Terri’s Stage 3A Relapsed KRAS+ Non-Small Cell Lung Cancer Story
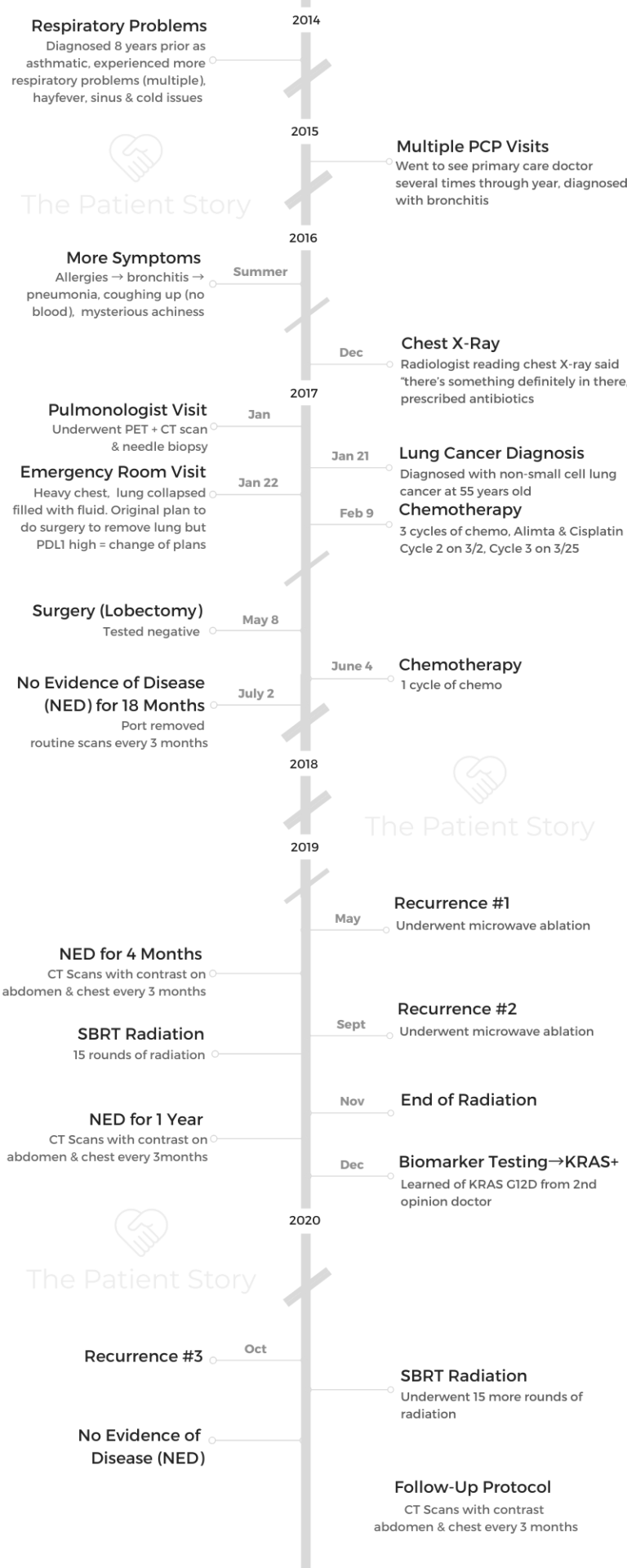
Terri shares her stage 3A KRAS+ lung cancer story, including experiencing 3 separate recurrences. She persevered through multiple treatments, including chemotherapy, surgery (lobectomy), and different radiation procedures, to getting to no evidence of disease!
She decided to take the feeling of helplessness and shift it into dedication to patient advocacy. Founder of nonprofit group “KRAS Kickers,” she also dives into what patients and caregivers should know, as well as how she navigated her own cancer experience. Terri touches on how she broke the news to loved ones, handled parenting with cancer, and the importance of connecting to a cancer community.

- Name: Terri Conneran
- Diagnosis (DX)
- Lung Cancer
- KRAS+
- Stage 3A
- Age at DX: 55 years old
- 1st Symptoms
- More trouble breathing
- Fluid in lungs
- 1st-Line Treatment
- Chemotherapy
- Alimta & cisplatin
- Surgery (lobectomy)
- Chemotherapy
- Chemotherapy
- 2nd-Line Treatment
- Microwave ablation
- 3rd-Line Treatment
- 15 rounds of SBRT radiation
- 4th-Line Treatment
- 15 rounds of SBRT radiation
- Terri's Story on Video
- First Symptoms & Tests
- Lung Cancer Diagnosis
- Treatment Decisions
- How did you decide where to go for treatment?
- Describe meeting your entire medical team
- Tip: Seek out a navigator or social worker for quality-of-life questions
- Guidance on how to navigate the overwhelm of appointments
- Did you get a second opinion?
- How did you break the news to loved ones?
- Any guidance on how to share the news with your children?
- Describe the treatment decision path
- Chemotherapy & Side Effects
- Surgery (Lobectomy)
- What was the plan with surgery?
- What was the staging?
- What are the questions you think are important that you wish you would have asked at the time?
- Describe the prep going into the surgery (lobectomy) and what you remember coming out of it
- Any guidance for others on recovery from surgery?
- What was the recovery like?
- How long was recovery at home?
- You did chemo after the lobectomy
- Describe the follow-up after hearing you had no evidence of disease
- It felt strange transitioning to fewer doctor’s appointments
- First Recurrence
- Second Recurrence & Radiation
- Third Recurrence
- Patient Advocacy
- Describe the shift from being a patient to patient advocate
- The importance of connecting with a cancer community
- What are the different lung cancer groups?
- What have you learned about KRAS?
- Exciting new treatment possibilities for KRAS+ lung cancer
- How important are clinical trials and patients taking part?
- Non-Small Cell Lung Cancer (NSCLC) Stories
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Terri’s Story on Video
How I Got Diagnosed
Chemo, Surgery, Radiation
What Patients Should Know
First Symptoms & Tests
Tell us about yourself outside of cancer
I live in Charlotte, North Carolina, and transplanted here from Arizona and from the Chicago suburbs. I have 3 kids that are all adults and an amazing husband. We play some games and like football. We like to just hang out and enjoy life.

What were the first symptoms?
The thing is that when you look back, historically, it makes a little bit more sense. When you’re going through it, you just think, “Oh, it’s an allergy. It’s like a cold.”
I’ve had asthma intermittently throughout my life. I went back and forth to the doctor several times, and she’s like, “You try doing over-the-counter stuff.” We changed up my asthma medication, and still, I was really struggling.
We spent quite a bit of time at the beach, and it just reached the point where the humidity just was oppressive. We went back again to the doctor. Like every other busy mom, you just push things off and push it off.
Finally, I went back to the doctor a couple of days before Christmas in 2016. By then, it had turned into full-blown pneumonia. She could hear the fluid in my lungs and treated me with antibiotics.
We did an X-ray at that point. Fortunately, from the X-ray, which is not a really good diagnostic for lung cancer, the fluid showed up. It highlighted the tumor that was in my lungs. We followed up with a considerable amount of testing.
When did you realize things were serious?
When they could see the fluid, it made more sense. We went back there and saw what she was talking about. You could very clearly see there was something inside the lung.
At that point, because cancer runs in my family, I was totally convinced it was probably cancer, but I was afraid to say those words.
My doctor said results would come right back in 10 days. That’s when we went back. When I wasn’t feeling better by the 1st, I knew for sure something was completely wonky. Then we saw the pulmonologist and went through a long diagnostic period.
I had no idea the difference between an X-ray or CT or a PET scan or any of that. You don’t find out until you need to know. It’s really important to understand that.
Describe the CT scans
Initially, I went back and had a CT scan, and it was just very simple. You just laid on the table, and the machine did all the work. There was no prep.
They could still see there was something going on. In order to prove to the insurance and all the other powers that be that we needed to extend testing past that, I had to do another CT scan, where they injected some dye into me,
It’s a couple of hours, and it’s simple stuff. Just lying there, the machine does all the work, nothing hard, nothing painful, very quick, very painless, except for the stress around waiting.
Describe the PET scan
The PET scan is a little bit more extensive. That’s where they do a whole-body scan, basically from the neck down. You have to do a certain amount of fasting, not eat sugar, and eat all high-protein items, because they inject a special sugar inside of your body to be able to find any sort of metabolic activity, which would be something that would be indicative of cancer.
The waiting around and having the test is very stressful.
Did you deal with scanxiety waiting for scan results?
The scanxiety doesn’t really hit until later. Now, doing follow-ups, and I’m 4 years down the road. Then you’re not even sure what you’re waiting for.
When you’re first diagnosed, I think that it was really a very stressful time for me, as it is for most people. You don’t know what’s coming; you don’t know what’s next.
You’re not really sure what you’re waiting for. Am I waiting to hear that there is something there or there’s something not there? What am I waiting to hear? What am I even hoping for? It’s not like you know the rules to this game.
It is stressful, and it is hard. How do you manage it? It’s like anything else. You’ve just got to do what you got to do. You want the right results, and you want to get the right information. The important thing is getting it done so you can see clearly what is there.

Describe the biopsy
It varies based on where the cancer is in your body. Mine was lung cancer, so that’s the part that they had to go into. Not all lung cancers are as easily accessible as mine was.
Relatively speaking, it wasn’t as bad. I thought of my lungs like balloons, and I was really concerned that they were going to pop, to be honest with you.
They don’t, because there’s fluid and there’s other things around it. It was a little bit of prep, and I couldn’t take certain things for several days. I went into the hospital, and it was just a several-hour procedure.
They stuck the needle in where they needed it to go. I got a little whacked out on the cocktail stuff they gave you, and that was it.
Was there any pain post-biopsy?
It wasn’t horribly painful. It was just a little bit tender, a little bit sore. It was relatively easy.
When did you get the biopsy results?
My doctor was able to call me back within 48 hours of the test to let me know the results of it. He offered to either give them to me on the phone or to have me for an office appointment. I’m not much for waiting. I already felt like I waited quite a bit.
Lung Cancer Diagnosis
Describe the moment you got the diagnosis
I was like, “Just give it to me. I want to know.” He told me that it was a non-small cell adenocarcinoma. That’s what I knew on a Friday.
Even if you suspect, even if you know, even if you believe, hearing somebody actually spell it out for you is still a moment that you just stop. It’s kind of that out-of-body moment, like being in a car accident or something.
You can remember that moment, that feeling. I don’t know what I was expecting to hear. I wasn’t surprised, but he was talking to me, and it was in some sort of weird dream.
You can just remember where you’re sitting and how you feel. At one point, I turned to my husband. I said, “Well, you weren’t there.” He’s like, “Yes, I was there.” Because I was so in my own head, all I could remember is just this one place, this one moment, this one thing right there.
It was intense. Not going to lie. It was intense. Now you hear it. Now you know.
Now what?
How did you process the lung cancer diagnosis
It’s really the closest I have ever been hit by a train, but that’s what I imagined it feels like. I’m looking at it this way, the train hits me out of here, and now what?
Definitely, you’re confused. Now it’s a legitimate diagnosis. It’s not all in my head. It’s not just a cold. It’s not whatever I did or didn’t do. I can’t fix this with kale or exercise. I have a diagnosis, and now what?
The next morning when I woke up, and I guess I was going into shock. You’re not really sure what is, and what’s not. It’s like you try and steady yourself.
I went downstairs first thing in the morning. It was just so heavy, and I couldn’t breathe. I’m thinking, “I must be having a heart attack. It must just be the stress of the whole event.”
I couldn’t get that anxiety to leave. In fact, it was more than anxiety. My husband, bless his heart, was like, “You have to go to a doctor.” I’m like, “I don’t want to go to the doctor. I’m going to just wait.” He’s like, “No, you really need to.” We negotiated back and forth, and I ended up back at the emergency room. I was not doing really well.
Describe the ER visit
My lungs had filled up from fluid, and I was essentially drowning. That’s why my chest was heavy and hurting. In my mind, it’s still a moment of shock, and so I’m convinced that it must be stress. It must just be the anxiety of it all, of being in the hospital.
Then they had to take some of the fluid out of my lungs, which is not an unusual situation with some sort of pneumonia. It isn’t a horribly painful procedure, but it is life saving.
We went through that over the course of the weekend because now I was a brand new diagnosed lung cancer patient, and those words still couldn’t fully come out. It just didn’t come flooding into my mind at that point. We went through and met a whole medical team at that point.
Treatment Decisions
How did you decide where to go for treatment?
Because of the way it happened with my lungs filling up and not doing well, I just went to the hospital that my pulmonologist and my normal PCP were at. It’s not a major research cancer.
They treat cancer patients. It’s what they consider a hybrid. It’s part of a bigger system. I just went there because that’s where I always go for my health care needs.
It wasn’t something researched. I had trouble breathing. I went to the hospital, and that’s where I was. That’s where I met the team and met the oncologist and what have you.
While I was there, they were just into the process of setting up tumor board for the upcoming week. I was the last slot to slide into the lung cancer tumor board, which they do only every other week. I was very fortunate from that standpoint.
All the doctors from all the different disciplines — the radiologist and oncologist and all the different portions of it — go through your case and look at all your factors, including your age, your health, how things are, where things look like, what they are, and what are the next steps. It’s not just a one-and-done event.
Describe meeting your entire medical team
The way my clinic does it is they bring you in as a separate appointment through the hospital setting, and all the doctors from the different disciplines come to you. You have one appointment, and they come to you.
On that same day, my family was able to meet the radiologist, the oncologist, and the nutritionist, which I can’t even remember — a host of all of them. I was also able to meet a nurse navigator to help me answer questions.
Tip: Seek out a navigator or social worker for quality-of-life questions
When you’re in to see the doctor, you want to ask the important doctor questions. You don’t want to feel like you’re wasting their time or your time, and you want to get more specific information.
At my hospital, there’s someone called a nurse navigator. Sometimes it’s under the social work. Sometimes it’s under some supportive care network. For others, it might be called community care.
They have different names, but all have the same meaning. The nurse navigator was able to point us into service areas, whether it was a support group that we needed, financial assistance if we were looking for it, understanding next tests.
She really was just a wealth of info.
It was like if I needed a mom to go to. Maybe it’s because my nurse navigator, Phyllis, was so amazing that I was just really fortunate, but I looked at her like a mom or the older sister whom I could lean into.
Maybe she personally hadn’t been through it, but she could point me in the right direction. That was really helpful. She really does an amazing job, because she could help you.
If somebody says, “Well, you need to come back in 3 months,” but your doctor says, “You need to come back in 3 weeks,” there’s a disconnect. She can then help you figure out how to get that straight and work behind the scenes in the administrative red tape that needs to be resolved.
Guidance on how to navigate the overwhelm of appointments
If you don’t understand, have them explain it to you. Yes, write it down. Bring other people with you. We had 4 people smashed in a little room. Each one of my kids was asking totally different questions, things that I never would’ve thought to ask.
At the same time, it wasn’t just that they got the information, but I had them to ask later because I wasn’t necessarily hearing everything I needed to hear at that moment. It was just a wealth of information, a wealth of knowledge, and you’re trying to take it all in.
Physically, you’re not on top of your game. It’s not like you went into this, and you’re all revved up, ready to go. You’re not feeling any good.
It really makes a difference to take the notes and ask the questions.
The more I look back at it, I wish I felt less threatened to ask the questions, because the doctors and the team want to explain it to you, but they don’t know what you do or don’t understand. You need to be willing to ask them.
Did you get a second opinion?
Looking back, I wish I did get a second opinion. At the time, it was, ‘You just have to do what you have to do.’
It’s like when you’re driving a car and you see, “Either I’m going to smash into a tree, or I’m going to run over the kid. I’m better off hitting the tree than I am the kid.” You’re just trying to manage what it is you’ve got going on. It’s just so much.
We didn’t have the benefit of amazing shows like this, where you can listen and get other ideas, because when do you get the questions? It’s 2 in the morning when you can’t sleep.
You don’t get the questions during the day, when you can call somebody at 2 in the afternoon. That’s why I talk about this, because I want people to understand I didn’t do it right.
I didn’t do as many wrong things as I could have done, and I was very, very fortunate. Learn from the experience, take that knowledge, and ask the questions. Understand the answers. If you don’t understand them, ask again.
How did you break the news to loved ones?
I don’t think there’s any way that you can easily tell your family any bad news, regardless of what it is. Telling them about cancer, telling them that I was sick — they saw that I was sick. They just still weren’t convinced it wasn’t totally pneumonia.
As the pneumonia turned into something a little bit more severe — when I was put into the hospital that weekend from being filled up with fluid in my lungs — there was no turning back.
They had to know, and they had to know then. Even at recurrence, it’s still utterly the hardest thing, and I have to tell them because there are just no easy words. There are no easy words.
»MORE: Breaking the news of a diagnosis to loved ones

Any guidance on how to share the news with your children?
No, I think you have to speak to the person. How my son is going to hear it, because he’s an engineer and he thinks that way, is completely different than my daughters.
One hears it more analytically, and the other hears it much more as a personal, emotional thing.
You have to speak to the person and the age. When there were other difficult conversations through their lives, how did they respond to it? Was it better in a group? Was it better individually?
As my kids have become older, I see that it’s better if I tell them all at one time, as much as I’m afraid that they’re going to turn on me, because it’s hard. That’s mostly because I don’t want one to know before the other one does.
»MORE: Parents describe how they handled cancer with their kids
Describe the treatment decision path
Initially, the plan was to do surgery and remove my whole left lung. It was called a pneumonectomy. In the meantime, my tumor samples were sent out for what I now know to be biomarker testing. They were looking for some genetic, genomic mutation marker to see what was going on inside of my body.
It took about 2 weeks to get the results back. It was 2 days before I was supposed to go in to have my lung removed, and the doctor reached out to me and said, “We’re not going to do that. Instead, you’re going to do chemo. We’ll see how you respond to chemo. From the chemo, we’ll probably just remove one lobe from your lung if you respond well to it.”
They show you a piece of paper, and something is circled on it. You don’t know what you’re hoping for. You’re hoping, “There’s something; there’s not something there. What does it all mean?”
In my particular case, they were talking about the PD-L1 level, which is indicative as to how you’re going to be responding to immunotherapy, which was just starting to come online at that point 4 years ago.
Based on that, they decided that I was going to do some chemo, so they calculated out the correct chemo cocktail for me. I did 3 rounds of chemo.
After the 3 rounds of chemo, I was responding well to it, and we were able to just remove one lobe of my lung. We removed the lower-left lobe of my lung.
Chemotherapy & Side Effects
Describe the preparation for chemotherapy
I went in and had a port put in, which they put up here. They didn’t let me pick where the port went.
I had mentally and emotionally prepared to have my whole lung removed and had gone through all the testing around it. They send you through breathing tests, where they put you in this soundproof booth thing, and then they have you breathing in and out of a tube.
I was mentally and emotionally prepared for that, so when they hit me with another direction, it was all over again. I didn’t know how to react. I didn’t know what to think.
I wasn’t quite sure if this was good. Was this bad? I don’t even know what it was. It’s very stressful. For anybody to tell you it’s not stressful and, “Well, don’t worry, it is what it is.”
No, it’s stressful, and waiting is hard.
You had a lot of mental reservations before chemotherapy
My mom had breast cancer and went through radiation in the 90s. She also went through chemo. She had a mastectomy. I was scared to death.
I was afraid it was going to hurt. I was afraid of what was going to happen. I didn’t want to lose my hair.
»MORE: Patients describe dealing with hair loss during cancer treatment
My youngest was about to graduate from college. I was really scared, and I did not need to be scared. I really shouldn’t have been scared. I wish I had reached out to somebody and asked.
I wish I had the guts to ask my nurse navigator. I wish I had reached out to somebody who had been through the lung cancer community. I wish I knew where to go to get that information.
Describe the chemotherapy regimen
I had Alimta, and I had cisplatin. Cisplatin is a type of drug. It’s platinum-based, and it’s old-school as far as chemo is concerned. It’s also known to cause some hearing problems, and so prior to going in for any sort of chemo, I had to go in and have a hearing test. Cisplatin will give you tinnitus, and you can actually get pseudomonas (infection) as a result of it.
My chemo lasted around 8 hours. I had to do blood tests for a couple of days beforehand to make sure everything, my liver and all these functions, were all right, and then I got jacked up on some version of steroids.
I had to take a certain course or certain medication leading up to it, and then they clean up the port and then infuse it.
The biggest fear I had was the infusion needle was going to hurt going in. I’m here to tell you it didn’t hurt. I sat around and watched TV. It was really quite comfortable. I wasn’t even cold. I didn’t even do chemo right. I wasn’t even cold like in the movies.
Where did you get the chemo infusions?
It was a clinic just specific for chemo and infusions. They didn’t do just chemo infusions, but also blood transfusions. It wasn’t just cancer patients.
Describe the chemo side effects
I kept gaining weight. I was hot. My hair didn’t fall out. It got thinner, and I kept gaining weight. It was about 3 weeks between each cycle, and so I would go in on a Thursday. Then 3 weeks later, I’d do it again.
I didn’t feel lousy at first. Day 3 or day 4 is when I really felt miserable. From the movies, I was completely convinced I was going to be throwing up. I wasn’t throwing up.
I didn’t feel on top of my game, I’m not going to lie. It really wasn’t like in the movies, and it wasn’t like it hurt going in. I was really, really afraid it was going to.
When you feel lousy like that, and then every time you go, going and doing it again, it gets a little hard. You know what to expect; you know what’s going to happen. You come home, and you think you’re fresh.

This picture was after chemo cycle number 2. Do I even look sick? This is not my Julia Roberts moment from the movies, where she’s throwing up over the toilet.
This is a couple of hours after the second chemo I had. My daughter had just gotten a puppy and brought it over for us to take a look at. I was all jacked up on steroids, and so I didn’t feel that horrible.
What helped with the side effects?
The funny thing is that all those things that your mama always told you to do like try and sleep well, drink lots of water, and exercise — those things are really important to try and do during chemotherapy.
Even though you may not be running a marathon, you can drink water and stay hydrated. You can try and move around a little bit, because it does help your body to feel better.
How did you respond to the chemotherapy?
I responded very well to the chemo. Their idea of very well doesn’t mean that I felt like running a marathon, but it does mean that it was going to kill the cancer. That was good, but the cancer wasn’t completely gone.
Surgery (Lobectomy)
What was the plan with surgery?
We found that I was responsive after doing a scan. Based on that, we went in and just did just the lobectomy. My youngest one graduated from college, so we delayed things a little bit so that I could attend her graduation.
I had the surgery done in May of 2017. I was in the hospital for around 10 days.
What was the staging?
Initially, when I had that fluid in the lungs, the doctors were very concerned that it might be stage 4. They were presuming that it was going to be stage 4 until all the tests came back with the biomarker and reading the fluid.
The results came back, and it wasn’t metastatic. That’s when they determined that it was stage 3.
What are the questions you think are important that you wish you would have asked at the time?
I wish I had actually asked for the full biomarker testing to see what their report was and ask questions about it. Cancer runs in my family, but I had done genetic testing. I didn’t understand this was different testing.
This is testing that is based on the genomics, the mutations within the actual pathology of your cancer. It’s not necessarily germline what you get from your parents, from your DNA. That’s not what they’re looking for. I wish I had that.
I was very fortunate. I ended up with a great system and a great doctor, but I do wish I had thought like a researcher, somebody who was specific to lung cancer, specific to that particular area, because there’ve been so many advances in lung cancer.
In particular, the last 5 years, it has changed so much and so dramatically that a lot of doctors are not current on the treatments at all.
I really wish I could have done that sooner. Even if we stuck with the same program of attack, I do think it would have given me more confidence that things were going to be going on better.
The first thing I wish I would have done is to not have been afraid to ask the questions.
If I didn’t understand, pursue it a little bit more. If that means getting involved with somebody, like maybe do phone buddy stuff, or with one of the big organizations, or reading and watching these shows, that’s really what it takes to get that information.
Describe the prep going into the surgery (lobectomy) and what you remember coming out of it
We hadn’t really talked too much about what we were going to do after I did the lobectomy. We met with the doctor and with my medical team. I went into it really excited because it really felt like I was doing something.
I was physically removing this cancer from my body.
It just really felt like it was the first time I had any power over it, as opposed to just picking stuff in my body unaware and afraid that it wasn’t going to work, not knowing what was going on inside of my body, except from these scans. It really gave me much more power.
As far as the prep going into the lobectomy, honestly, I kept thinking it’s the waiting that’s just brutal. You get yourself so jacked up in your head, like, “What’s going to happen? What might really fix this? What about this? What about that? Do I have my will done? Do I need my will done?”
These are all really important issues. These are probably things that we should have taken care of way before I got sick. This is just something we should normally take care of as an adult, but you don’t really think about until you get a really serious diagnosis.

Any guidance for others on recovery from surgery?
They have different approaches to how you handle a lobectomy now. Now it’s getting a little bit more common to be able to do what they call wedge resection, or just go in and just take out a piece of it or a portion of it.
In my particular case, they had to go in and cut me in a V across my shoulder blade. They could go in, and I could get victory over that cancer. They went in, they cut that out, and then they took out the cancer.
I was in the hospital for around 10 days. I woke up, and I wasn’t mentally prepared for the juice coming out of me. They didn’t really hurt, but I was surprised. It just didn’t cross my mind to ask the question, “What am I going to wake up with?” I just didn’t know. I knew I’d be in the hospital for around a week.
What was the recovery like?
Lying in a hospital, eating their food, watching their television. The only time that they have anything for you is in the middle of the night when you’re trying to get some sleep. Every other hospital is just like that.
How long was recovery at home?
All the wonderful people that I have in my life — my Bible study ladies, my friends, my family, the neighbors, and people in my house that I work with — also were very helpful.
The insurance company was reaching out to me, and somehow it really became overwhelming. It felt like I needed a secretary to take care of all of it.
It reached a point where I had to say, “Thank you,” and then just not respond so then I could recover. Otherwise, it felt like I just kept saying the same thing over and over and over again.
That is something to be warned about. As much as they love you, take your space so that you can recover. I was just lying on the couch, or I was lying in bed. I was at home, and I was recovering and watching TV. Zoning in and zoning out is what you do when you’re not feeling that great.

You feel bad. As far as things I had to do, I had this little breathing apparatus, a spirometer or something. You had to blow this little ball in there, fill up your lungs.
At first, it was uncomfortable, but the more that I did it, it felt like I needed it. It felt like a good burn, a good exercise, like when you get the good stretch. It really felt like it was starting to really stretch well. That was helpful.
I just wanted to start moving around. It wasn’t exercising. This was just moving. Some days it was a big, exciting day because I took a shower.
You’re not feeling fabulous, but at the same time, you need to be able to move around. Just do a little bit at a time, and do a little bit more than the next day. If you’re not feeling so great, bring it down a notch.
You did chemo after the lobectomy
I was more worn down from the lobectomy, and then I did the chemo. That was a little bit harder than it had been previously. I did a scan following that, and the results came out well.
I had done so well that they decided that we could take the port out. I could physically go in and actually did it over the 4th of July weekend because I felt it was literally independence.
When they said I could get it out, I was like, “Let’s just do this now.” I didn’t want them to change their mind. Let’s get the port out and just make this go away.
Describe the follow-up after hearing you had no evidence of disease
I’m getting scanned every 3 months and talking to my doctor regularly. When you’re going through it initially, it seems you’re at the doctor’s 3 or 4 times a week.
Sometimes you’re getting 2 doctors in one day just because of the schedule and getting a hearing test every time before you get the chemo and all this stuff.
When you get back to the point where it’s like, “Okay, we’ll see you in three months.” It’s like, “Well, wait a minute, I’ve been here all this time. What am I going to do with my schedule now?”
It felt strange transitioning to fewer doctor’s appointments
It was a little sense of abandonment, because it’s like, “What do you mean?” They’re like, “Yes, okay, we’ll see you in 3 months.”
That’s the time you have to start being more intentional and start taking little pieces of your life back, as far as whatever your exercise program looks like, whatever your normal life looks like.
First Recurrence
First recurrence after 18 months of no evidence of disease (NED)
We just went in for my scans like a good patient. Every 3 months, I went in for my scan, a CT scan where they do a contrast.
It’s similar to what they did for the diagnostic, where they have an IV pushed in, and you have to drink this stuff to make sure everything’s okay in your abdomen. I’m still doing it every 3 months.
From one of my regular scans, that’s when we saw that there was something. My doctor called to let me know that there was something.
Nobody wants to hear ‘recurrence.’ Nobody wants to think about it, because I wanted to be done. This was it. I was done.
I was ready to move on with my life. Every part of me wanted to just shut the door and just move forward. That’s not what was in the plan, I guess.
How did you process the first recurrence?
The first recurrence, in some ways, I felt I let my family down. I felt it was really hard to tell everybody because I felt like I did something wrong. That’s one of the things that goes on behind scenes, at the time in the heart.
I want to be a good patient, and good patients do this. I’ve watched the movie. They get into remission, and so I wanted to do that. I didn’t.
How do you tell them, and how do you tell them right? Let me know when you figure it out, because it’s just hard to do.
Describe the microwave ablation
I had never heard it before. When I have this recurrence, my doctor tells me about it. I’m like, “Okay, what’s the plan?”
Now, I’m 2 years into the journey, so I have a lot more knowledge. I’ve reached out, I’ve connected with people, and I have a little bit of a better handle on what’s going on. She was saying, “Well, I think what we may have to do is radiation.”
The radiologist took a look at it and said that they would have an interventional radiology. There’s a specialty in it, being able to do what they call an ablation.
This is my non-science explanation, but the way I understand it is they stick a little probe inside of you. I picture a really skinny little soldering iron, and they burn this out of you. They don’t burn it like thousands of degrees; it’s only 110 degrees because your body’s only 98. They burn it down, and sometimes they freeze it out.
I was quasi-awake in their cocktail-y state in the CT scan so that they could see exactly where it was. I might have to hold my breath or move this way or that way. They went in, and they were able to ablate it and burn it all out.
We blew that up and got rid of that. After, they took a couple of samples of it so they could send it away for another biomarker testing.
Dealing with changes in the cancer
That’s what’s really important. Sometimes this cancer changes. Every time we have the opportunity to go in and see what it is, we mostly likely see what it is.
Most of the time, the insurance should cover it. If they don’t cover it, you generally can reach out to one of the lung cancer organizations, and they can help you figure out a way that it can become covered.
Were there side effects from the microwave ablation?
I’ve had worse PMS cramps through the years. I was lousy for about a day or 2, but I even went to church the next day. They watched me in the hospital overnight just as a safety precaution.
Then that was it. I was fine. I continued doing the scans every 3 months. I don’t even know if it was 3 to 5 months later, but I had another recurrence.
Second Recurrence & Radiation
Describe how you processed news of a second recurrence
It becomes just such a blur because I didn’t feel like I had recovered from the last one, and it was back at it again. Honestly, for me, I just feel like I was a disappointment.
I’ve always been a good student. I’ve always been a good patient. I do what I’m supposed to do. I tried to stop doing stupid things. I was disappointed in myself again, but it’s like, “Okay, well, we’ve got what we got. We’ve got to move forward with it.”
You can’t fix it if you don’t know it’s there. First find it. Now let’s do something about it. I know what it’s like to go through the other end of it, and I know how hard it can be later on.
I’m better off staying in front of it and just moving forward with it. Based on the scans and based on the information, they determined that the best approach was to do radiation, so I did 15 rounds of radiation.
Describe the SBRT radiation
I’m still picturing what the radiation is that my mom went through. This was not my mom’s radiation from the 90s. I wasn’t all burnt up; I wasn’t all fried. This was not like that at all.
It wasn’t bad like that at all. I laid down on the radiation table and laid still, which is not something I do very well.
I had to lie down for an extended period of time. As they’re marking me, they’re taking scans of me to see exactly where it is that they need to line up their radiation equipment so that they can hit it. That took like a good hour.
It was not easy to sit still, not easy at all. Then, when I actually went in for the radiation a couple of weeks later, they go back. They do their mathematical calculations, which I guess they have a whole department of people to do.
They have a pay grade way above mine. They go in and they determine exactly what they need to do. You lie back in the same place again. It was SBRT, and it was super short.
I drove up there, I laid down on the table, I was in there for maybe 5 minutes, and then I was gone. I was out the door. As long as I wore a yoga top or sports bra and stuff, it was no big deal.

Any more tips on what to wear to SBRT radiation?
Honestly, stay away from anything metal. Stay away from your underwires. It’s stuff like that. If I was wearing yoga pants and a yoga top with nothing metal, nothing on it at all, most of the time — I don’t say always, but most of the time — I can keep my clothes on.
Describe the radiation schedule
It was 3 times a week for 5 weeks, which would destroy my whole afternoon. I would come home because it is still 30, 45 minutes to get up there.
You park, you get in, you’ve got to check in, and you do your thing. The actual part of the radiation is super fast. [It’s] way longer to drive up there, park, get in, check in, all that, and then come back out and drive back home. Then you’re trying to work it so that you’re not driving in rush hour traffic and all that, and so it’s great. It’s always like that.
Most times, I didn’t have to wait very long, just a couple of minutes. I just had those yoga tops on and stuff like that. I pretty much would just go in there and just lie on the table. I’d probably be in and out in 10 minutes at the absolute. It’s really, really fast.
Were there SBRT radiation side effects?
It would feel icky as it wore on. It depends on where it is within your body to determine if you may have some bowel problems or stomach problems.
I didn’t really have any particular problems. I’d just come home some days a little bit more tired — not fatigued like it was during chemo, but worn out. You feel like you’re stuck. I just really got used to having a life, and then with recurrences, they take your life away.
Third Recurrence
You were NED for a year before you learned about the third recurrence
I had a recurrence, and we had to go through the same sort of thing. It had been around a year, and I had to go through another 15 rounds of radiation.
Just went through that and just fit into my normal life. Other than the inconvenience of the scheduling and whatever, I knew what to expect. I knew how to negotiate it through my calendar in my life.
Guidance for people who are dealing with recurrences themselves
It’s like anything else. You do what you’ve got to do. I’ve just taken that attitude whenever I go in. That’s where this scanxiety hits.
The scanxiety is this anxiety that surrounds the scan that you’re going to go in, and you’re going to have a recurrence. I used to get my scans every 3 months, and I try to keep myself really, really busy. Really busy so that I can sleep really well.
I get a little snippier than usual, but I might indulge in a little bit more chocolate or some of the other things I normally would not be so inclined to do, because I just tend to need a little bit of extra TLC. I keep telling myself that if it’s there. It’s there. I’m just going to know it is.
That’s the whole thing about lung cancer or about any cancer. It’s growing and it’s feeding inside of you, and you don’t know it’s happening. This gives me the upper hand. I have to take it and look at it as an empowering moment and keep telling myself that. It’s hard, but you do what you have to do.
How do you manage your cancer as a chronic disease?
I will be doing it because there’s a reason that we don’t really call it remission. We don’t call it cured. We’re told no evidence of disease. Even as though we’re looking at, again, I know people that have been doing this for 15 years or more, and they’re still getting scanned.
They may not be getting scanned every 3 months. It may only be one time a year, but they’re still doing it. At one point, I’ll go from 3 months to 6 months. Then from 6 months, it’ll probably go to about 9, and then from 9 months to about a year.
I think with a cancer diagnosis, it’s like anything else that happens in your life. The diagnosis isn’t going to go away. You’re just always going to have it. You always just need to be very vigilant about taking care of it and being intentional about getting scanned.

Patient Advocacy
Describe the shift from being a patient to patient advocate
You get what you get, but you’ve got to do something with it. I’ve just always been brought up with the mindset that you need to change what you can change and accept what you can’t.
When I had the lung cancer diagnosis, I had to deal with what I had. I went through the diagnosis, I went through the treatment, and I did the things that I needed to do. You feel so vulnerable, so helpless, and really confused.
As I learned more and found and connected within the different groups, I found out that there’s more people out there who have information, and they’re willing to share it.
I wanted to be one of those people who could help out and help reach that hand out to others. As I became involved, the first thing I did was I joined a lung cancer support group in our local community. We also have national groups around the country.
They’re not selling products. It’s just patients getting together, hanging out, and talking. Talking about what it’s like to be a patient and talking about doctors and stuff. I’ve really enjoyed it.
The importance of connecting with a cancer community
I’ve really enjoyed being able to connect with the other people and sharing what they had to say. Being able to just share and process what I had been through, too.
Being able to connect out with people, we just got in a little bit more engaged. I ventured out into Lungevity and the GO2 Foundation and connected with those folks to be able to give back and do phone buddies for people who were just newly diagnosed.
The lung cancer community breaks up into different biomarker groups around whatever the type of lung cancer that you have, mainly because we have different treatments that work for different people.
What are the different lung cancer groups?
Within the particular lung cancer groups, there’s EGFR, ALK, ROS1. It’s different groups. I wanted to find my group, but I didn’t know what my biomarker was. I didn’t know what was causing it.
I kept asking my doctor. My doctor didn’t give me the information that I needed so that I could understand. Finally, when I went out for a second opinion, I said to the doctor, “What is my biomarker?”
The doctor said, “You have a KRAS, and you have a certain subtype of a KRAS.” I was shocked, but I had something and immediately went home, looking for the KRAS people to be able to connect who have this particular type of mutation.
There wasn’t any group of people that had it. There was a group of people that had it, but I didn’t have one area of connection, so I started the KRAS Kickers.
What have you learned about KRAS?
What I’ve learned is that KRAS’s mutation is the most common cause in lung cancer. It’s also the most common mutation in pancreatic and colorectal.
Within the KRAS Kickers, we do have other patients that are from colorectal and pancreatic. Because I’m from the lung community, I’m most familiar with that. The largest group of people in the group has lung cancer.

Exciting new treatment possibilities for KRAS+ lung cancer
3 years into my diagnosis, I found out that I have KRAS, and it’s K-R-A-S. KRAS was one of the very first mutations that they found that caused cancer, and it was 40 years ago.
The researchers had been trying to find some sort of a treatment, but they were unable to find a way to be able to specifically target that mutation. They had termed it “undruggable.”
Just recently, they have found out that there’s a way that it could be drugged. We’re going to be able to take a target, and we’re going to be able to do something along the lines of possibly taking just a pill.
It’s just different subtypes within it, but it’s like any path, right? You have to make the first couple of steps before you get further down.
But after 40 years, for the first time, they’ve actually made progress. They’re going to be able to do something. I’m having a hard time sitting still.
I’m jumping out of my seat because it is so exciting. You’ve got to understand. 40 years, right? 40 years of not having anything and not being able to do anything, and now there’s a possibility of being able to do it and being able to literally kick cancer’s KRAS.
We’re the KRAS Kickers, and that’s what we do. We help connect the patients with the most current information that there is around KRAS. The KRAS Kickers are that sweet spot in the Oreo that brings those 2 areas together.
We support each other and help connect each other with the information, with the current treatment, and with the support. We’re all going through different things. It’s different for every person. If you learn my story, it’s my story. Your story will be yours.




How important are clinical trials and patients taking part?
I’m here today because of research. My mom’s not here today because there wasn’t the research that we needed today. What we’re going to be here tomorrow is a result of what it is we learn today.
I went into this space not knowing what’s involved or what’s engaged in any sort of a clinical trial or research. It’s scary and confusing.
Now that I’ve actually learned about it, I have learned that you’re really treated well, but you’re treated to either standard of care or the experimental drugs.
The experimental drugs have been experimented on the little critters in the labs for years before they get it to you, and they are confident that this is going to be okay for you.
You are saving somebody’s life tomorrow by working on it today. It really is just where the heart of it is, and that’s really what gives me hope. I know that there’s not going to be hope for anybody tomorrow unless we start doing more today.

Inspired by Terri's story?
Share your story, too!
Non-Small Cell Lung Cancer (NSCLC) Stories

Michelle W., Non-Small Cell Lung Cancer, EGFR+, Stage 2B
Symptoms: None; discovered by chance during a check-up for persistent head and neck pain
Treatments: Surgery (lung resection), chemotherapy (upcoming), targeted therapy (upcoming)
Kelsey D., Non-Small Cell Lung Cancer, EGFR+, ALK+, Stage 4 (Metastatic)
Symptoms: Severe back pain, falling due to collapsed spinal vertebrae
Treatments: Radiation therapy, targeted therapy (tyrosine kinase inhibitor, osimertinib), surgery (spinal fusion surgery), chemotherapy (through a clinical trial)

Megan F., Non-Small Cell Lung Cancer, ALK+, Stage 4 (Metastatic)
Symptoms: Chest pain, anxiety, shortness of breath, arm pain and swelling, back pain
Treatment: Targeted therapy (lorlatinib)

Roxanne C., Non-Small Cell Lung Cancer (NSCLC), Stage 3
Symptoms: None; incidental finding
Treatments: Surgery (lobectomy), chemotherapy (cisplatin), radiation therapy, targeted therapy (tyrosine kinase inhibitor/TKI)

Natalie B., Non-Small Cell Lung Cancer, Stage 4 (Metastatic)
Symptoms: Extreme fatigue, severe cough
Treatments: Chemotherapy, immunotherapy, clinical trials, radiation therapy, surgery (double lung transplant)
2 replies on “Terri’s Stage 3A Relapsed KRAS+ Non-Small Cell Lung Cancer Story”
Recent stage 4 Lung Cancer diagnosis. Found this site informative. Start Chemo next week.
Was just diagnosed with Stage 3 Non small cell adenocarcinoma with KRAS mutation.. Surgery is scheduled since no mets so far but it is a large 7 cm tumor. Would love to be a part of this group.