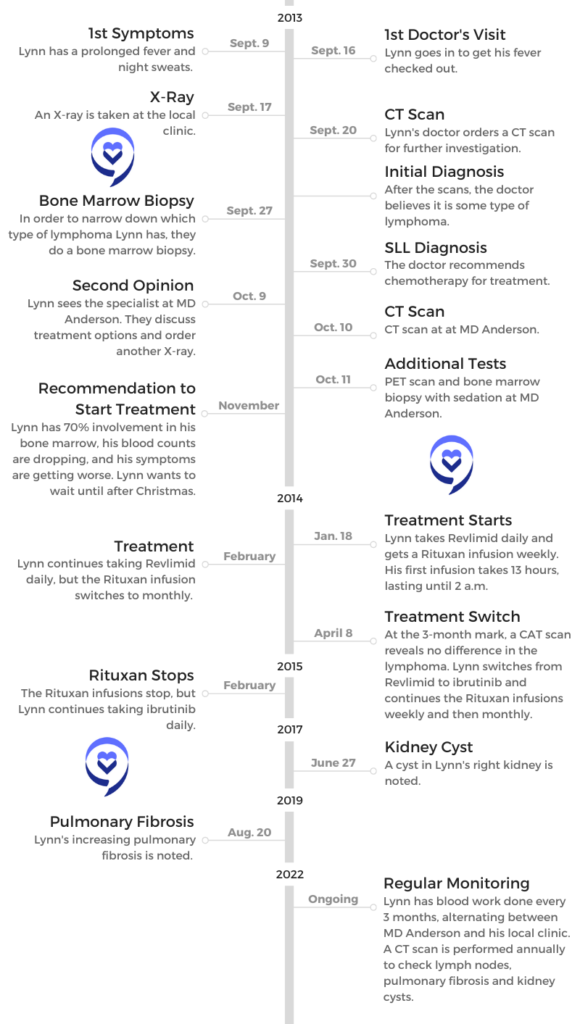
I began to run a fever with no known cause, which was not a new thing, but it prolonged. It lasted day after day after day. It went on for a week, and so I said, “Okay, I don’t know what it is, but I want to go see my primary care physician.”
I was having some night sweats along with that, too. I was meticulously keeping the record of the daily temperature. I actually saw the nurse practitioner, but he had a lot of experience and he said, “Let’s just get a chest X-ray and see where we go from there.”
Then the call came from the doctor’s office after they got the chest X-ray. They said, “He also now wants you to go get a CAT scan.” The alarm bells went off then. I said, “What did they see on the X-ray? Something’s going on here.”
Anyway, I went and got the PET scan. Then I had the appointment the next week with him to see what he saw. He said, “It appears that you may have a type of lymphoma. We don’t know, but you need to go see an oncologist.” That’s how things evolved at that point.
Night sweats
I had some night sweats with that. I didn’t know what to think about that. Is this just part of the fever or what? I would find that it would get much worse in the coming months. I found that it would be to the degree where your night clothes were drenched and the sheet underneath you was drenched.
I would sometimes have to get up and change clothes, underclothes and then the spot in the bed would be too wet to lie back down on. Through all that, I didn’t want to wake my wife up. We are in a pretty dry climate out here in West Texas, so things would dry out pretty quickly.
Getting an X-ray, CT scan and bone marrow biopsy
X-rays don’t raise an alarm. You’re just kind of like, “Oh, yeah, I’ve had a lot of X-rays.” But when they said, “We want a chest CAT scan.” Well, I’ve never had a chest CAT scan. Something is going on. I try to compartmentalize that, try to put it off to the side, but it’s there. It’s just nagging and you know something’s not right.
All of a sudden, what life I had left, which I thought was maybe 15 years, shrunk down to maybe just months.
The next week, I went in to get the report from the primary care physician. He said, “I think you’ve got lymphoma.” I went home and told my wife, and she didn’t believe me because I’m always joking and pulling pranks on her and things like that. She didn’t believe me when I went and told her. I had to insist that it was true.
She really stepped up to bat, because I withdrew into my cave. She began to research and print things out off the Internet, and I didn’t want to read them. Of course, I had the upcoming appointment with the oncologist and then the bone marrow biopsy.
When I got there, she said, “We can do a biopsy of your lymph nodes, but they’re all internal, so it’s going to be a little more difficult to get to them. We need to do a bone marrow biopsy and we can assess from that what type of cancer this is.”
The Diagnosis
Receiving the diagnosis
Then when the report came back on that, she said, “This is small lymphocytic lymphoma (SLL), which is akin to chronic lymphocytic leukemia, except this is primarily in the lymph nodes and not detectable at this stage in your blood. What I would recommend is that you be treated with R-CHOP.”
We remember the acronyms from when our son had cancer. We remember the acronyms and that they had meanings, and we recognized some of the drugs that she mentioned that I would be treated with.
I went home with the feeling that my days were numbered. Of course, I’ve always known my days were numbered, but I said, “They’re very short.” I went home with the thought, “I got to go through this.”
Within a day or so, my wife contacted the children, the grown adults, and told them what was going on. She came back and said, “The kids and I want you to go to MD Anderson.”
Processing the diagnosis
I crawled back into my cave and just accepted the fact that I was going to have to go through chemotherapy. My days were numbered. It was a dark place and just almost a resignation that this was the end.
My wife came, and still I had not read any literature. I had not looked on the Internet. I was scared of what I would see. My wife came, and she had printed some things out that I didn’t want to see. She said, “The kids want you to go to MD Anderson.”
With our history with our son having had cancer back in the ’70s, we were familiar with MD Anderson. We knew it was the right place to go. I knew it was the right place to go, but I just felt so lousy. It didn’t feel good, and I didn’t want to make the 400-mile trip.
She stepped up as the caregiver and called MD Anderson and made an appointment. She didn’t even get a referral. She just made an appointment and said, “I got you all lined up. We’re going to go down there, and we’re going to go there in a week-and-a-half.”

It’s one thing when somebody else gets a diagnosis, but when you personally get the diagnosis, in my life the future just disappeared. Even at that age of 66, the dreams I had of being a granddad and what was to come and things to enjoy since I was newly retired — those all vanished.
All of a sudden, what life I had left, which I thought was maybe 15 years, shrunk down to maybe just months. I didn’t know. I certainly knew I didn’t feel good, and something was wrong. The doctors were right. I did not feel well.
»MORE: Patients share how they processed a cancer diagnosis
Did you feel like you were losing things you had been looking forward to?
Yeah. We had retired where I was working in West Texas, out in the country on 6 acres. There was an extensive area to mow, but there were things we were involved in.
We were involved with our church, and we were joining with an acoustic group of musicians singing at the rest home. I was enjoying getting to take my guitar, and there were dulcimers, violins, other banjos and other kinds of instruments.

He said that we can’t cure this disease, but we can manage it. All of a sudden, the glass for me was half full again.
All of a sudden you’re sick, and you need to stay away from people. When I saw people, I was not one who held it back or didn’t share my diagnosis. I shared that with other people. All of a sudden, it’s like you’re marked, and I felt marked.
I felt like, “I’m here, and I just want to tell you that I’ve got this diagnosis of small lymphocytic lymphoma.” Of course, nobody knew what that was. It is a rare disease, just like its counterpart CLL. They’re rare diseases.
Can you describe what you meant by feeling “marked”?
We’ve all been through that in our life where somebody we knew was diagnosed with a terminal disease. You have different reactions. When you hear that, you don’t know how to respond to that person or to their family. Sometimes you’re asking their family members, “How are they doing?” because you’re uncomfortable asking that person how they’re doing.
We’ve seen through life experiences that some people withdraw from you. Some people that have been friends don’t know how to cope with it, so they pull back. I was pulling back, too. It was a difficult time.
Processing what it means to live with chronic cancer
I finally saw the specialist at MD Anderson, and the phrase that he said to me brought hope back in my life. He said that we can’t cure this disease, but we can manage it. All of a sudden, the glass for me was half full again. It was not half empty. I found that to bring hope to my life.
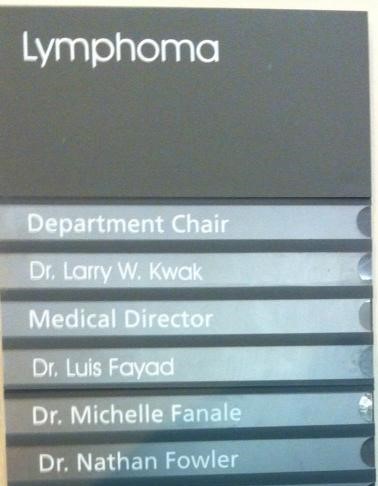
On that trip we made to MD Anderson, I decided to start looking for things that were humorous again and find things to laugh about. As I stood there in the medical clinic at MD Anderson and I looked at the list of doctors, I began to laugh. One of the doctor’s names was Dr. Fanale. He was not my doctor, but that was one of the doctors.
The doctor at the top of the list, the one in charge, was Dr. Kwak. I had to take a picture of that and post it on my Facebook page to let folks know that I was finding things to laugh about again.
We stopped and ate at a restaurant. Of course, camo or camouflage-type dress is common in Texas, and I looked over there and saw these folks with camouflage. It made me think of the TV show about the guys in Louisiana that sell the duck calls. I thought about them. Things like that were bringing humor back to my life.
Can you explain the power of your doctor saying you could manage the cancer?
I think I was thinking he was going to say, “We can just buy you some time.” But he turned it in a positive way to say that we can manage it.
I did not have any comprehension of the research that was going on that was going to begin to explode in the treatment of CLL and SLL, which certainly has exploded in the last 10 years. It would bring so much hope for people that are diagnosed with those diseases.



To that point, the treatment was going to be chemotherapy. But as we sat down and talked — the doctor and I did, and my wife and son were with me — he said, “Let me just talk to you about some of the treatment options. We’ve got the traditional chemotherapy that we can treat you with, or we can treat you with some novel therapies, targeted therapies.”
We began to see that there were some other options. We were up into the time frame of November, and he was ready to start treatment because I had 70% involvement in my bone marrow, and my blood counts were beginning to drop. The B symptoms, as they say, would be getting worse: losing weight, the fevers and the night sweats.
Treatment and Side Effects
Deciding to Start Treatment
Testing for treatment options
He gave the option to start treatment in December, and I said, “You said that this is a disease that we don’t have to treat right away? We can defer. How about if we start in January? I would like to enjoy Christmas.” That’s the way that took place. We went back to MD Anderson. At this point, we were going to MD Anderson every month.
Now I digress a little bit, but you go from where you’re comfortable, the doctors you’re comfortable with. Here you go to the big city, and you go to the parking garages, and you go to the freeways. All that, to me, was like a maze. As we age, we’re not as capable of negotiating those kind of traffic jams and problems you have.

It’s like a great sigh of relief came when you get the car parked and stop and take a picture of the parking lot number so that you remember where your car is when you get ready to come back to your car.
We were having CAT scans, and I had PET scans, bone marrow biopsies and blood work. I’m sure at some point in there I had an X-ray, and then at some point in there I’m sure I had an EKG. They wanted to be sure that the kind of drugs they were giving me would not interfere with that.

Discussing treatment options
There we were, going to start in January, and we discussed the options. It was chemotherapy or a novel therapy. The doctor said, “We’ve got 2 drugs that have had some benefit for this type of cancer. One of them is Revlimid. The other name for that is lenalidomide. It’s a common treatment for multiple myeloma. The other drug is Rituxan.”
Of course, those didn’t mean much to me. Some folks have a long watch and wait. During that time, they can research and see what the different drugs are and how they interact and so forth.
A pill a day keeps the cancer away.
I was so naive that the Rituxan went in on an IV, so I thought that meant I was actually getting chemo. I didn’t understand that it was a monoclonal antibody, and it was not chemo. I got Rituxan and Revlimid. I was getting the Rituxan IV every week, so we stayed there locally.
We were going back every week to get another infusion, and this stretched out for about a month. Then after that, we were coming monthly for the IV and to get a refill on my pills, which were the Revlimid.

Changing treatment
At the 3-month mark from the time we started, the doctor said it’s time to do a CAT scan and see if this is working. The results came back, and we sat down with him. That was in April of 2014, and he said, “Okay, what we’re seeing is no difference.”
I said, “Well, that’s good, isn’t it? I mean, they haven’t grown.” Here I am, the guy with a glass half full of water.
He said, “No, no, that means we need to try something else.” He said, “There’s a new drug that was just approved by the FDA, but it’s approved for second-line therapy.” I had failed Revlimid and Rituxan, so I was ready for second-line therapy.
We began with again repeating the Rituxan every week (and then stretching it to every month) and taking the ibrutinib every day. That’s how that all started in April of 2014.
»MORE: Read more about ibrutinib and other patient experiences
Over 8 years later, are you still on ibrutinib?
That’s right. I’m still taking my daily pill. As I say, a pill a day keeps the cancer away. In some ways, to me, it’s not too much different than the person who’s a diabetic and has to get insulin every day or some other type of chronic disease.
I choose to look at it in a positive way. I know that this may not work forever. I know it’s got some side effects, and we don’t know for sure what the long-term side effects are.
God bless those folks that were in clinical trials, because those pioneers that took this — some of them it worked for them, and for some of them it didn’t. For some of them it’s still working, and they’re at 10 years on this drug. They continue to bring me hope that this will continue to work for me.
In the meantime, I’m on the very first of the BTK inhibitors (ibrutinib), but since then, there have been several other ones that have been developed. There are second generation and third generation ones that have fewer side effects and are easier for people to take. It brings hope for other people.
Besides that, there are other types of treatment that are targeted or novel that are not chemo. They know now that chemo’s probably not the best treatment. Before ibrutinib, the standard of treatment was FCR. That still is the standard and probably is in some other countries. Fortunately, in the U.S., we’re able to move on to other options.
Side Effects
Balancing side effects and new treatments
Back in about 2015, I was taking ibrutinib, and I was at a Patient Power conference at MD Anderson. Dr. Michael Keating, who is one of the pioneers of treatment and drugs, was answering questions.
I asked the question, “Since a bone marrow transplant or stem cell transplant is the cure that we would have to lean on if everything else quits working, but at a certain point we get too old to take that, why don’t we just do that up front? Why don’t we get the stem cell transplant up front?”

He said, “Because these other drugs that you’re taking have so much fewer side effects, so much less risk. There’s a lot of risk with a stem cell transplant or bone marrow transplant.”
I was reading the blog of Dr. Brian Koffman, CLL Society, and what his journey was like and what was working for him. He was one of the pioneers of ibrutinib. There was another fellow, Terry, who had a blog going back to year 2000 about the different drugs that he was on even back then. To be able to read those real-life stories, just like you’re creating with these videos, gave me hope.

Being able to take treatment at home instead of going to a clinic
I started well for the first line. I had a pill and the infusion. I didn’t have to go in and get an infusion once we got the infusions behind us. Life was much more normal than it would be with every week or every month having to go in and get IVs. Of course, every time you had to go get an IV, you had to have a blood count to go with it to be sure that your counts were up high enough to proceed with that.
When I started on ibrutinib in April of 2014, I think even my doctor was cautious, too, because all he had to read was the clinical trials from a medical standpoint. But he didn’t know how long it was going to work. I was going back every month to get the infusion. I also was having blood work done.
Of course, that led us to that 3-month point when the CAT scans showed that wasn’t working. Even after we proceeded forward with ibrutinib, I was still getting a CAT scan every 3 months. With SLL, the disease was hidden in my body. There were no swollen lymph nodes on my neck to observe. It was lymph nodes that were internal, so the CAT scan gave an option to see what was going on.
They would look at the CAT scan and compare it to the previous one to see if anything was changing. Did the lymph nodes decrease in size? And once they had, were they staying at that point? Thankfully, I only have to get that CAT scan once a year now.

Side effects of treatment
If you’re on Facebook with a CLL group on there, you’ll see people talking about the side effects that they’re having. I had a lot of those. I had the achy joints. I had the sore muscles.
At one point, my knee hurt so bad I thought that I was going to have to have a knee transplant. I said, “Let’s hang in there. It’s probably just a side effect.” Any time I stood up or anything, it just hurt. I had that happen a couple of times, but thankfully, that pain would just vanish after about 3 days. Then the next day it was almost like a memory. If I didn’t remember it, I didn’t even know it had happened.
Then after some period of time, I began to notice my nails were splitting. I had to be careful when I was prying anything with my fingernails [so I didn’t] pull a nail loose or split a nail. Then I began to keep my nails much shorter and to file them if they got rough edges and things like that. That’s still an issue.
My hair was so straight and normal in my perspective, but it became frizzy and wild. My wife just finally said, “Just cut it all off.” That’s what we did. There’s some hair up there, but not a whole lot of it.
If I had it growing out, I would look like Albert Einstein. I would look like those pictures of him where he had the wild and crazy hair. That’s kind of how it evolved.
Having those side effects, you find yourself comparing with other people through the different forums and encouraging other people. For some folks, the side effects are so overwhelming they just can’t go on. They have to change to a different treatment.
The danger of low neutrophils
The first dangerous side effect that I had was picked up at the 3-month point. When I went in for blood work, my neutrophils were down, I think around 600 or so. The neutrophils are like the number one fighter in your immune system.
I’ve got a friend right now over in England that’s in the hospital. The neutrophils can get low enough that if you’re running a fever, you can become septic really quick. You have to be really careful.
Fortunately for me, the doctor said, “Okay, we’ve got something we’ll try with this. We’re going to give you a Neupogen injection.” Oh, boy, here’s another shot. As a cancer patient, you’ve been stuck every which way but loose.
I said, “Well, here’s another one.”
He said, “This one goes in your stomach. It’s just subcutaneous. It doesn’t go very deep, and it’s a little bitty needle, so just a little sting.”
It was easy enough that they gave me one there, and then my wife was able to give me the next 2. By then my neutrophils were beginning to climb back up, so fortunately I was able to rebound.
But some folks don’t. Some folks have a harder time with that, so some folks have to have infusions if their platelets or various blood components get too low. You just have to be careful when neutrophils get low. You have to be careful about being around people. You have to be careful about eating food that hadn’t been cooked.
That was just another one of the side effects that you have. Some folks have rashes. I have some rashes, but I don’t know if they’re caused by the SLL, if they’re caused by the treatment I’m on, or if they’re caused by something else.
Continuing to Monitor
Regular blood work
I realize that with the treatment I’m on, the cancer is not gone. I still have some of the side effects of the cancer. I still have night sweats every once in a while. They’re not really bad.
They looked at my blood at MD Anderson. They said that I have 1.6 cancer cells in a flow cytometry test. That’s like 1.6 in 10,000, so that means it’s still there. You take me off of the ibrutinib, and it’ll come back. You just keep on taking that pill a day.
I get blood work done twice a year at MD Anderson on a 6-month interval, but my doctor has asked that I also get intermediate blood work done at the 3-month and the 9-month marks. I do that through my local primary care physician.
Other issues to monitor
You did bring up the kidney cyst, and he referred me to a pulmonologist there, who reviewed the CAT scan and so forth. They said I could follow that locally, so I see a urologist once a year here and take them the CAT scan.
With the pulmonary issue, something new has come up in the last 4 years. They solved it back in 2013 on those early CAT scans from some issues in the lungs. I’m a non-smoker. As it moved forward, the pulmonologist told me that it’s idiopathic, which means they don’t know what caused it. Idiopathic pulmonary fibrosis.
Anyway, we just track that. I hope it doesn’t take me out eventually, but you just go with what you got. Of course, that’s one of those things I went back to the doctor at MD Anderson and said, “Is there anything in the side effects of this drug that would point to this being the cause of this?” That’s, I think, the question anybody would ask. I would look on the Internet and try to see if I could find anything in my layman’s understanding that would point to that.
I do that usually every year before or every 6 months before I go back to MD Anderson and see if there’s anything there that we need to talk about. I realize he’s got a plate full of patients besides me. You’ve got to ring your own bell when you’re there and bring up the questions you have.
Are your kidney cysts and pulmonary fibrosis related to your SLL?
No, it’s not. Apparently the kidney system is not that uncommon, according to the urologist. Even my cancer doctor said that any issues from that cyst will not bother me in my lifetime.
Of course, then if you look at that from a negative way, what does he mean by “my lifetime”? Does he know something I don’t know? There’s always a comment on that report every time I have it done. It’s happening in both areas.

Self-advocacy
Certainly, your doctor is the medical expert. You really need a doctor that can explain to you in your understanding what’s going on. There are things that concern us. If you and your doctor differ about the route you’re going to go in the treatment… For some folks, you change doctors.
I have not been to that point. I’m comfortable with my doctor. He’s probably in his late 60s now, so I know he’s got a lot of experience in treating different cancers. As a specialist, he treats more SLL patients than anybody else I might go to in the Southwest, so I trust his judgment.
Like you say, with new drugs, there are new side effects and issues you’re dealing with.
»MORE: How to be a self-advocate as a patient
Getting a second opinion
I’ll just backtrack here a little bit. We had the experience with our son that when you had a side effect or you had an issue, your local doctors would say something. When we got to MD Anderson to review what we had heard, we found out that they were the experts. They understood what was going on in a much better way than our local doctors. I believe that’s still true today, just by the fact that your doctor is a specialist.
Usually in those areas, some type of teaching facility like MD Anderson, they treat a much greater number of patients.


They can also question other doctors in their facility that are treating similar patients to see, “Are you seeing this?” In my case, a pulmonologist referred me to a pulmonologist there locally at MD Anderson that I could talk to about what was going on. She was used to dealing with cancer patients and the issues they had related to your lungs.
Being a Caregiver and Lessons Learned

Lynn’s Experience as a Caregiver
Seeing a specialist
We certainly became advocates for anybody that had cancer to go see a specialist. If there’s any hope, it’s going to be from a specialist. Not only because of their knowledge, but they’ll know what the latest treatments are. Often, a doctor in a remote area may not be up to date on what has evolved in the last 6 months or 12 months.
There are doctors that meet at these national and international conferences, and then they review the results of the clinical trials and what they’re seeing. From our perspective with our own son, we would definitely encourage anybody dealing with any kind of disease to go to where the specialists are.
At one point, my doctor at MD Anderson said, “You seem to be doing well. If you want to go back in the care of a local oncologist, you can.”
I said, “No, I want to stay with you.” We laughed about it later, but I said, “We’re not dealing with a common cold.” To be fair about it, it probably wouldn’t be a bad idea for me to have a local oncologist in a supporting role. [I would] still let the doctor in Indiana be the driving force. I think that’s probably a wise thing. I haven’t done it, but as you get older, it’s harder for you to travel distances.
As time has gone by, I’m aware of some other doctors. There’s a Dr. Awan over at the Southwest Medical Center in Dallas who is well thought of, so that would be an option for me. At MD Anderson, there are probably a half dozen or more doctors there that if my doctor decided to retire, they could just step in and pick up without skipping a beat.
Lynn’s son’s 1st symptoms
He was 3.5 years old, and we were with some friends at the swimming party. We noticed that his stomach was very swollen like a malnourished child. We said, “What is going on?”
We went to his pediatrician the following Monday. Of course, the doctor was very wise and an older doctor. He knew this was a bad thing. That went from there to him being in the hospital locally there, where we lived in Corpus Christi. He was there for a week. They were running various tests.
There were no CAT scans back then, so it was just blood work — maybe some type of a sonogram or something like that, but no CAT scans. Finally, the doctor, his pediatrician, told those doctors, “You’ve got to step up. This kid is getting worse and worse.”
The diagnosis
At that point, they did an exploratory surgery, opened up his abdomen and found a massive tumor in there. They took biopsies and so forth and then gave us the name of a local oncologist. We said, “We want to go to MD Anderson.”
When we finally got to MD Anderson, for some reason — we don’t know why — the biopsies were not usable. That’s why “undifferentiated” was the diagnosis. The doctor at MD Anderson said, “We hope this might be a Burkitt’s tumor,” which was that tumor found in children in Africa.
Anyway, it never was for sure what that was. He went through treatment and went through a relapse. We had him for 28 more years, and we were so blessed to have him for those 28 more years.
The cancer in the end did not come back. Actually, he passed away because of the damage of one of the drugs. He was like 3.5 years old. One of the drugs damaged his lungs and eventually his heart.

Advice of seeing specialists as a caregiver for any diagnosis
Even to this day, to somebody who has a child with some type of cancer, we would say go to MD Anderson if you can, or go to UT Southwestern. Go to one of the places where they have the experts. You can keep your doctor locally as a part of your team.
We went through this with my brother-in-law. He was diagnosed with pancreatic cancer, and we said, “We’ll take you. We’ll take you to MD Anderson if you’d like to go.” We did make several trips with him, and it’s a very difficult cancer to treat. He lasted 9 months. You got to try. You’ve got to look at all your options.
Emotional and mental impact of being a caregiver and then being the patient
When the cancer diagnosis comes, I think we all look at it from our own perspective. We look backwards at people we’ve known, and so often, people that we’ve lost, people that passed away from cancer.
I knew there was hope with some types of cancer. I knew that they were beginning to cure some types. When I heard that word, “lymphoma,” it was like the word “leukemia,” a very scary word.
So many other folks that get that diagnosis look at it all of a sudden as the person that has it, whereas before they were looking at other people that had it. They remember that experience, what happened, and what worked or didn’t work. It’s a tough time when that diagnosis comes for you.
Reflections
Looking on the bright side
Even with an SLL diagnosis, if the doctor were to say at my next visit in August, “Okay, you’re beginning to relapse. We’re going to have to start looking at other options,” I must say that that would be a disappointment. It would be a downer.
I think after kind of having a little pity party, I would begin to also to look at the bright side. There are other treatments that have a lot of promise. Newer drugs have been developed. There are drugs that are being given in combination that, for some folks, are at least getting them so deep in remission that the disease is not detectable, and it’s questionable whether it will ever come back.
Then there’s CAR T that Dr. Brian Koffman had, and Deborah Sims down in Australia had that as well. Both are doing very well. It’s not always a cure, not always even a remission, but still there are options. You take them as they come.
Benefit of watch and wait
One of the things I know a lot of people worry about with watch and wait is that the time is going by. But this particular disease (a chronic cancer or lymphoma), it just depends how you’re feeling at that time, what your blood counts are doing, and what other risk you have, because they often will watch and wait.
Each year that goes by means newer drugs are being developed and new clinical trials are progressing. That means if you’re not being treated today, but your treatment’s another year or 2, 3, 4 or 5 down the road, there may be new treatments or new combinations that were not even thought about when you were diagnosed.
Even for me, ibrutinib has bought me 8 years. There are other drugs that have come along and have been proven to be helpful, like venetoclax, that would be an option for me at that point.



Have you thought about getting to the point of undetectable minimal residual disease?
Yes. I have looked at the other options and have questioned the doctors about it. We’ve also even had a clinical trial nurse from MD Anderson join us on one of the CLL Society monthly calls and talked about the clinical trials that might be an option to add another drug to (in my case) ibrutinib.
One of the things that all of us eventually bring into this mix is our comorbidities. I mentioned that the issue of the pulmonary fibrosis makes it perhaps difficult to qualify for a clinical trial.

Another issue I have is I’m on a blood thinner because I’ve developed blood clots. Before I was diagnosed with cancer, I had 2 occasions where I had blood clots, and I found out that I’ve got a genetic issue with my blood that makes it more likely that this could happen. It’s not really common.
Anyway, those 2 things (the lungs and on a blood thinner) would make it more difficult for me to be approved for an additional drug. My doctor kind of took a risk, and I did, too, when he put me on ibrutinib back in 2014.
A lot of those patients would not be put on ibrutinib if they on a blood thinner because one of the side effects of ibrutinib is bleeding in the brain, subdural hematoma. I’ve told my wife, “If I fall and hit my head, no matter what I say, put me in the car and take me to the emergency room. I need to have a CAT scan.” Bleeding like that could certainly happen even if I wasn’t on ibrutinib.
What advice do you have for other people in your situation?
I would say certainly be open to go to a specialist, because it made the difference for me in getting the latest treatment that was available. If I had stayed here, the doctor was going to give me R-CHOP, which is not the right treatment at all. You won’t find that as a treatment.
My doctor at MD Anderson said that hasn’t been given for years. By being at MD Anderson, I was at the right place to begin on the drug of ibrutinib. Now they know that ibrutinib outperforms FCR, which was the long-time gold standard for this type of cancer. For some folks, it appears to have been a cure on the FCR. Anyway, I would say that it’s important to get to a specialist.
Things will get brighter.



Finding a community
I think the other thing I would say is, “Find yourself a community of other people dealing with cancer.” You can find groups on Facebook. I have a group that I joined, Blood Cancer Uncensored, on a weekly conference call. We’re friends that get together and talk for about an hour and a half when we can make it. It just warms my heart to be able to talk to people and to be concerned with others about the things they’re dealing with. We have not only CLL or SLL; we have other types of cancer.
Likewise, CLL Society, I join with a group out of the Dallas-Fort Worth area on a monthly basis. We talk about people and give an update on what’s going on with their cancer. If you want to talk, you can talk. I don’t want to really say anything. You can do that as well.
»MORE: Join other patients and caregivers on The Patient Story social media community
Helping find doctors
I’ve also joined with another group called AnCan, headed up Michele Nadeem-Baker. It’s a good group. It’s give and take, and lots of times folks will say, “Let me give you an Internet link that you might want to follow. There’s a study here that might be of interest to you.”
I like to try to help people find a doctor. It’s one thing to say, “I recommend a specialist.” Well, where would I find a specialist? You can go on the CLL Society website, and they’ve got a list of doctors there by the states that are specialists in this area. Likewise, [you can look for] whatever type of cancer you might be dealing with.
The specialists are going to be at the university teaching facilities. That’s also going to be the place where you can get research. The community doctor cannot put you on a clinical trial, because it’s not available through that location.
You’ll need to go to the specialist to see what trials might be available. I would encourage you to. You may have a pity party. Things may be dark. But I really think that when you get to talk to a specialist, things will get brighter
Inspired by Lynn's story?
Share your story, too!
More SLL & CLL Stories





Nadia K., Small Lymphocytic Lymphoma (SLL)
1st Symptoms: Rash, lump under arm, fatigue
Treatment: Ibrutinib and acalabrutinib

Tamsin W.
1st symptoms: Out of breath, dizzy, nauseated, tiredness, palpitations
Treatment: Obinutuzumab & venetoclax

Michele N.
1st Symptoms: Slow healing, scalp infection, enlarged lymph nodes
Treatment: Clinical trial of ibrutinib, fludarabine, chlorambucil and rituximab; acalabrutinib

Sean R.
1st symptoms: No apparent symptoms; went to ER for unrelated shoulder pain
Treatment: Clinical trial, Ibrutinib & Venetoclax


Tony D.
1st Symptoms: Lump in back of neck that got bigger in a couple weeks
Treatment: Targeted therapy - orall pill (Imbruvica), takes 3 pills a night