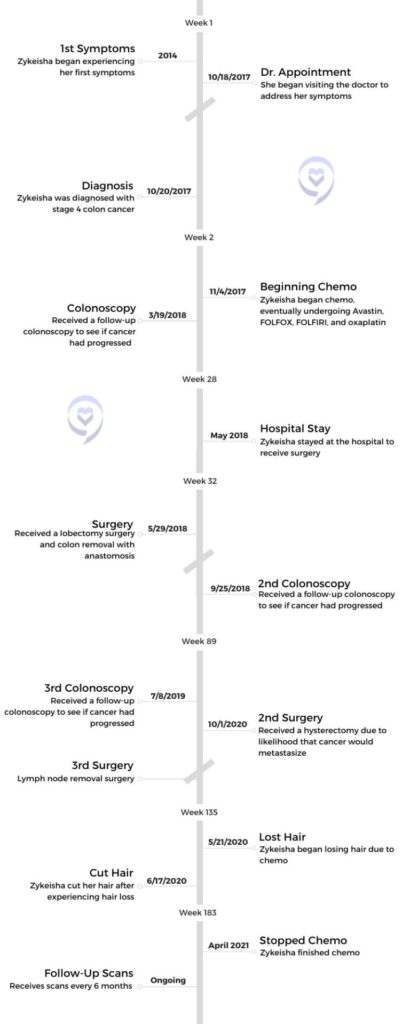
Zykeisha, a 37-year-old mother and fire rescue dispatcher, faced a difficult battle with stage 4 colon cancer. Her journey was marked by initial misdiagnoses and persistent symptoms like anemia and unexplained back pain which arose around the time of her pregnancy. Despite enduring grueling treatments including 12 rounds of chemotherapy, liver surgery, and a subsequent cancer relapse, Zykeisha’s faith and resilience moved her forward. She became a beacon of hope, advocating for herself with determination to overcome each setback.
Through her journey, Zykeisha emphasizes the importance of self-advocacy, urging fellow cancer patients to ask questions, explore treatment options, and prioritize their mental and emotional well-being. With her infectious smile and steadfast faith guiding her, Zykeisha’s story serves as a testament to the power of resilience and inner strength in the face of adversity.
Name: Zykeisha L.
Diagnosis (DX):
Colon Cancer
Staging:
Stage 4
Symptoms:
Anemia
Stool changes
Blood in urine
Sharp back pain
Treatment:
Surgery
Chemotherapy
Avastin
FOLFOX
FOLFIRI
Neupogen shots
Whatever gives you peace while going through something like this, find that and protect that.
Zykeisha L.
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
My name is Zykeisha. I am 37 years old. I am a mother of two beautiful, active boys. They are seven years apart. One is 13 years old and 7 years old. I am a fire rescue dispatcher by occupation. Hobbies: I love traveling. I love reading. I’d rather read a good book than watch a movie. I love to laugh, like anybody. I’m always smiling, that’s how I’ve always been. No matter what, I’m going to smile when I find a reason.
What were your initial symptoms?
I started experiencing symptoms in, I want to say, 2014 or 2013. I did not know initially that they were symptoms. I started having issues with anemia, so I had applied for insurance that they were telling people to go get – the cancer insurance. The insurance company actually dropped me, but kept my then husband and my youngest son. I received a letter in the mail that said I was dropped, and I was like, he has more health conditions than me. How was I dropped? I did not know that anemia is one of the things that insurance companies look for as a sign of cancer.
We had to do a physical for my job and I did my physical. The physician called my mom and said, “Your daughter needs to go to the hospital. Her hemoglobin is super low. She could pass out.” I didn’t think much about it. I went later on that night because I had a migraine.
I did not know that anemia is one of the things that insurance companies look for as a sign of cancer.
The doctor actually did a very uncomfortable stool test right then and there in the room. Beyond uncomfortable. They were checking me to see why my hemoglobin was super low. It was not because of a cycle. It was not because of anything. Nothing else was said or done about that. I was given a blood transfusion and nothing else. I was told to go on bed rest for two weeks after the blood transfusion.
More health problems arose during pregnancy
When I got pregnant with my youngest son, I did the regular tests that they have you do at 6 months, such as the glucose test. They called me and said, “Your hemoglobin is really low, you need to see a hematologist. I said, “Okay.” I called and said, “My hemoglobin is at a 6 and I’m 6 months pregnant. They said, “You’re not coming here, honey. You want to go to the hospital.”
I went, I was admitted, and they said, “Something is taking your blood, but we don’t know what it is and we can’t do extensive tests to find out.” They gave me the rundown on what was happening with the baby and so forth. They said, “We’re going to give you iron infusions.” Every time they gave me iron infusions, my hemoglobin kept dropping back again. They were like, something is going on.
Describe your delivery and postpartum
Before you have any major surgery, your hemoglobin has to be a certain number. Mine dropped right before my due date. Prior to then they were trying to take him early and I said, “Nope, his birthday is this date and that’s what it is.” When it came down to the actual day, I said, “Well, what are y’all going to do? Y’all can’t leave him in there, you have to take him.”
They gave me all these antibiotics. They were really concerned about doing major surgery with your hemoglobin being low. I delivered the baby and nothing else was said about the hemoglobin being lost. Nothing.
When I came home, I started noticing excruciating back pain. I was like, something is wrong with my back. I went to my primary doctor who had me do x-rays. She said, “Well, nothing’s wrong with your back. It may be the epidural.” Then my stomach was acting really weird. My stool had changed. When I would eat, I felt like I had diarrhea, but it wasn’t diarrhea. The doctor said, “You have irritable bowel syndrome” and gave me some pills for that. I didn’t know then about questioning the doctor more.
Then one day at work, I went to urinate. I was not on my cycle or anything. I turned around and it looked like a massacre was all over the toilet, there was blood everywhere. I took a picture of it and cleaned it up. I was at work and it was in the afternoon.
Diagnosis
Symptoms worsened
I went to my doctor and I said, “This is what happened when I was at work, and it was the only time that this particular thing happened.” She said, maybe it’s hemorrhoids. It was always a, “Maybe it’s this, maybe it’s that” kind of thing. Mind you, for a whole year, I’m going to the doctor for the back pain and my stomach with my babies in tow because I’m like, something is not right. I thought, well, maybe it’s me. You start thinking, is it in my head? Am I really having this? Are these symptoms really that weird?
It wasn’t until one morning that I was getting ready for work. I nursed my son as usual. Afterward, I had this really sharp pain under my right breast and I was like, that’s weird. I continued getting ready, and this is at 4:00 in the morning. I dropped him off as usual and went to work. I had to work a 16 hour shift that day.
I was sitting there with my co-worker and I said, “I’m having this sharp pain.” It was getting sharper, deeper, and really fast. We were sitting there and going, “Maybe it’s your appendix, maybe it’s this, maybe it’s that, maybe it’s gas.” It was a variation of maybes. I said, “I’m going to go to urgent care on my lunch break and let them see what it is.”
You start thinking, is it in my head? Am I really having this? Are these symptoms really that weird?
I went and the urgent care physician said they do not have the equipment there to do any testing. I need to go to the emergency room because maybe I pulled a muscle or it’s gallstones. At that point, I was like, I’m not going to the emergency room for a pulled muscle. What if that’s just what it is? I have to work a 16 hour shift. I’m just going to go back to work. My supervisor told me, “Do not come back here without going to the emergency room first to see what is going on.” I was like, “But what if it’s a pulled muscle?” She said, “If it’s a pulled muscle, then at least it’s a pulled muscle and you know.”
Taking a trip to the E.R.
You don’t think that it’s anything huge. On my way to the E.R., I prayed. I said, “God, I’ve been praying that they don’t find anything. But today, God, I’m asking you, let them find out what it is because something is not right.” Everything just lined up. They took me in right away. I didn’t have to wait.
They started giving me morphine because I couldn’t lay down at this point. I could not lay flat. The pain was so bad. I described it as a throbbing toothache in my stomach. They asked, “What does it feel like?” I said, “A throbbing toothache in my stomach.”
They did an ultrasound and other tests. A lot of that was a blur. I remember the ultrasound and one of the tests came back. They asked, “Has anything come back about your liver, the tests or different things you’ve taken? Have you been going to the doctor?” I said no. He said, “Hmm. We found a mass on your liver, but don’t worry, it could be benign.” I said, okay. I never paid attention to what happened after that because they told me it was gallstones and that they’re going to remove my gallbladder in the morning.
I was admitted to the hospital. But I never paid attention to the fact that I was admitted to the oncology floor. It was, someone who was close to me at the time. She said, “Do you know that they admitted you onto the oncology floor?” They had a suspicion and I did not know anything that whole night.
Receiving a cancer diagnosis
The next morning, right before surgery, the admitting physician walks in and says, “You have tumors and it’s colon cancer.” He just said it. He just walked in and said it. I was like, whoa. No one was with me. It was hard to process something like that because, in my mind, I didn’t think cancer. My thing is, I’ve been going to the doctor for a whole year. They never connected the actual dots. I went to the hematologist for the pregnancy, but no one said anything afterwards. They told me in the hospital that something is going on but we don’t know what it is and we can’t do the testing.
No one said after I delivered that baby, let’s talk about what’s been going on. Let’s talk about you weren’t supposed to have a C-section with your hemoglobin being at that level. No one spoke on it. It was really confusing. These are not like the best doctors or anything, because there are some phenomenal doctors out there.
I do tell doctors now, “See me how you would want to be seen or how you want your loved ones seen.” Being a dispatcher, I don’t see names. I don’t see who we’re helping, but to all, I always try to go above and beyond. You don’t know when you may need help.
How did you react to your diagnosis?
I thought it was a death sentence.
No one expected this. The people that knew I was getting ready to have surgery cried. I had people that called me and I cried with them. At one point, I was comforting people like, “It’s going to be okay. It’s going to be okay.”
All I could think about were my babies. I said, “God, why? Why are you taking me from my babies you just gave me?” That’s all I could think about. I thought it was a death sentence. It’s something that I wouldn’t wish on anyone to receive. Even if it’s expected, it still hurts to hear it.
At that point, they did a colonoscopy and they said, based on the scans, that it was for sure colon cancer. They could not tell me the stage. I had to go see a specialist afterwards and I did not go right into surgery.
I met the first oncologist I had. I’ve only had two. The first one I had was all facts and evidence. Every question you asked him, he’d say, “Facts and evidence says this and facts and evidence says that.” He got to the point where he was unreachable.
My insurance, I didn’t know, did not cover me getting treatment at the hospital that I was at. I would have to change [medical care] and that was the best change. God was all in the math for that. The oncologist that I have today [helped me] get in remission. He’s still my doctor. He’s just a phenomenal person and he cares about my life.
Beginning chemotherapy
He ordered that I start chemotherapy. I had to get 12 rounds of aggressive chemo. Aggressive chemo was something that I was not prepared for. The first oncologist told me, “You’re still going to be able to go to the gym. You’re going to be able to run around after the kids. You’re going to be able to do all these things.” Research showed that people do these things while going through treatment.
Firstly, we were going to do 6 rounds of chemo and then surgery, but we ended up doing 8. Then I went back in for the last 4 afterwards. With colon cancer treatment, one of the drugs I had was Avastin.
Before I did chemo, I had a cruise already booked for my sons and I. It was a birthday cruise for my oldest. I went on that cruise, came back, and started treatment. The same day that I came back, I had to get my port placed that morning, and I said, “This is it.” I found a video the other day that I didn’t know I recorded of my sister taking the bandage off of my port, and I said, “I’m going to keep this in for one year then we’re going to be done with this thing.”
What was your experience on chemotherapy?
Treatment was not what I expected. Nothing could have prepared me for what happened. I was so sick, treatment was hard, and it was depressing. I’m not going to lie, I dealt with depression in a different way. I always show up and smile like nothing is wrong, but this was different. I had to sit in it.
I couldn’t be around people. This was before COVID. I was wearing masks and gloves before COVID. I’d get stares and my kids had to be careful around me. They had to go to daycare and school but had to watch out.
Chemo was 46 hours total and I had to get the Neupogen shot after that. I didn’t know what Neupogen was. After a few rounds of my white blood cell count going down, they said, “We’re going to give you this Neupogen shot and it’s going to bring your cell count up.” I’m like, okay, cool. Let’s go.
Oh my God. That shot is traumatizing. I’m traumatized to this day from what it does. The bone pain is not mild. It always started at my neck like a heated rush. Then it felt like something was breaking my bones. It would go down my body, just breaking. It’s paralyzing pain. I felt like I couldn’t move or touch anything, just scream.
I switched to the University of Miami where I met my surgeon. Before I started treatment, he said my liver was covered in masses. Only a small portion of it was clear, but the majority of it was covered. I knew that I would have to end up getting surgery. He told me that he considered it because of my age. If I was older, he would not recommend something like this. The liver is a huge surgery. I didn’t know how huge it was because it’s bloody, it’s all the above.
I did about 8 rounds of chemo and then it was time to go into surgery. Two weeks after I did chemo, they withheld the Avastin, but I did the other chemo. FOLFOX at first and then I went to FOLFIRI. I didn’t recover well enough but went straight into this huge surgery.
Before I started treatment, he said my liver was covered in masses. Only a small portion of it was clear.
I didn’t know how to speak up for myself or say, hey, wait a minute. Is what we’re doing a lot? The conversation when you’re dealing with the cancer world is, “We’re trying to save your life so we’re going to do this, this, this and this, and you just gotta deal.”
I went into surgery. They put me to sleep really fast. I woke up from the surgery and I wasn’t sent to the ICU. I was sent to a regular room to be admitted. They said the surgery went fine. The conversation was to remove 60% of my liver but the surgeon removed 70% of my liver. That was the first time that I was diagnosed. I was diagnosed three times and that was the first. Mind you, this was in the era where colon cancer in a young woman was not the norm. This was in 2017. Now you’re starting to hear more about colon cancer in younger people.
Relapse
Was your cancer treatment successful?
When I went back to my primary [care doctor] where this all started, he was so nervous. They said, “We would have never suspected this in a young, fertile woman.” I immediately became a case people were curious about. Wait a minute, you had stage 4 colon cance? I had it when I was pregnant.
After that, I was told. “Hooray! You’re in remission.” After the surgery, I had to go back for what they called a clean-up chemo, just to make sure that there was no residual [cancer]. They kept saying, “Hooray, hooray, you are in remission.” I didn’t know how serious colon cancer is. There are other cancers where you can be stage 4 or 3, but they’re curable. Colon cancer is the second deadliest cancer, so it may not have been curable. I did not know that at that time. I was like, why are they so surprised that I made it?
This was in the era where colon cancer in a young woman was not the norm…Now you’re starting to hear more about colon cancer in younger people.
My oncologist said, “You’re in remission. This is good news. This is celebration time.” So I did what I love. I went on a 3 day cruise to celebrate that I’m still here. After the cruise, I said, “Let me live life a little.” I took my kids to go see snow in Baltimore. I was living life.
Did you receive follow-up scans?
At the same time, I was having this pain on my right side. When I went to the surgeon and said, I’m in pain, he told me I should not be having pain still. “The surgery was a success,” is what he told me. He went on to say, jokingly, “Maybe it’s because you don’t want to go back to work.” I was really annoyed because I said, “I actually like my job. If I’m having pain, I’m having pain.”
My mom is like a doctor without the degree. She researches everything. She would go with me to these appointments, so when he said that, she said, “How about we do a scan to find out why there’s still pain?” I said, “Yeah, let’s do a scan. Let’s find out what’s going on.” We did this scan and it sat on his desk for about a month or so, maybe longer.
Experiencing cancer relapse
When I came back, I started getting all these phone calls. They called me back to back. The nurse said, “Hey, something showed up on the scan that you did back in December.” Now we’re in January. “The surgeon wants you to go see your oncologist.” I went to the appointment. Before I went to the appointment, I went on the the app to see my results to see why they’re calling me. “Nodule in the right lung has grown since August.” I said, what?
Now I’m looking up nodules. I saw that it could be pneumonia, it could be this, it could be that. I believed it could be pneumonia because I had just left the E.R. after that scan. They told me I had pneumonia. The nurse practitioner confirmed it wasn’t pneumonia, it was indeed cancer. Now I was confused because I’d just left the emergency room and they didn’t say anything. They said, “Well, maybe they figured you already knew.”
I thought, this can’t be it. The surgeon did not speak to me. He did not deliver the news. I went to my oncologist. He was very caring, phenomenal, and the first words out of his mouth were, “I hate that you have to start the year off like this.” I went to see my oncologist, let’s just say on a Tuesday, and he already had chemo scheduled for me to start in 3 days or so.
The nurse practitioner confirmed it wasn’t pneumonia, it was indeed cancer.
They had to do a PET scan to see where all the cancer was at. It was in my lung and it came back in my liver. Mind you, I just had surgery on my liver. Now the concern was, if we cut any more of my liver…There are so many concerns. Then the oncologist said, “Okay, before chemo, we’re going to do the surgery. We’re going to have the lung surgeon go in and remove that nodule.” He said the only way to get cancer out is to get it out, so let’s go there first.
What was your next course of treatment?
Right before the surgery – this is how you know your doctor is really thinking about you and really concerned – he calls and says, “You know what? I thought about it all night. I looked at your scans all night and I think it’s best to do chemo. Let chemo get as much out of it as it can, and then we’ll do the surgery.” Well, this time I knew what chemo was going to be like. I knew what to expect. I knew the biggest part was the neupogen shots.
That chemo took away the cancer in my liver so they just had to remove the nodule from my lung. It was then that my oncologist told me my prognosis was a 15% [likelihood] of me making it through that, but it goes down every time you’re diagnosed. That was a very humbling moment because I have small babies. It puts a lot on you. It takes a toll. I did that, went into remission, rung the bell, I had a whole party, and I was good.
Side Effects
Processing cancer complications
My oncologist told me my prognosis was a 15% [likelihood] of me making it through that.
I went back to work and a friend’s husband had passed away from stage 3 colon cancer. I got to the point that I took a break from cancer completely. It wasn’t a [long break]. I just made up my mind, I’m not going to scans. I’m not doing anything. I just don’t want more news. I’m done with cancer. She told me, “You’re going to those scans.” She made me go.
I went to go get the results. This was the same week COVID happened, but this was a few days before the world shut down. I went to the doctor and we were talking like I was good. Then the doctor said, “There’s an area of concern.” I literally broke because it was that week that things happened between my ex-husband and I that I was hurt by and then the cancer.
I was like, what is going on? I was trying to co-parent and all these things. I broke down. I think that was the biggest shock of my life. I just did not expect it. This time, it was more than just going right back to chemo again. I was diagnosed on Thursday and Tuesday I had to start chemo. He already had it planned out for me before I even got there. He’s such a phenomenal oncologist. I really do thank God for him. I said, “I’m just tired.” At that point, I was tired of life. I just didn’t know what to do.
Did you have side effects on chemotherapy?
I went to chemo. I would show up to chemo with my graphic t-shirts, light up shoes on, make up, and head wraps. This time he changed it to full fury. He said, “I don’t want the burns on your hands. I don’t want all these things. I’m gonna do full fury with you this time.” It was that chemo that took out my hair. The bone pain was crazy. Also, chemo brain.
I had a lot of chemo in a short period of time. It wasn’t spaced out. It was almost 4 years back to back. People didn’t get it. People look at you and say, “There’s nothing wrong with you, you’re good, you’re together,” but there’s so much inside.
Also, my teeth. My teeth are a big thing for me now. I had braces when I first started chemo. I was told by the orthodontist and dentist that I would be fine, and I probably would have been fine that one time, but I had a second and third time. I still went to them and they were like, “Everything is going to be fine.” When they got ready to take the braces off, the enamel from my teeth started coming off with it. Little by little, my teeth just kept decaying and my dentist told me it was going to continue because at this point, the chemo had rotted my teeth. When he showed me an x-ray from me being there just one year before until that time, it looked completely [different]. I had just had all this dental work done. Dental is a big thing of it.
There’s a lot in the mental and emotional side of it. I can honestly say I went to a deep, dark, place that this can take you to. At one point, I felt like I was trapped and could not get out.
I had a phenomenal surgeon. I love him, he’s so honest. I had 4 major surgeries at one time. One was a full hysterectomy because I was told that in women the cancer tends to hide in their uterus. I spent about 10 days in the hospital. That was the minimum that they required. I don’t have a colostomy bag. They did not remove my entire colon. They removed 34 lymph nodes from my stomach, a lymph node near my left kidney, the full hysterectomy, and my gall bladder. I think that’s it. They would have kept me longer, but mind you, it was during COVID. My heart goes out to people who have to be in there longer.
My last treatment was April 2021, and I’m just relieved. I started to see remission differently. Remission is a waiting period. They’re waiting for something to happen because they’re big on, after 5 years, I’ll celebrate with you. I had a phenomenal surgeon. He even said, “After 5 years, I’ll celebrate with you.”
Reflections
Whatever gives you peace while going through something like this, find that and protect that.
Do you have any advice for cancer patients?
I would say, be your own advocate for your health. Ask the questions. Do not feel scared to ask questions. Do not feel scared to try things. You have to be at peace with your own decisions at the end of the day. Some people are anti-chemo, some people are for it, and some people grew a garden and that’s how their cancer went away. Whatever it is, you have to make sure that you’re at peace with every part of it.
Don’t just take the first answer that’s given. Go research some more, ask the questions, and research more. One more thing, for me, my faith was a huge part of it. Mental and emotional, the way you go into this is huge. I always smile. I was told by a lot of nurses and doctors that because I smiled through it all, that that’s the reason why I made it. I’m not saying that you have to smile. That’s not my thing. I’m just saying, whatever gives you peace while going through something like this, find that and protect that.
Cancer Details: Diagnosed 2 weeks after 5 years remission from testicular cancer 1st Symptoms: Inflamed bowel Treatment: Subtotal colectomy, immunotherapy
Cancer Details: The sigmoid colon (or pelvic colon) is the part of the large intestine that is closest to the rectum 1st Symptoms: Stomach discomfort, nausea, bloating, blood in stool Treatment: Colectomy
Cancer Details: Discovered Lynch Syndrome after genetic testing 1st Symptoms: Found the cancer as a result of family history, early colonoscopy Treatment: Partial colectomy
Cancer Details: Family history wasn’t flagged, should have had colonoscopy earlier 1st Symptoms: Stomach discomfort, difficult to process food Treatment: Colectomy, Chemo (FOLFOX, CAPOX)
Cancer Details: Had no usual first symptoms, found as a result of routine colonoscopy and endoscopy 1st Symptoms: None Treatment:Partial colectomy, chemotherapy (FOLFOX)
Cancer Details: Diagnosed at 32, cancer spread to ovary and lung 1st Symptoms: Lump in pelvic area, funny-smelling food, weight loss Treatment: Chemotherapy, colectomy (surgery)
Symptoms: Abdominal pressure, fatigue, small amounts of blood in stool Treatment: Surgery (colon resection), chemotherapy (FOLFOX: folinic acid, fluorouracil, and oxaliplatin)
Kelly B.Diagnosis: Stage 3 Colon CancerSymptoms: Blood in stool, cramping, bloating Treatment: Chemo, surgery
Courtney H.Diagnosis: Stage 1 Colorectal CancerSymptoms: Blood in stool, fatigue Treatment: Chemo, oxaliplatin, capecitabine, surgery
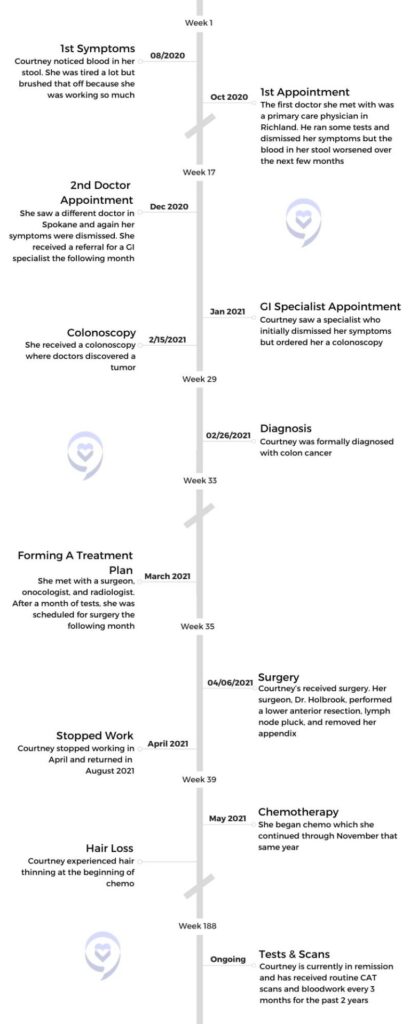
Courtney, a high school English teacher from Spokane, experienced symptoms such as fatigue and blood in her stool that led her to suspect she had colon cancer. Despite initial dismissals from multiple doctors due to her age and lack of family history, Courtney persisted in advocating for herself, ultimately undergoing a series of tests, including colonoscopies and scans, which confirmed her suspicions. Diagnosed with stage 3A colorectal cancer, Courtney underwent surgery to remove the tumor and lymph nodes, followed by chemotherapy as a precautionary measure.
Throughout her treatment journey, Courtney faced various challenges, including side effects from chemotherapy such as hand-foot-and-mouth sores and neuropathy. Despite these obstacles, she pushed forward, continuing to teach full-time and engaging in physical therapy to regain her strength. Three years into remission, Courtney emphasizes the importance of self-advocacy, listening to one’s body, and pushing for answers, especially when faced with medical dismissals or ambiguity. She encourages others to trust their instincts, seek support from loved ones, and persevere in navigating the healthcare system to ensure proper diagnosis and treatment.
Name: Courtney H.
Diagnosis (DX):
Colon Cancer
Staging:
3A
Symptoms:
Blood in stool
Fatigue
Treatment:
Surgery
Chemotherapy
Capecitabine
Oxaliplatin
Advocate for yourself, know your body, listen to your body, and keep pushing until you find answers.
Courtney H.
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
My name is Courtney. I am a teacher. I teach high school English – specifically honors 9 English and mythology. I am a big lover of reading. I like to play outdoor volleyball, garden, and explore. I live in Spokane, in the Pacific Northwest. It’s so beautiful. We have four seasons and lots of activities and different things to do. I like to spend time with my niece and nephew.
What were your first symptoms?
I took an anatomy and physiology class in college, and one of the only things I remember from that was that the professor said, “Most often when you have internal bleeding of some sort, it is your body’s inability to heal itself, and that usually comes in the form of a tumor.”
What had happened was I had gotten a teaching job in Othello, where I grew up, and I moved down there. This was August of 2020. I was a very busy new teacher. I was the head cheer coach for a cheer program. I worked a lot of jobs in grad school, and so I just was very used to being on the go all the time and having a busy and packed schedule.
I knew I was sick. I knew I had colon cancer, so I just kept pushing.
When I moved to Othello, I started showing one symptom – I had blood in my stool, and I instantly knew. I knew instantly that I had colon cancer. Moving down to Othello, I had to get all of my records and everything transferred down there, including all my medical stuff. So I wasn’t able to go in and see a doctor until October. My symptoms kept progressing, and I just knew when that started happening. I was trying to find somebody that could help me find the exact diagnosis. The answer.
Did you have any additional symptoms?
Just blood in the stool and fatigue. My friend’s mom, who’s a nurse, did a blood test on me and she said I was very anemic. What we ended up finding out when they had taken the tumor out is the blood flow was feeding the tumor, and that’s why I was so anemic.
The first general practitioner doctor I went to, he dismissed all my symptoms and said, “There’s nothing wrong with you. You’re thin, you don’t have a family history. You just need to make some dietary changes.” I was like, “Well, I’m going to keep trying to find answers.” It was in the middle of COVID, so everything was pushed back. Then symptoms kept getting worse. When I came home for Christmas break – home was Spokane – I saw a different doctor and it was the same thing. He spent about an hour with me, ran some tests, dismissed all my symptoms, but I knew I was sick. I knew I had colon cancer, so I just kept pushing.
The first doctor in Richland, he actually had put in a referral for me to see a GI specialist. I was able to see a GI in January of 2021 and [experienced] the same thing. She dismissed all my symptoms. Finally I said, “Listen, this isn’t about you being right or me being right. This is about figuring out what’s wrong. You’re speculating and I’m speculating.” They were all saying, “We think you have Crohn’s or diverticulitis, diverticulosis, or a bleeding hemorrhoid.”
One of the greatest skills that my parents ever taught me was the ability to advocate for myself and to know your body.
I said, “No, I think that I’m sick. What can we do?” She said, “Well, we can give you a colonoscopy. You’re too young and they’re very expensive.” I said, “Well, I’m a teacher. I have great health insurance. We need to do this. I think it’ll give me peace of mind knowing that we have tried everything.”
Receiving a colonoscopy
Months later, she did a colonoscopy and found the tumor. That was February of 2021. That whole month and a half that I went through 9 different tests. I did 3 colonoscopies, a sigmoidoscopy, 2 CAT scans, a PET scan, and an MRI. There’s another one I did but I can’t remember the name of it. All of those tests brought me to the diagnosis. Now what are we going to do? What’s the plan of action going to be? I got a team together.
What tests did the first doctors do?
He did a blood test and some general stuff. He felt my stomach to see if I had any lumps or bumps. Then he went through and looked at family history. Obviously, I don’t have a family history of it. He said, “You’re thin, you’re not pre-diabetic.” I was in Richland, Spokane, and then I went to Kennewick. So three different cities, three different doctors. The doctor in Spokane pretty much did the same thing. They didn’t do anything extensive because you can’t really diagnose it unless you actually get a colonoscopy.
The problem was, neither one of those two doctors could perform that. Then they just dismissed my symptoms. They said, “Well, we’re not going to put in a referral for you to have a colonoscopy because we don’t think, from our experience, that you have it. I really had to beg the GI specialist to give me one.
We did a blood test with the first doctor and he didn’t see anything abnormal. Then the doctor in Spokane didn’t really see anything abnormal. But my friend’s mom, who’s a nurse, knew what to look out for because I told her what was going on. She did her own test and said, “You are severely anemic. Something’s going on.”
Did your insurance cover the cost of the colonoscopy?
I paid a little bit out of pocket, but it was mostly covered. The problem was, and this is something that I think a lot of people run into when they’re getting tests done, especially a colonoscopy or sigmoidoscopy. My insurance company did not want to pay for the right type of drugs. I didn’t know that. I didn’t hear the confirmation. They actually had to tell my parents, and it took 8 hours for the drugs that they gave me to wear off. So I actually didn’t find out about the tumor until the next day. My parents waited to call because they tried to talk to me after the procedure and I was just bonkers.
Surgery
The importance of advocating for yourself
They dismissed the symptoms because I didn’t fit the profile, but one of the greatest skills that my parents ever taught me was the ability to advocate for myself and to know your body. I just knew I was sick. I had that feeling in my stomach. Sometimes science can only go so far, and sometimes you have to put it in your own hands and keep pushing for it. It was a unique set of circumstances, because when I did my colonoscopy, COVID cases were very light, so I was able to go in and get a colonoscopy. When I had my surgery, COVID cases were really light, so they didn’t push my surgery back. These were just perfect little windows where things ended up really working out in my favor.
Formulating a treatment plan
Because I didn’t have the right drugs, she couldn’t finish the colonoscopy. I would have to come back 4 days later and do another one. I came back that Friday. I had [the first one] done on a Monday, came back that Friday, and everything else looked clear. She said, “I’m 98% sure that this is a cancerous tumor. We’re going to send it off to have it biopsied.”
It took two weeks to get back. The next conversation, I said, “I know a surgeon who saved my dad’s best friend’s life. He had stage 4 rectal cancer and he’s been in remission for 20 years. I want that guy.” She was going to put in a referral for somebody else. I said, “No, I want this guy.” Then everything started to move, all the tests.
After all of the tests came back – because the original plan was to do some radiation, 6 weeks of chemo, and then do surgery after the MRI, – the radiologist called me and said, “This is miraculous, but your tumor is a lot smaller than we thought, so we’re going to operate. Nothing else is lining up in your body, so we’re just going to go for it and operate.” So they did.
Describe your surgery
Dr. Holbrook went in and did a lower anterior resection and took out part of my colon, 21 lymph nodes, and my appendix. He said, “I had a stage 4 appendectomy patient who’s 17 years old last week. I just thought I’d take your appendix out.” He spent about 4 hours in surgery. He just retired last year, but he’s one of the best in Spokane. I trusted him.
The prep work was I had to go onto a liquid diet about 48 hours before. They gave me some things that they wanted me to take prior. After I was in the hospital for about 4 days, I had a series of things that I had to go through to get out of there. I had round the clock bloodwork. They would come in at 2 a.m., they’d come in at 6 a.m.. They were checking fluids and different things like that.
As far as the procedure, he just went in. He didn’t tell me how much of my colon he took out, but he took out the sigmoid region of the colon. That’s the end. He took that part out and did the lymph node pluck. After that, I was on a liquid diet for about 3 weeks, giving my bowels a break and allowing things to heal. He was able to go in and do it minimally. The incision where he went in was about this big. He was able to go in right underneath my stomach and do it.
Chemotherapy
What stage were you in?
We got a really good prognosis back. I had a stage one tumor. There were just a few little cancer cells that had broken off and gone into one lymph node, so I had a really good prognosis.
Preserving fertility before starting chemo
I had my 3 week clearance from surgery, and then I actually harvested my eggs, and then I did chemo. It was boom, boom, boom. My body had been through some things. Harvesting your eggs is quite an interesting process. I didn’t know this. When you go through and you do all the things, they monitor you, they take your temperature, they do all the things.
The day before my procedure, they did a COVID test on me and it came back positive. I didn’t know I was asymptomatic. Seattle Reproductive had to fight with Seattle to advocate to harvest my eggs because it’s a $15,000 procedure. They ended up saying, we’re going to suck it up, risk it, and do her procedure. Then I started chemo right after I was cleared from COVID.
I didn’t have to do chemo because of my prognosis, but my surgeon and team recommended that I do it as an insurance policy. I was prescribed 2 different types. I had an infusion chemo which entered through a port and a pill chemo. I would do one infusion every 3 weeks. Then I was on pill chemo for 2 weeks at a time and I’d get a break at the end of it.
Which chemos were you on and did you have side effects?
Capecitabine. The infusion chemo was called oxaliplatin. I had side effects with each. With capecitabine, I had hand-foot-and-mouth, where you get really bad sores everywhere. The other chemo was oxaliplatin. It’s a platinum chemo. It had some really strange side effects. You couldn’t touch anything cold. You couldn’t ingest anything cold. I couldn’t drive in my car with the AC on or it could close my throat. Everything had to be room temperature or hot.
It was in the middle of the summer, so one of the biggest issues I ran into was I was dehydrated a lot. I was hospitalized 2 different times for dehydration which was scary. I lost a lot of weight. I think I lost about 25 pounds. I tried to eat when I wasn’t hungry. I had to watch what I ate. They tell you you can’t have raw fruits and vegetables while you’re on chemo, which is so weird because you should be eating healthy foods, and they said to eat what I could.
The first two days after infusion chemo and pill chemo, you’re the sickest, you’re nauseous. It’s really, really hard to get up and move around. With oxaliplatin, like I said, it’s a platinum chemo so it causes neuropathy. You have a lot of tingling going on in your body. It got to the point where my eyes were affected by it. I could taste it in my mouth. It was very all-consuming throughout my body.
Stopping oxaliplatin
I did my own research about my particular prognosis and I decided to stop oxaliplatin after 4 rounds. That’s the infusion chemo. A lot of patients push past that, and there are some patients that end up disabled from doing that chemo. I did not want to do that. I didn’t want to risk that. It was making me so sick that I could barely eat.
Did anything help alleviate your chemo symptoms?
When I was dehydrated, I would go in and get pumped with fluids. That helped. I did take Zofran to help with the nausea. You can’t be in the sun either when you’re on chemo. You have all these things that you can’t do.
The best thing that helped with the side effects was to get my mind off of it.
I think for me, the best thing that helped with the side effects was to get my mind off of it. I taught full time while I was on it. That was my choice. I didn’t want to lay in bed every day and dwell on it. That’s just my personality so I decided that I was going to work and let that be the thing that would help get my mind off of it. I did oxaliplatin for 3 months and capecitabine for 6 months.
When I went back to school to teach, I did physical therapy and that helped a lot. It helped me build up strength because I had lost so much muscle mass and lost so much weight and it helped with getting through those days.
Reflections
How long have you been in remission?
I am almost at the 3 year mark of being in remission. I count it as April. My oncologist counts it as November because that’s when I finished chemo, but I think that the surgeon got everything.
How often do you get scans and do you experience scanxiety?
I don’t think that it ever really leaves you. I think that it stays with you.
I just hit the 2.5 year mark, so now I go every 6 months. I think that’s one of the hardest parts. I was joking with a friend that I’m a part of an exclusive club now because it doesn’t really ever leave you. With scanxiety, I just do my best to just try and stay positive. It’s always quite exhausting because it’s a 4-day process – blood work, scan, and meet with your doctor.
My aunt is a phlebotomist, so she’s always encouraging, giving me tips on how to stay positive and hydrate, make sure you’re ready to go. But it is a real thing, and I honestly don’t think that it ever gets any better. I think that you learn how to manage, how to live with it. The farther out that you get, you feel better. But I don’t think that it ever really leaves you. I think that it stays with you.
What advice do you want to share with cancer patients?
Advocate for yourself, know your body, listen to your body, and keep pushing until you find answers.
You need to advocate for yourself and you need to be able to listen to your own body. Science only goes so far. Knowing, understanding, and listening to your body is really important. Because if you’re sitting in front of this doctor that doesn’t know you, you’re just a statistic. They’re trying to see where you fit, and if you don’t fit the category, you don’t fit the profile, of course they’re not going to suspect anything.
I also think that you have to hold on to your faith and keep pushing through roadblocks and things that are in your way. You just have to keep going until you find the answers that you really desire to have. For me, that was, I’m sick of hanging out in ambiguity. I know I have it. You are speculating, but that’s why we have science. That’s why we have these things. We shouldn’t be profiling people based on their age or the way that they look. We should be listening to the patient and to their concerns.
Advocate for yourself, know your body, listen to your body, and keep pushing until you find answers. That’s why I’m alive and well today, because I advocated, and I continued to push until I got the answers that I needed. I don’t blame any of them. They’re doctors, they’re human, but I do think that they need to listen to patients better. I think that they need to listen to their patients, listen to the concerns that they have, and really do a better job of putting something in place that is going to help. Help eliminate this ambiguity. For people that may not feel as comfortable to advocate, you just have to remember that you know your body. So even if it’s something that’s totally foreign, talk to somebody about it and try and find those answers that you are desiring to look for.
Kelly, a small-town entrepreneur from Illinois, received a life-altering diagnosis of stage 3 colon cancer shortly after celebrating her 50th birthday. Despite her active lifestyle of flipping houses, running a tumbling gym, and being an avid runner, Kelly noticed concerning symptoms such as blood in her stool. Despite initial dismissals by her primary doctor, Kelly persisted in seeking answers, ultimately leading to a diagnosis of a sigmoid colon tumor.
Her journey took an unexpected turn during surgery when complications arose, prolonging her hospital stay. Despite setbacks, Kelly’s determination to advocate for herself remained unwavering. She navigated through treatment options, including chemotherapy, with a strong sense of autonomy. Kelly’s decision to undergo chemotherapy was not without doubts, but her resilience and determination prevailed as she faced the challenges of treatment.
Chemo has proven to be a daunting experience, marked by side effects. However, Kelly’s perspective on life underwent a profound shift. Embracing each day with a newfound appreciation and a sense of urgency, she encourages others to live without regrets and prioritize self-care.
Name: Kelly B.
Diagnosis (DX):
Colon Cancer
Staging:
Stage 3
Symptoms:
Blood in stool
Cramping
Bloating
Treatment:
Surgery
Chemotherapy
12 rounds
Cancer or no cancer, you’ve got a life to live.
Kelly B.
This interview has been edited for clarity. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
My name is Kelly. I’m from a small town in Illinois of about 800 people. I was diagnosed with stage 3 colon cancer on November 1st. I wasn’t expecting that from my 50th birthday.
I own two self-employed businesses. I started flipping houses 5 years ago – I’m on [house] number 9. It was a hobby and it turned into an obsession. I absolutely love buying old houses and turning them into something brand new. Picking colors, flooring, and all that stuff. I’m the tear out girl, so I do most of the construction work pulling things out myself, such as drywall, cabinets, you name it, I’ve done it. I can do everything but electrical.
I also own a tumbling gym with a hundred athletes, and we compete competitively throughout the state of Illinois. We attend nationals once a year. Sometimes we go to West Virginia or to Florida. It depends on where we’re at that year. I have since taken a leave of absence from both jobs due to the diagnosis.
My hobbies are running. I love to run. I ran the marathon and half marathons. I’ve been running consistently for years. I journal a lot, even prior to the diagnosis. I was just settling into accepting the empty nest thing after my son went off to college 3 years ago, and getting into a groove. I love to travel to Florida. I’ve been back and forth to Florida 6 or 7 times in the last year, and that’s actually when I started seeing signs that something wasn’t right, in June.
What were your initial symptoms?
My first symptoms were that I had blood in my stool. I was actually in Florida in June, celebrating my 50th birthday with all of my kids, and I chalked it up to something that I ate. Maybe it wasn’t blood. I talked myself out of it thinking it was something that I ate or I was drinking red ice drinks a lot.
It continually kept happening and it seemed to happen more when I was in Florida, which I thought was strange. I didn’t have anything other than blood in my stool, which I knew wasn’t normal. I thought it could be anything, really. I didn’t think for a second that it was colon cancer.
I associated cancer with low energy, losing weight, and just not feeling well. I felt really good…Doctors kept telling me I was fine.
I came home from my trip, scheduled an appointment with my primary doctor, and saw them at the end of June. They told me that they thought it was hemorrhoids and I shouldn’t be too worried about it. I again saw them because it continually happened probably 2 or 3 times a week.
I wasn’t losing any weight, so I really wasn’t that concerned but I was concerned enough to continue to call my primary doctor. I saw them again in July. I wanted blood work to see where my levels were at. My dad died of a brain tumor at the age of 56, so I went in for cancer screenings once a year, but nothing came up.
What did blood work show?
I had blood work done. My NPV level was the only thing that was flagged as low. I think it was at a 7 and they were not concerned about that at all. I took that and decided I’ll just keep coming back until somebody gives me some answers.
I went back 2 times in July and 2 times in August. They finally sent me to a specialist in October – a gastro specialist. He saw me and he said he would schedule me for a colonoscopy, but told me not to be worried. I did, at that point, start to have some cramping in my stomach and maybe a little bit of bloating. Again, I just turned 50 in August, so I thought maybe it was menopause. Maybe I was just getting old.
Did you suspect you had cancer?
I associated cancer with low energy, losing weight, and just not feeling well. I felt really good, even though I was continually having blood in my stool and a little cramping. Doctors kept telling me I was fine. I finally did go see the specialist and he said it was all good.
Diagnosis
Receiving a colonoscopy
I’d never gotten the call back to go get a colonoscopy. Here I am 3 months later after being diagnosed with stage 3 colon cancer. That was frustrating because nobody would take me seriously until I went and got another opinion. She scheduled me for CAT scans of everything from the waist up to rule that out, then the waist down.
They found a large mass in my colon so they set me up for a colonoscopy. I did the colonoscopy prep on my favorite holiday, Halloween, which is awful. The prep didn’t go well for me because I’m a puker. I was not really pooping like I was supposed to. I was throwing up.
We did the colonoscopy on November 1st, and the doctor came in after I woke up, they took us to a little room, so I figured it was not good news. He said it was 100% cancer.
How did you react to your diagnosis?
I’ve been going to the same doctor for years. It’s not like I didn’t trust them, but I had to trust myself more, and I knew something wasn’t right.
I said, “Okay, let’s go to Applebee’s. I’m hungry.” My daughter was devastated. I thought, okay, we’ll just deal with it however we need to deal with it. That’s it. I wasn’t feeling heard. I knew something was wrong. I didn’t know what was wrong. I’m pretty good at being able to tell what’s going on with my body. I’m very in tune with my body, my feelings, my thoughts. I felt like I was being dismissed.
They kept telling me over and over again, “It could be hemorrhoids.” I said, “It’s not hemorrhoids. I’ve never had hemorrhoids in my entire life. Even when I gave birth to 3 children who are now adults.” I knew it wasn’t hemorrhoids. I started to get a little bloated towards the end of October, but again, I chalked it up to menopause. I almost talked myself out of my symptoms because nobody would listen to what I had to say, and I’ve been going to the same doctor for years. It’s not like I didn’t trust them, but I had to trust myself more, and I knew something wasn’t right.
He said that the tumor was so large that they could not get the camera through on my colonoscopy, even though they changed the camera to a NICU baby size. The mass was too big. I didn’t really understand that because I’m a tiny girl. If I had such a large mass, how could I have not known that? The mass ended up being 11 inches big.
Creating a cancer care plan
When he told me I had cancer, I said, “Okay. Let’s go. What do I do now?” He was urgent, and said, “We need to go now. You need to see a surgeon. You need to schedule this and that.” I was clearly not in a hurry because I’d been dealing with this for months, so I was like, let’s just take our time here, people.
But that’s not how it works when you’re diagnosed with cancer. That was the crazy thing. They said I could have had the tumor for 5 to 8 years. Dr. Kerry was the first one to actually listen to me, listen to my symptoms, and want to rule anything out. She suggested the CAT scans. Of course, I went along with that because I wanted to know what was going on.
After I was told it was 100% cancer and it was time to see the surgeon, they scheduled me in. I went to see him the first week of November. He wasn’t too concerned about getting me in for surgery right away because the tumor was so slow growing that I could have had it for, he said, 5 to 10 years.
Did you have a family history of colorectal cancer?
They assured me that I didn’t do anything wrong because nobody would get me a colonoscopy. I didn’t have any family history of this. It sounds silly, but my friends and I made a pact to get colonoscopies at some point because my best friend’s husband died of colon cancer. So that makes the story a little bit crazier.
Surgery
Not rushing to get surgery
After I saw Dr. Kerry, things moved really quickly. I met with my surgeon, Dr. Modi, who is phenomenal. He’s like a little Doogie Howser and he didn’t push me to go too soon. He gave me a couple of weeks. He told me to go live my life. He knew the tumor was rather large, but he was very confident that he would get it out with the robotic arm hands. Surgery would take about 3 hours, so he gave me 2 weeks to go do whatever I wanted to do.
I really wanted to travel. My kids wouldn’t let me do anything. They were scared it might rupture. I teach gymnastics too, so I went back to work and did my thing.
Describe your surgery
I went in for surgery on November 21st, and that’s when things got really real, because the surgery didn’t go the way I expected it to go. I thought for some reason it was like going to the spa. I packed books and things like I was going to recover fast, and it didn’t happen that way.
My tumor was in the sigmoid colon. Surgery was my only option to get the tumor out. There was not going to be any radiation or chemo at that time. They’d remove the tumor and then we would go from there. We didn’t expect the tumor to be 11 inches, and it was in my sigmoid colon. I had also told my surgeon that I did not want the poop bag. I didn’t even know the correct terms for that. There were certain things I was not going to do, and I guess I wasn’t a really great patient, but I advocated for myself.
Complications during surgery
He ended up taking my colon out of my body, setting it on the table, fixing it, and putting it back in.
We went in for surgery on November 21st. It was supposed to last 3 hours. Apparently it lasted 7, because my prep didn’t go well. When he had me on the table, it was supposed to be laparoscopic, robotic, for incisions to get the tumor out, but he ended up having to open me up because I started to fill up with poop.
He ended up taking my colon out of my body, setting it on the table, fixing it, and putting it back in. The strange thing is, I remember going in at 7:30 in the morning and I had no doubt it was going to go very easy. When I came out of it and I started to wake up, there were so many people in the room and it was dark outside. I knew something wasn’t right and that it didn’t go as well as he had expected it to go. He ended up having to call in a colleague to help him with all of the feces.
When I woke up, I wasn’t too happy because I had the incision, but I didn’t have the poop bag. I didn’t have to worry about that because there was a certain way I was going to live my life after this, and it wasn’t going to be with that. No disrespect to the people who have [a colostomy bag]. I just knew that it was not going to work for me. I didn’t want that. I wanted choices. If I had to make that choice, it was a no.
Hospital Stay
How was your hospital stay?
In the hospital, things did not go well. We thought that I had an infection or a leak where the incision was and in my colon. I guess I didn’t. In the hospital, I don’t remember a ton.
He went to have an anastomosis. Putting my colon back together, filling everything around me with water to see if there were any leaks. My surgeon was convinced there were leaks. I was convinced there were no leaks. I just didn’t feel like he gave my body enough time to recover. He wanted me to sign consent to open me back up to see if there were any leaks. I refused to sign the consent form. I knew that my body just needed more time, so he sent me down for CAT scans.
I will say this, when you are throwing up and you lose control of your bowels…I was puking and throwing up at the same time, it was the most humbling experience for me. I am trying to get on the CAT scan table and crawling over after surgery. It was like doing the army crawl to get on the table to do the CAT scan. That was my lowest moment in the hospital. I really felt like things were not going to go well. I probably did have an infection and that was just the way it was going to go, because I was not going to let them open me back up. I couldn’t do it. I wasn’t strong enough. I had accepted it.
My kids were devastated, but I also knew that if I was just given a little bit more time, my body would come back a little bit. I have to trust my gut through this entire journey. Everybody’s got a lot of opinions, but I knew I didn’t want to go back under the knife. I wasn’t going to do it. It didn’t matter, life or death. I wasn’t going back under and got the CAT scan results back and there was no leak.
Leaving the hospital
I took more antibiotics and they took out the NG tube. For a couple of days, I thought they were just getting the infection out, so after my CAT scan came back normal, I said, “Get the NG tube out. I’m done with that.” It was triggering me to vomit a lot. That was the worst feeling in the world for me at that moment. Two days later, the doctor said, “If you can eat and drink a little bit, we’ll let you out of the hospital and you can go home.” That is what I did, miraculously.
I was technically only supposed to be in for 3 days and I ended up being in for 5. I was still on track because they said the most was 7 days. I really think they released me to get me out of there. I was not an easy patient to deal with. I’m stubborn. I kept telling them, “Give me more time, give me more time, and I’ll get out of here on my own accord.”
The importance of advocating for yourself
I think it’s super important to advocate for yourself. Cancer or not, you are the only person that’s in control of your own feelings and yourself. You know your body. If you know something’s not right, it’s not right. I just cannot stress that enough to people. If you think something’s not right, it’s not right. Keep looking for people until you find a physician that will listen to you. You’ll eventually get there.
I was lucky it only took me a few times, but it took me a span of 6 months to know something wasn’t right and then to be diagnosed with stage 3 colon cancer. It was unbelievable. When they diagnose you with cancer, it goes boom. I didn’t want a stage 3 diagnosis. I wanted a stage 2, but one of my lymph nodes out of 32 came back positive for cancer cells.
I think it’s super important to advocate for yourself. Cancer or not.
Just keep pushing. Push for yourself. After I was released from the hospital, I had some time to look for an oncologist. Unfortunately, I live in an area where there’s not a lot. There’s not a lot that specialize in colon cancer. I was determined to find at least 3 different people so I could figure out what the best course of action was for me. I don’t follow everybody else’s rules. I don’t. I do what I want when I want to. I’m extremely independent and stubborn, and it’s not a one size fits all.
What did doctors recommend next for treatment?
I wasn’t a candidate for radiation. The first oncologist that I saw was actually pretty fantastic. He recommended chemo 6 times over a 3 month period, but he was more nonchalant about it. Do it or don’t do it. It didn’t really matter to him. I wasn’t comfortable with chemo at first and I said I’d get back to him.
I went to my second opinion, which was the University of Iowa Cancer Care Clinic in Iowa City, and I met with an amazing doctor, Naomi Fei, and she sat me down and said, “You need to do chemo,” and also backed it up. My surgeon was really hell bent on me doing chemo as well because I said, “I don’t think I’m going to do it.” He said, “If it were my mother, daughter, sister, or family member, I would want them to do chemo.” My second opinion at Iowa City said that it’s like an insurance policy. It’s preventative care.
My surgeon got all the cancer. It had not metastasized to any of my other organs, thank God, for as long as they think that I had it. She recommended 12 rounds of chemo for 6 months. I didn’t want to hear that. I had told my children – like I said, they are adults – that if my scans were clear and it had not metastasized and my bloodwork looked good, I was just going to live my life. They gave me maybe 5 years, and I was okay with that. I just turned 50, I could do another 20, but I just wasn’t comfortable with the chemo.
Chemotherapy
Did you decide to still do chemo?
I came home from Iowa City. I had a third opinion but I canceled that appointment. I sat by myself for hours and hours. I don’t know how you guys feel about Jesus, but he talked to me. I’d already told my kids, I’m not doing it now. I’m gonna live my life, sell my house, and move to Florida. Then, this is going to sound crazy, but I made friends with my ceiling fan. When you’re down, you spend a lot of time in your bedroom. You spend a lot of time by yourself.
I had a lot of conversations with myself, took a lot of funny notes in the middle of the night when I couldn’t sleep. I decided, plot twist, that I would do 12 rounds of chemo for 6 months. I just finished up with my second round a couple of weeks ago. I called my kids and I said, “I will do chemo. I will get through as much of it as I can.”
It still didn’t register with me that I had cancer up until just a few weeks ago. I hadn’t processed it yet. I didn’t feel sorry for myself. I’ve yet to really cry or get upset. I’m not angry. I really feel like I would be doing a disservice if I didn’t take the chance and do the chemo to live a little bit longer, because there’s many people that didn’t get the chance to do the chemo. My best friend’s husband, like I said, died of colon cancer 31 days after diagnosis. I couldn’t imagine at least trying to get more time. Of course, my kids were elated when I agreed to do the chemo.
Describe your experience with chemo
I’m going to tell you that chemo is not nice. I went in and got my port with my surgeon and I’ve seen him since then. He wants me to keep my port in longer than I expected – a few months after I get done with chemo.
Unfortunately, my third round of chemo was supposed to be last Friday, and we had to cancel because my white blood count was down by 140 points. That might have been the first time that I cried because I just wanted chemo. I just wanted to keep marking off the numbers and be done. I have no control over this, and I’m a woman that has control issues, a little bit of OCD, and a whole lot of ADHD. I’m a planner and I was devastated because my body said, “Not right now.”
Colon cancer chemo is not what people expect. I go in for my chemo and sit in an infusion chair for 4 hours. At first, it was a little terrifying. It’s really just sitting still for 3 or 4 hours. I didn’t like that at all. Being hooked up and watching the poison drain into my body, I didn’t like it. I’ve acclimated and I’ve had 2 treatments. I go in and infuse for 4 hours and then I have to go home with a chemo pump bag for 46 more hours.
When I tell people that they don’t really get it, I didn’t either. It’s for this certain type of cancer. You go home, you pump for 46 hours, and then you disconnect. We’ve decided to disconnect the needle from the port at home, which is going very well.
Have you had side effects on chemo?
The side effects of chemo…I might as well be pregnant. I’m very sensitive to smells and things anyway. With the chemo, I probably threw up at least 25 times, but I also don’t like to take my meds. I’m not a pill taker. I’m a self-care, “I’ll just deal with it.” Even if I’m sick, I just want to deal with it and mask it. Chemo had other plans for me. We tried to mask the nauseous feeling as much as we could.
The first treatment didn’t go well. The second treatment, I did do all of my meds, but I still probably vomited about 10 times. My energy level was hard for me to get back to normal. I pump for 3 days and then I have 4 days of feeling miserable. It’s really one week of total hell. I start to get better the next week, but it’s every 2 weeks. By the time I get to the good stuff, I have to go back into the chemo chair.
Like I said, my third infusion was canceled and I go back in for blood work on Tuesday. Hopefully I’ll be back in the chemo chair on Wednesday. People are like, “You’re the only person that cried because they couldn’t get their chemo,” but I just want to be done with it. There’s a lot more to do.
Reflections
Has cancer changed your outlook on life?
I’ve always had a different outlook on life. I felt like, prior to the cancer diagnosis, you really don’t know how much time you have left, you don’t know what’s coming. You don’t know what’s in store for you. I lived my life like that prior to cancer, but now my friends call me a little unhinged. I know I can’t just say I see things differently, but I literally see things differently. The colors to me are brighter. I don’t quite understand that. The sky is blue, the grass is greener, the snow is whiter. I just see things differently.
Happier? I can’t say that I’m happier with the cancer diagnosis, but I really think that God was trying to slow me down a notch, because I’m a workaholic. I own two businesses, gymnastics and flipping houses. I think this was his way of saying there’s more to life than just work. You need to calm down, and I have. I’m definitely unhinged. The hardest part about this cancer diagnosis is people telling me how I’m supposed to feel. That is extremely difficult for me.
I look at people differently. It’s not that my healthy friends are wasting their life by any means…But I’m not tired. Maybe during my chemo weeks, I’m tired and I take a few naps here and there, but if I’ve got some good time…Like yesterday, I painted the kitchen with my daughter. We just go get things done. There’s no excuses. Cancer or no cancer, you’ve got a life to live. Doesn’t matter how long it is. Go do it, people. Just go do it.
Do you have any advice for someone on their cancer journey?
My best advice would be, no regrets. If you’ve got things to say to people, say them. If you’ve got things to do, do them. Everybody always waits like they do have more time, and we don’t. Cancer or no cancer, like I said, go and live your best life.
Be selfish. I’m not a selfish person. I’m very empathetic. I do a lot of things for other people. I have my whole life, and now I’m like, if I don’t want to do it, I’m not going to do it. It’s okay to put yourself first, and that’s a lesson that took me a really long time to figure out. Without cancer, I don’t think I would have got that. I think I would have continued to do things for people, but I have to take care of myself. Saying no to doing things is so much easier than it was before.
Cancer or no cancer, you’ve got life to live.
With that being said, travel, take trips, don’t hesitate, and love people. Love yourself, love your family, and let go of some of the stupid shit that doesn’t matter anymore.
Updated October 9, 2023. Originally broadcast September 20, 2023.
Quality of life and precision are top of mind for chronic lymphocytic leukemia (CLL) patients. Understanding the complexities of available treatments can help you optimize your CLL care and prioritize the questions to ask your doctor.
During this live conversation, panelists Dr. M. Yair Levy, director of hematologic malignancies research at Texas Oncology, and Dr. Catherine Coombs, a hematologist oncologist at UCI Health who specializes in CLL, discussed the latest in CLL care. The discussion was hosted by CLL patients, advocates, and administrators of the CLL Support Facebook group Michele-Nadeem Baker and Jeff Folloder.
This discussion covers the current landscape of CLL treatment and care options, as well as new CLL treatments awaiting FDA approval, factors doctors consider when starting or switching a patient’s treatment, encouragement for CLL patients to advocate for themselves, and each doctor’s outlook on CLL treatment and patient quality of life.
There is hope. Hope to live a normal life, and hope to see your kids and your grandkids grow up. There’s always hope on the horizon, in my opinion.
Dr. Catherine Coombs
Thank you to AbbVie and BeiGene for their support of our patient education program! The Patient Story retains full editorial control over all content.
This interview has been edited for clarity and length. This is not medical advice. Please consult with your healthcare provider for treatment decisions.
Michele-Nadeem Baker: I’m Michele-Nadeem Baker. I’m a medical and health journalist, but in addition to that, I am also a patient. I started advocating for other patients on my first day of treatment when I realized that there was so much unknown out there and to demystify things for my fellow patients and help them through their journey.
Jeff Folloder: My name is Jeff Folloder. I am a passionate patient advocate. I am now in year 14 of my little journey with CLL and I am living a great life. That’s why I became a patient advocate because I want to make sure that everyone knows that it is possible to live a great life with CLL.
First up, I get to introduce Dr. Catherine Coombs. She is a hematologist oncologist with UCI Health and she specializes in chronic lymphocytic leukemia. She also helps lead clinical trials, trying to find better ways to treat CLL. Dr. Coombs, tell me what drew you to specializing in CLL. We don’t hear that a lot.
Dr. Catherine Coombs: It was a long road. I went into medical school knowing I wanted to be a cancer doctor. I didn’t have any doctors in my family, but I do have a lot of family members with cancer. It always inspired me to be on the patient end of the oncologic relationship. That’s always what I thought I would do.
Now, I didn’t decide on CLL until my residency years. I looked for a research project right away, because that’s the only way to get into a good fellowship program is by doing research. It always was something I wanted to do regardless. I found a wonderful mentor in my time at Duke University as a resident, Mark Llaneza, where I focused on the underlying genetic risk of CLL as my residency project. That drew me to the field right away.
Then I saw all these other benefits of being a CLL-focused clinician, which is that the patients do really well and they live a long time. I love having that long-term relationship with my patients. I love blood cancers in general, but I would say the acute leukemias, which I had focused on a bit earlier on in my time as a faculty when I was doing a bit of both were hard because there are a lot of patients that we lose and I really admire the docs that do it. But I think for my long-term well-being, I know that it’s just so much more gratifying and less emotionally traumatic to be able to have patients that thrive for so many years and be able to really enjoy those relationships as the added benefit.
The therapeutics have just continued to improve over the 13 years since I first graduated medical school and started doing research.
Michele: We need more doctors like you. Dr. Coombs, thank you so much. I’d also like to introduce Dr. Levy, who is a hematologist oncologist at Texas Oncology. He is the director of Hematologic Malignancies Research and specializes in CLL. He’s also helped lead clinical trials in CLL. Dr. Levy, what drew you to CLL?
Dr. Yair Levy: Before moving to Texas, I actually did mostly chronic lymphocytic leukemia, but I’m a little older than Dr. Coombs. So back when I was doing it, it was still a relatively better outcome for this cancer, but we still lost some folks to chronic lymphocytic leukemia. However, if I reflect on my current experience, I don’t believe that I have lost a patient to chronic lymphocytic leukemia in the past decade. This is not because I have a shortage of patients. I’ve probably accumulated about 150. I’m not saying that the patients don’t die, but they don’t die of CLL.
So to live a normal life is the goal. Even though we still think of CLL as a treatable but incurable malignancy, for the most part, people are doing relatively well. Not to mention, not only are our treatments better in terms of efficacy, but they’re so much better tolerated.
If I reflect on my current experience, I don’t believe that I have lost a patient to chronic lymphocytic leukemia in the past decade. This is not because I have a shortage of patients. I’ve probably accumulated about 150. I’m not saying that the patients don’t die, but they don’t die of CLL.
Dr. Yair Levy
Jeff: We have an interesting topic for today’s program, Shared Treatment Decision Making: How To Be An Empowered Patient. This is something that strikes me right in my heart. I am a firm believer that patients who take an active role in their own care tend to have better outcomes, and this is actually borne out of clinical research.
I took an active role in my own care. I chose not to go in the specific direction that my first doctor wanted to go in, and I wound up at a large research hospital participating in a clinical trial. I’ve been living a great life as a result.
Michele: For me, treatment decision-making also came down to becoming an empowered patient and becoming health literate in CLL. The more I could learn from credible sources, for me, was better. I realized all patients are different and doctors, you can probably relate to this more than anyone but the world has changed quickly and pretty drastically for clinicians, researchers, and those of us who are patients.
I was diagnosed 11 years ago, not quite as long ago as Jeff, but still a long time ago. My frontline treatment started in 2015 and things were even different back then. I was on a trial that combined ibrutinib, which at the time was not approved yet for frontline treatment. It had been for relapsed and refractory but not frontline treatment. It was combined with FCR, the standard at the time, fludarabine, cyclophosphamide, and rituximab. Things have changed so quickly even since then. In my frontline treatment, I’m now on a different treatment. I had relapsed in between.
Dr. Coombs, could you tell us how the landscape of treatments for patients has vastly changed over the last couple of years?
BTK Inhibitors
Dr. Catherine Coombs: Over the past decade, but even over the past few years, we’re seeing advances. When I first got into the field, yes, it was chemoimmunotherapy for patients fit enough to receive it like FCR and BR. With the introduction of targeted agents, largely chemoimmunotherapy is not widely used. However, we still do see about a third of uptake looking at these large-scale studies across the country.
I’d say that doctors who are focused on CLL realize that chemoimmunotherapy is not worth the toxicity. Its efficacy is also inferior to these novel drugs that are more efficacious, so more likely to put the CLL at bay, in remission, and delay time until ultimate progression, but also hugely safer. That was first ibrutinib, as you wisely know from your own personal experience and your knowledge over the time of your journey as a patient. But now we have a lot of newer and better drugs. Ibrutinib has been amazing and revolutionary, but it does have some side effects. Fortunately, they’re not so common, but they still can be clinically significant.
The first category of drugs that have really changed in the past few years is newer generation BTK inhibitors. Ibrutinib was the first in class. It inhibits this critical protein that’s part of CLL cell machinery, BTK, but it’s not totally selective for its target. We now have 2 additional drugs that inhibit BTK – acalabrutinib and the most recent addition, zanubrutinib which was FDA-approved in January.
The advantage of both of these drugs is that they’re more selective for their target, BTK. That, fortunately, has translated to improved safety, where both drugs have been compared head to head with ibrutinib and they demonstrate improved tolerability, specifically lower rates of atrial fibrillation for both drugs. Acalabrutinib also has the advantage of lower rates of hypertension.
What we don’t know is whether zanubrutinib is better than acalabrutinib or acalabrutinib is better than zanubrutinib, because we don’t have that comparison. But I think they’re both excellent options and both offer advantages over the ibrutinib days when we were dealing with a lot of atrial fibrillation. There’s a lot less in the way of that.
The other huge class of drugs that I haven’t mentioned is a completely different way of treating CLL, so I’ll mention it briefly. I don’t know if we’re going to get more into the nitty gritty on this, but these BTK inhibitors work wonderfully at controlling CLL, but they’re considered as treat-to-progression regimens, meaning that patients go on and stay on as long as they’re, number one, tolerating it and their CLL is responding favorably.
Some patients don’t like the idea of being on a drug indefinitely, so the other huge therapeutic advance over the past few years that’s been widely available is the drug venetoclax. This is typically combined with another drug called obinutuzumab when used in the frontline setting. Because it can so effectively kill off the CLL to very deep levels, patients are able to completely stop treatment after one year and then eventually relapse, but it can take a long time. That’s one of the other major, major changes in CLL just over these past 5 years or so.
I’d say that doctors who are focused on CLL realize that chemoimmunotherapy is not worth the toxicity. Its efficacy is also inferior to these novel drugs that are more efficacious, so more likely to put the CLL at bay, in remission, and delay time until ultimate progression, but also hugely safer.
Dr. Catherine Coombs
Michele: Dr. Levy, what else would you add?
Dr. Yair Levy: Dr. Coombs, you hit the nail on the head. It’s a dramatic change from chemoimmunotherapy. In the chemoimmunotherapy era, our high unmet need was what we considered high risk which were ones that harbor a 17p deletion, or a mutation in this TP53 tumor suppressor protein, or these cells of origin that are called pre-germinal cells of origin. So a more immature cell that had gone bad, and we’ve known that they have done historically quite poorly with chemoimmunotherapy.
As Dr. Coombs mentioned, the biggest improvement that we saw was when we actually recognized druggable targets within the B-cell receptor pathway. The first such drugs were actually not Bruton’s tyrosine kinase (BTK) inhibitors, and they are largely relegated to the history of the B-cell receptor pathway now. But these were the PI3K delta inhibitors. Those worked irrespective of cell of origin, and they also worked in the 17p deletion. So again, they did certainly have some tolerability issues and the efficacy was not comparable to those of Bruton’s tyrosine kinase inhibitors, which is one of the big reasons that those have really fallen out of favor.
As Dr. Coombs mentioned, the BCL2 inhibitor venetoclax has also been a game changer. We’ve been utilizing these agents, either alone or in combination with CD20 monoclonal antibodies. Now, the European Medical Association has even approved the combination of a BCL2 and a BTKi. This is something that we’re doing further studies on within the United States as well because we’re seeing that people achieve very impressively high rates of response. More importantly, very deep responses can allow, hopefully, a very long treatment-free interval, and perhaps even in some cases, a functional cure.
So, in the beginning, we were saying that CLL is largely treatable but incurable, but we put an asterisk on that. Even with chemoimmunotherapy, there was a subset of CLL that may have been cured by chemoimmunotherapy, or at least a functional cure. I think we’re going to see the same thing with these other combinations as well.
We’re seeing that people achieve very impressively high rates of response. More importantly, very deep responses that can allow, hopefully, a very long treatment-free interval, and perhaps even in some cases, a functional cure.
Dr. Yair Levy
How CLL doctors are providing CLL patients with precision care
Jeff: This is exciting stuff. We’re talking about an awful lot of options for patients, but before we can get to those options, we need to figure out how we get to that point. So let’s chat a little bit about the tests that are needed to diagnose and then accurately inform those potential treatments.
A lot of us in the support groups and on social media love tossing around the cute names, the FISH test, the flow test. Not a lot of people truly understand what’s going on with those tests. They don’t understand the concept of chromosomal abnormalities that may be going on with a patient at the time of diagnosis. Dr. Coombs, can you briefly give us a top line as to what these tests are doing and more importantly, what they’re telling you in terms of prognostics?
Dr. Catherine Coombs: Absolutely. Before the advent of all these, let’s call them sophisticated tests, we would stage patients. That’s always what I think cancer patients think of, what stage am I? We do have a staging system called the Rai Staging System that we use in the US. In Europe, they use this Binet Staging System. But the idea is, how much is this really affecting me? Rai stage 0 is when it’s just a high white count to Rai stage 4 when you have low platelets from the CLL.
I’m taking a step back because there were, for decades, ways of saying this a good or a bad CLL. However, what we’ve learned over the years is that there are some patients with really early-stage disease that would follow very aggressive clinical courses and then some that may have been technically a Rai stage 4 that were totally stable for decades. The goal with all these more sophisticated tests was to better predict, how is this person’s CLL going to behave, which then helps us as clinicians know what to expect. It helps the patient as far as what he or she should expect.
So taking a step back, we now have a lot of advanced testing that we can send. The good news is that these can be sent on the peripheral blood so it’s not necessary to get a bone marrow biopsy early on. Of course, we do consider these at the time of therapy, but we can send these tests in the blood because the CLL, by its nature, is circulating in the blood. So we can pick up different abnormalities that can tell us, this is a good or a bad CLL or maybe somewhere in the middle to help us, number one, know if we should follow this person more closely. Number two, is this someone that perhaps it’s less likely to cause more trouble than not?
The categories of tests are looking at the DNA, which is either via a FISH test which uses fluorescent probes to find common abnormalities that are known to be seen in CLL. The most adverse is the 17p deletion. On the other spectrum, the most favorable is an isolated 13a deletion.
However, what we’ve learned is that this is only looking at certain probes. Sometimes you can have other abnormalities that aren’t present as part of the FISH panel. In my own practice, I also send a karyotype test which looks for the same thing, abnormal chromosomes. Instead of using a preselected panel of common abnormalities in CLL, it just looks at all the chromosomes. The chromosomes, just for the patient’s knowledge, are just the big chunks of DNA that live inside every one of our cells. We’re focusing on what these abnormalities are in the cells because there are common patterns. There are good patterns and bad patterns.
It’s also bad to have a complex karyotype, meaning 3 or more abnormalities in any given cell, so that’s one category. The 17p deletion I mentioned is known to behave more aggressively. It’s still a chronic disease, but those are often the bad actors, especially back in the chemo days when chemo doesn’t work well at all. It does do better with our new drugs, but that is a particular problem because it deletes a copy of this very important gene called TP53.
We used to think the only way of losing that gene was by completely deleting the part of the chromosome where it’s contained. What has been learned over the past 10 to 15 years now in CLL, is that it may not be deleted, but it could be mutated. That’s another test that I think is very wise to send, especially in patients who are going to need treatment because a TP53 mutation is largely the same as a 17p deletion. There are a little bit of nuances there, but these are 2 separate tests. They both give similar information because those 2 abnormalities are treated as one and the same as far as their impact on prognosis.
The next category of testing is looking at the immunoglobulin heavy chain status, so a normal B-cell over its life. CLL is a cancer of B-cells that undergoes a process of somatic hypermutation where it just acquires mutations. It’s actually good to have a mutated, immunoglobulin-heavy chain. The bad finding is for that to be unmutated, which suggests this is a bit more primitive of a cell. And what’s been borne out through a lot of studies is that patients with unmutated are the ones who need therapy quicker and they don’t respond as well to certain therapies. Now, again, the negative predictive impact of some of these abnormalities is somewhat outdated. Sometimes they do just as well with our new treatments, but they definitely don’t do as well with the old treatments.
The other test I always send is the beta-2 microglobulin (B2M), mainly because that goes into our scoring system for CLL, the CLL International Prognostic Index, but it’s an adverse finding to have that elevated. I think that wraps up the bulk of all the prognostic tests that I send at the time of meeting a new patient and trying to help understand what is our future going to be like.
The goal with all these more sophisticated tests was to better predict, how is this person’s CLL going to behave, which then helps us as clinicians know what to expect. It helps the patient as far as what he or she should expect.
Dr. Catherine Coombs
Jeff: Let me play that back for just a second and put it in terms that are not quite so technical. You have a toolbox, and that toolbox has a lot of really nifty tools in it, where instead of saying you have leukemia or you have chronic lymphocytic leukemia or you have one of these genetic abnormalities, you’re able to hone down to a very precise level of differentiation. That’s where the term personal and precision care comes in. Correct?
Dr. Catherine Coombs: Excellent explanation. Yes.
Michele-Nadeem Baker: I love this term and how that is happening more and more for patients. Dr. Levy, before planning treatment, what do you like to understand from your patients so that you can learn more about them when it comes to prescribing their treatment?
We need to speak with the patient and find out what is most important to them and explain everything about the treatment, including side effects, logistics, expected outcomes if you choose one route versus another, and the cost of travel. There are a lot of things that go into everything.
Dr. Yair Levy
Dr. Yair Levy: We’re all different and everybody’s cancer is also different. The reason that we have jobs as oncologists is because, I’m not sure that’s true here, but hopefully we know more about CLL and the treatment options than the patients. It’s our job to explain to them all their various options and then help them arrive at a choice that makes the most sense for them.
I think Dr. Coombs mentioned that we have a lot of options, but they haven’t necessarily been compared head to head. So we can’t tell you prospectively how treatment A compares to treatment B or treatment C. There are certain guidelines of what’s called preferred therapies and other alternative therapies that are also acceptable. We need to speak with the patient and find out what is most important to them and explain everything about the treatment, including side effects, logistics, expected outcomes if you choose one route versus another, and the cost of travel. There are a lot of things that go into everything. This is our job to get them to ask the right questions and then answer those questions.
The role of patient comorbidities in CLL care
Michele: And what about comorbidities? Is it important for patients to discuss their other health issues with you, such as cardiac issues? There’s a myriad of so many other types.
Dr. Yair Levy: Absolutely. This is what we were saying is, we’re all different, we all have different things that matter, and we are all in a different place in our lives. We take all of that into consideration, there’s no question about it.
The comorbidities are incredibly important, but we certainly advanced past where we were 15 or 20 years ago when we were looking at whether patients are fit enough to take therapy versus not because right now we’re not necessarily looking at fitness for therapy as much as we’re looking at what is the optimal therapy for them.
Many of the therapies that we have, if you take a look at what’s called the Preferred Category 1 recommendations from the NCCN Panel, were all studied in what we would have technically called a non-fit population before. It’s wonderful that we have all these highly effective therapies that we can give to people, even if their fitness is not optimal.
The benefits of watch and wait
Jeff: We’ve been talking about a whole bunch of novel therapies, stuff that has really impressive outcomes these days. Michele and I will both be able to tell you without hesitation, that the first thing that most patients encounter is not treatment. It’s this thing that we call watch and worry. You guys call it watch and wait. CLL does not always need to be treated right away. Your medical team is going to work with you to decide when it’s best to start treatment. In the meantime, the patient’s worry. Did I sum that up correctly, Michele?
Michele: We sure do, even though we tell everyone not to and to take a breath when they’re first diagnosed. Jeff, you and I both know that we still go through that when we’re back in that time period. It’s just so counterintuitive to not be treated right away when the disease has not progressed where it ends up going when you do get treated.
Dr. Coombs, what are you looking for when it’s time to treat? You go through years, hopefully, during watch and wait. Worry and wait, as patients call it. But what is it that you’re looking for and is there any benefit to treating it sooner as with some of the other cancers out there?
Dr. Catherine Coombs: I’m coming straight from my clinic. I’m in a clinic room. I just had this conversation with a patient who is newly diagnosed about watchful waiting, which I totally understand why it’s watchful worrying for many. I always see it as my duty to help them understand why this is our approach. I acknowledge this is not what we do for many other cancers where you hear, find it early, treat it early. I wish our treatments were so good that treating it early would knock it out and you’d never have to worry about it again. In 2023, we haven’t been smart enough to come up with something that will do that for CLL.
The way that I help put that in context for my patients is this disease can be so indolent that maybe up to 1 in 3 patients never need treatment in their lifetime. So if we treated everyone, inherently we’re over-treating people. I hate giving people things they don’t need because every treatment comes with a cost, whether it’s financial or side effects. That’s my one very strong argument for not over-treating. But also, none of the early treatments that we have tried and done clinical trials on have been shown to make patients live any longer. That is just where we are.
I definitely could understand the frustration on the part of patients because that leaves you with these worries. I do see those getting better in patients as time goes on. There’s this initial period of uncertainty, but then as you see what your pattern is, that either tells us, maybe we are approaching the time for therapy or nothing’s really changing, I feel fine, and this is something I can accept.
Now, obviously, we never know which camp a patient is going to fall into in these prognostic tests. They help us have a general sense of, maybe this will be a super slow CLL versus one that progresses more rapidly, but nothing is certain. I do personally have enthusiasm for making this change.
There is an ongoing countrywide clinical trial looking at early intervention for patients with high risk. That is open at my own institution and across many, many institutions in the country. I really hope things will change so we can improve patients with early disease. I don’t think it’s going to be every patient because of this third that never needs treatment. I don’t ever see a reason to just treat everyone, but the trial specifically is focusing on high-risk patients. Maybe there will be some movement there. It’ll probably take about 10 years to find the results of the study because you have to follow patients for a really long time.
For now, my job is to not over-treat and not make people who are feeling good feel worse. If you’re asymptomatic, then the best I can do is leave you alone, but hopefully calm some of whatever natural anxieties come about with what is a life-changing diagnosis.
This disease can be so indolent that maybe up to 1 in 3 patients never need treatment in their lifetime. So if we treated everyone, inherently we’re over-treating people.
Dr. Catherine Coombs
Michele: We have some questions coming in from our audience. Dr. Levy, here’s one of the questions for those of us with liver enlargement. Should we watch and wait?
Dr. Yair Levy: I completely understand the anxiety that comes along with this. I’ve been treating indolent lymphomas for a couple of decades now, and I’ve got the same experience. You talk with patients, you tell them they have cancer, and then they’re saying, “You tell me I have cancer, but you’re not going to treat me now. Are you sure you went to medical school?” I had that come up several times.
By the way, we don’t do watchful waiting anymore. We call it active surveillance. Nobody likes watchful waiting, but if we’re saying we’re actively surveilling you, that sounds certainly a lot better.
The way that I explain it is, that there are really only two good reasons to treat you for anything. This isn’t just an oncologist, it’s in all of medicine. My wife is a real doctor, she’s an internist. She has the same parameters for treatment. So, number one, if you can make somebody feel better, that’s absolutely a great reason to treat them. Number two, if you can make them live longer.
What we’ve seen, as Dr. Coombs was saying in chronic lymphocytic leukemia, as well as a variety of other indolent non-Hodgkin’s lymphomas is that early treatment does not confer a benefit in survival. In other words, if we treat you when you’re asymptomatic, you’re not going to live any longer than if we wait to treat you when you are symptomatic. This is important because as we were talking before, our treatments are changing and changing for the better.
The treatments are becoming more effective and better tolerated. And remember, something is only incurable until we’re able to cure it. So there are a lot of good reasons to wait. Dr. Coombs mentioned this as well. If I can’t make you live longer by treating you earlier with our current therapeutics, the question is, can I make you feel better? If you’re asymptomatic, I can’t make you feel better. I can make you feel worse. I can spend a lot of your money, but I’m not helping you. You are the most important part of that equation.
If somebody has liver enlargement, the question is, are they symptomatic? Are they having pain? Are they having any other symptoms from their liver involvement? If they’re asymptomatic, I would not necessarily treat them just for liver enlargement. The same thing is true with spleen enlargement as well, which is a far more common finding in chronic lymphocytic leukemia.
If we treat you when you’re asymptomatic, you’re not going to live any longer than if we wait to treat you when you are symptomatic.
Dr. Yair Levy
Michele: I experienced that when I relapsed, but along with other things as well, which led to my going back into treatment. Dr. Levy, thank you. You brought up a lot of great reasons why people are not rushed into treatment which also hints at all the things that you do look at when it is time for treatment, which we’ll continue to talk about as we go through with our program today. Thank you very much.
Considering the duration of treatment for CLL patients
Jeff: We spoke earlier about a bunch of the newer options that are available. We know that the treatment landscape is changing by the minute. I’m going to tee this up in terms that forum participants and our support group participants, they all had the same questions.
Yeah, the drugs are great. Am I going to have to take them for the rest of my life, or is there a chance that I can do it for a fixed duration? Dr. Levy, let’s break down what those current treatments are, what baskets they fall into and is this a lifetime activity or could we end it in 6 months? Could we end it in one year? You’ve got a lot of stuff that ends in -ibs, and -tas, and -mabs, and all that. Explain to us what’s going on.
Dr. Yair Levy: Again, this treatment progression model is a relatively new phenomenon for us in the treatment of malignancies. We used to treat with a fixed duration of therapy when all we had was chemoimmunotherapy. You can understand why. Once we give chemo, we can’t take it back. Certainly, the effects of cytotoxic chemotherapy are not something that you want in a cumulative manner.
Because of the logistics of how cytotoxic chemotherapy works, we could not give that till progression because that would be a very difficult life. Everybody thinks that the worst thing in the world is dying, and no, the worst thing in the world is not dying. The worst thing is a long, crappy life. That’s what we would assure we would do to people if we continued them on chemoimmunotherapy.
If you take a look at our approved therapies right now, basically it’s two categories. Bruton’s tyrosine kinase inhibition, BCL2 inhibitors, and monoclonal antibodies, can be sprinkled on any of these regimens. In terms of approved fixed durations of therapy, it’s only with the BCL2 inhibitors. The reason for that is that’s the most ideal drug that we have seen in the treatment of chronic lymphocytic leukemia. What I mean by that is it is a killing machine. It kills so well that we had to attenuate the dose because if you kill things too quickly, that can also become a problem.
We’re able to get those very, very deep responses. These deep responses, even if they’re what’s called MRD, which stands for minimal residual disease, really should be measurable residual disease. Even if people achieve a level of disease below where we can measure it, we know that in many cases it still returns. We really need to get that logarithmic killing. We really need to reduce their tumor burden by many zeroes in order to give them that long treatment-free interval. Currently, that’s possibly more likely with a BCL2 inhibitor venetoclax.
As we were alluding to before, we are seeing combinations of Bruton’s tyrosine kinase inhibitors like ibrutinib, acalabrutinib, or zanubrutinib in combination with venetoclax. Again, this was based on these laboratory models in which they actually saw whether or not these cells were primed for death with this combination. They actually saw synergy, meaning that the drugs worked better together than the sum of their parts.
As we mentioned, this is a fixed duration of therapy that’s actually approved in Europe right now, but not here in the United States. In the United States, we certainly can give a fixed duration of therapy with venetoclax and a CD20 monoclonal antibody. I can tell you that anecdotally, I’ve also done that with Bruton’s tyrosine kinase inhibitor and a monoclonal antibody if I can achieve that very deep response.
In terms of approved fixed durations of therapy, it’s only with the BCL2 inhibitors. The reason for that is that’s the most cidal drug that we have seen in the treatment of chronic lymphocytic leukemia.
Dr. Yair Levy
Factors in choosing a first-line treatment for CLL
Jeff: Excellent. Lonnie’s got a great question. Since we’re now considering treatments, he wants to know what are the primary factors to consider in choosing a first-line treatment. Dr. Coombs How do doctors and patients make that call? How do you choose which drugs are up on deck first?
Dr. Catherine Coombs: I think there are disease-related factors and patient-specific factors. We tackle those one at a time. I think there is an important role in knowing what an individual’s CLL risk findings are because those can help inform how likely a treatment is to lead to prolonged remission. Specific to a venetoclax-based approach in the front line, what we do know is that there are shorter remissions in patients with the 17p deletion or TP53 mutation and also shorter remissions for individuals with unmutated IGHV.
I tend to be an optimist and so my view is that these therapies, venetoclax-based, work way better than chemotherapy ever did for patients with these high-risk features. We can still see lengthy remissions on the order of a little over 4 years for the 17p patients for progression-free survival or around 5 some years for the unmutated IGHV. That is shorter than if you don’t have those markers.
I do think it helps weigh expectations on what to expect from a time-limited regimen. If you have high-risk markers, if you have all favorable markers, venetoclax also works really well and it just works longer than if you had negative markers.
Now, Bruton’s tyrosine kinase inhibitors as a class that have really leveled the playing field. If we divvy up patients with the unmutated and the mutated IGHV and the chemo days, the unmutated would relapse years faster than the mutated. There’s not much of a difference, and so those drugs work really for everyone. Now, they’re just so different conceptually and side effect-wise, which is why it is so important to weigh the patient’s comorbidities.
In addition to these disease-related factors that could help gauge the relative success of any given therapeutic approach, there are patient-specific factors. That’s why it’s so important for me to know, not only the details of the CLL but also the details of your specific comorbidities. Do you have a high degree of cardiac comorbidities where maybe we might be a little bit nervous about the BTK inhibitors, which can have cardiac side effects?
I will say the newer drugs are much better than ibrutinib, but it is something I weigh whether you have significant kidney disease, which might be a little bit risky. When we think of a drug like venetoclax that causes tumor lysis syndrome – none of these are complete no-goes, but they help tip the scale of which one are we favoring a bit more.
Then, of course, I want to know what other medications you’re taking, because a lot of medications can interact. That’s something we have to make sure of. Often that’s not a big deal, we just switch one out, but we have to know.
Lastly is social factors. What are your preferences? Are you the type of person who wants to do everything and doesn’t mind a frequent schedule, but wants that payoff of then being done with treatment in a year, where we might lean more towards venetoclax-obinutuzumab? Or are you someone who wants to spend as little time at a doctor’s office as possible and is okay with indefinite treatment where we may lean more towards BTKi? Those are the 3 major categories I think of – disease factors, patient comorbidity, specific factors, and then social and preference.
My view is that these therapies, venetoclax-based, work way better than chemotherapy ever did for patients with these high-risk features.
Dr. Catherine Coombs
The benefits of monoclonal antibodies for some CLL patients
Michele: Dr. Coombs, thank you for talking about the biomarkers that might indicate someone is a high risk, such as 17p or TP53. I am high-risk, but I don’t have either of those. I have the other that you had discussed being unmutated IGHV, and that actually impacted my treatment decision when I relapsed. I just finished. I am on acalabrutinib and was on a blinatumomab until a couple of weeks ago. It was obinutuzumab for 6 months along with the acalabrutinib.
Now, I will be staying on acalabrutinib indefinitely because I am considered high-risk. I had originally stated before that I started on ibrutinib. BTK inhibitors work for me and I just had adverse events initially and that’s why I went off. I had a couple of years of a drug holiday and then my doctor decided that while BTK inhibitors were still working, let’s go for it. I would still have another option with venetoclax.
Dr. Levy, why does a monoclonal antibody help? What does it add to the one-two punch? I know you talked about the different things that they’re addressing and being a killing machine, but why is it only for some patients? For example, what I’m on, acalabrutinib and obinutuzumab trials have shown that it specifically works the best. One trial was presented at ASH this past year for people like me who were unmutated. So, why only for some patients is it a benefit?
Dr. Yair Levy: Well, that’s a great question. The CD20 monoclonals were our first immunotherapy in the treatment of many B-cell malignancies. When we combined them with some of the targeted therapies, we didn’t necessarily see what we were expecting. In all of the trials with chemoimmunotherapy, adding a CD20 monoclonal improved progression-free survival. But interestingly, when we took a look at some of the studies that had arms that contained both ibrutinib, our first, covalent Bruton’s tyrosine kinase inhibitor in combination with a CD20 monoclonal or without those progression-free survival curves were superimposable. I think we were really surprised by that.
By the way, I need a button that says “I agree with Dr. Coombs.” Dr. Coombs was actually mentioning the fact that there are differences among these covalent Bruton’s tyrosine kinase inhibitors, and our first one had a less focused kinase profile. In other words, it hit other kinases, not just Bruton’s tyrosine kinase that we were trying to inhibit. One of the other kinases that it inhibited was something called ITK or IL-2-inducible tyrosine kinase. This led to antagonism of the CD20 monoclonal, which is why we got no benefit from the addition of the CD20 monoclonal.
This is not true for the other covalent BTKi, zanubrutinib and acalabrutinib. However, you’re seeing the combination with acala because that is FDA-approved and zanubrutinib does not have an FDA label in combination with a CD20 monoclonal. Do I have any reason to think that it wouldn’t work as well? I do not. There’s certainly data that supports that as well, that there are differences in terms of PFS for folks receiving the combination of zanubrutinib with a CD20 as well as without.
Now you can say, so why doesn’t everybody get a CD20 monoclonal? The answer is that there are trade-offs. Everything in life is a risk-benefit ratio. We know that, for example, there is this virus here in Texas, I don’t know if you guys have it too, called COVID. We know that for COVID, the CD20 monoclonal certainly antagonized an immune response to vaccination, as do the BCL2s and Bruton’s tyrosine kinase inhibitors.
Certainly, you are at more risk for adverse events and complications when you add additional drugs, so everything is a trade-off. We’re getting additional efficacy but at a cost. Our job is not to tell patients what to do. Our job is to have a discussion and come up with a solution that works best for them after we have a discussion and they are fully informed.
Now you can say, so why doesn’t everybody get a CD20 monoclonal? The answer is that there are trade-offs. Everything in life is a risk-benefit ratio.
Dr. Yair Levy
What CLL doctors consider before ramping up treatment and dosing
Michele: Thank you. Dr. Coombs, let’s talk about ramping up treatment. When you start treatments such as with venetoclax or even obinutuzumab, you start with smaller amounts and then ramp up to full dosing. Why is that?
Dr. Catherine Coombs: It’s different based on the drug. Let’s tackle obinutuzumab first. Obinutuzumab is the monoclonal antibody that can be paired with either venetoclax or acalabrutinib. It can also be used by itself less often. It’s a hugely effective drug, and it doesn’t really have that many side effects except for one that’s almost universal, which is these infusion-related reactions. Of course, it has other side effects such as impaired vaccine efficacy infections. It can cause low blood counts, but the one that’s universal is infusion-related reactions.
Instead of just giving patients their full dose of 400 mg daily, we…slowly introduce it so we’re more slowly killing off the cells in a way that’s friendly to the kidney and friendly to the rest of the body to minimize any potential risks from all this dead cancer cell debris.
Dr. Catherine Coombs
What they’ve learned over the course of developing this drug in clinical trials is that, instead of blasting patients with the full dose on the first day, the reaction seemed to be more manageable if you split the dose. The traditional way of administering obinutuzumab, the full dose is 1000 mg.
Instead of doing that all at once, which would make for a very colorful reaction in the infusion suite that no one nurse nor patient wants to be involved with is giving 100 mg on day one and then the other 900 mg on day two. Then of course you follow along with the rest of the schedule. The reactions, fortunately, are almost always on the first 1 or 2 days and then not long-lasting except for rare exceptions. That’s the reason for ramping up obinutuzumab, to make the reactions more manageable.
Venetoclax is a different story. As Dr. Levy mentioned, this drug is remarkably effective at annihilating CLL cells. But it’s not a good idea to kill any cancer just too quickly, because when you kill a cancer cell, all this dead cancer cell debris gets released into our bloodstream and our kidneys can’t handle that, even the best kidney in the world.
Instead of killing cancer rapidly by administering the full dose, it’s been learned through very well thought out and designed clinical trials that patients tolerate it better with less chance for dangerous tumor lysis syndrome, which is the term for complications from cancer dying too quickly, is to ramp it up. Instead of just giving patients their full dose of 400 mg daily, we give them a little whiff of venetoclax in week one, 20 mg, a little whiff the next week, 50 mg, and slowly introduce it so we’re more slowly killing off the cells in a way that’s friendly to the kidney and friendly to the rest of the body to minimize any potential risks from all this dead cancer cell debris.
Considering the side effects of CLL treatments
Jeff: Dr. Levy, I love the fact that you used the term risk management because that’s pretty much how I approached my entire journey, with risk management. We know that for most people there are going to be some side effects. There’s going to be some challenges when they start treatment. Can you give us a minute on, are they all going to happen upfront? And how do you manage them?
Dr. Yair Levy: That’s a great question. As Dr. Coombs mentioned, for the CD20 monoclonals, most of the reactions occur early and typically improve as you receive more of the drug. This is also true for the oral medications that we have. Most of the side effects, if you look at what’s called adjusted incidence, meaning how likely is it to happen per amount of time, it’s more likely to happen in the beginning. However, as we talked about, some of these therapies are indefinite progression or intolerance.
If you take a look at the cumulative incidence of events that continue to go up, there are certainly some events that are much more difficult to come back from. One that we worry about in particular is what’s called ventricular tachyarrhythmias, so getting a funny heart rhythm can actually lead to sudden death. It’s tough to come back from sudden death, isn’t it? One person’s done it right. They wrote a book about Him. One Person came back from the dead. A very popular book, but nobody else has done it since so we want to make sure that we give patients the safest possible therapeutics that we can.
Reasons to switch a CLL patient’s inhibitor
Jeff: Sometimes patients are told that they need to switch out their BTK inhibitor. There are a lot of reasons why this could be done. Dr. Coombs, can you tell us what’s going on with this?
Dr. Catherine Coombs: That is a common question, and that’s something that’s evolved over the years from having one option, just ibrutinib, to now having multiple options. In my own practice, I actually have switched patients for a number of reasons. I would say the reason that I consider switching a patient off of a BTK inhibitor to a different BTK inhibitor is if they’re having some side effect that’s negatively impacting their quality of life. I have switched patients from ibrutinib to acalabrutinib with very good success. I’ve also switched patients from ibrutinib to zanubrutinib, and I’ve even switched patients from acalabrutinib to zanubrutinib.
There have been studies looking at switching for side effects. About 70% of the time, the patients have improved tolerability on one of the newer drugs. There have been studies looking at switching to both acalabrutinib from ibrutinib and then switching to zanubrutinib from both ibrutinib and acalabrutinib and it seems to be a pretty uniform result where more often than not, the newer drugs are better tolerated than our oldest drug, specifically ibrutinib. I think that’s a very valid reason to switch.
The education point is, I would not switch in the setting of progression. That just is not a strategy that works more than a month or two and it isn’t really worth it. If you’re progressing on a BTK inhibitor of these FDA-approved ones, again, not speaking to switching from any of the approved ones, ibrutinib, acalabrutinib, or zanubrutinib, that is not recommended.
Now, I’ve heard of some occasional doctors just switching everyone off of ibrutinib. I’d say I talk to a lot of the community. I think most of us don’t do that because the side effects that occur most of the time are early on. I don’t use ibrutinib for my new starts, but I definitely have patients in my clinic who have been on it for years and they’re doing well. The old expression is if it ain’t broke, don’t fix it. Some people think, well, let’s just switch everyone. I don’t think that’s wrong, but it’s just not something that I’ve done for the reason I mentioned.
Jeff: Thank you for that. Makes complete sense.
I would not switch in the setting of progression. That just is not a strategy that works more than a month or two and it isn’t really worth it.
Dr. Catherine Coombs
New CLL treatments awaiting FDA approval
Michele: Doctors, there are so many types of treatment and clinical trials. Dr. Coombs, which ones are you most excited about that are getting closer to FDA approval?
Dr. Catherine Coombs: There are two that I’m going to mention. I’m excited about a lot of things, but the ones that I think are the closest to being approved potentially, I have no window into when the FDA actually approves things. One is a drug called pirtobrutinib. This is a drug that inhibits the same target as ibrutinib, acalabrutinib, zanubrutinib, and BTK, but instead of inhibiting it irreversibly, it is a reversible inhibitor.
The reason that that’s important is that when patients develop resistance to ibrutinib, acalabrutinib, and zanubrutinib, the resistance is shared by all of these drugs. So you can’t switch from acalabrutinib to zanubrutinib or ibrutinib to zanubrutinib, etc., if your patient is resistant because they develop most commonly mutations where the drugs bind. Pirtobrutinib binds at a different mechanism. It’s in a different part of the BTK molecule protein and it has shown very excellent efficacy in a very large study. I do think that that may attain FDA approval for CLL in the coming days.
It’s already FDA-approved for mantle cell lymphoma as of January, so there are ways to get it off-label, but I would much rather see it get full FDA approval to help with insurance paying for the drug when it’s needed. It fills a huge unmet need for patients who have progressed on covalent BTKis, especially after patients who have progressed following venetoclax where we don’t really have good options.
The other big category that Dr. Levy has alluded to is the combination of a BTKi plus venetoclax. Europe approved the combination of ibrutinib with venetoclax, which did not get approved in the United States. I can’t really speak about the reasons because I’m not involved with those discussions. I do wonder if some of it may be the toxicity of that regimen, which can be somewhat hard to tolerate, especially for older adults.
But what we know is that we have better BTK inhibitors with respect to tolerability. So there are a couple of trials that are looking at the combination of acalabrutinib and venetoclax that I do think hopefully will be positive trials that lead to FDA approval. That’s the other major category that I’m looking forward to. Those would be frontline treatment. You would use that combination as your first treatment. Whereas pirtobrutinib, if it gets approved, would be a relapsed treatment, at least for now. Things obviously change as time goes on.
It fills a huge unmet need for patients who have progressed on covalent BTKis, especially after patients who have progressed following venetoclax where we don’t really have good options.
Dr. Catherine Coombs
Michele: So your top two are pirtobrutinib and the combination of–.
Dr. Catherine Coombs: A BTKi plus venetoclax.
Michele-Nadeem Baker: Dr. Levy?
Dr. Yair Levy: I agree once again. There are other small molecule inhibitors, again, targeting that B-cell receptor pathway, which has really revolutionized the way that we treat a lot of these B-cell NHLs. In addition, the bispecifics, are certainly working their way into our armamentarium for non-Hodgkin’s lymphomas as well as CAR Ts.
Interestingly, one of the first articles that came out about CAR T was in chronic lymphocytic leukemia, despite the fact that our current constructs, these current autologous derived products are certainly not showing the same level of efficacy in chronic lymphocytic leukemia as they are in diffuse large B-cell lymphoma, for example. Nevertheless, I think that we are going to see some tremendous improvements in terms of the CAR Ts in chronic lymphocytic leukemia as well as the Bispecifics.
CLL doctors’ top takeaways
Jeff: So, Dr. Levy, I’m going to put you on the spot. What is the number one takeaway that patients should be grabbing from this discussion that we’re having today? What’s the top of the list?
Dr. Yair Levy: We’re doing so much better. As I mentioned at the beginning of the conversation, I have not had a patient die of CLL in the past decade. When we take a look at the high unmet need and again, Dr. Coombs was alluding to that. Folks who have progressed on a Bruton’s tyrosine kinase inhibitor and a BCL2 inhibitor are certainly the unmet need. We have a tough time finding those folks.
We’ve had some studies that have been languishing for accrual because it required folks to become double refractory. Again, we have a tough time finding those patients, which is wonderful. I don’t want to find those patients. I’ve put 2 people on in the past 5 years, and one of them was actually not even really refractory. He just wasn’t taking his medication. With CAR T, once I give it to him, he can’t take it, so this was more of me being paternalistic.
We’re doing so much better. As I mentioned at the beginning of the conversation, I have not had a patient die of CCL in the past decade.
Dr. Yair Levy
Jeff: Dr. Coombs, what is the single most important thing that you want patients and their caregivers to take away from this discussion?
Dr. Catherine Coombs: Jeff, we are friends now. It’s going to be hard to narrow down one thing, but I think if I have to say one thing, it’s there is hope. Leukemia is a horrifically scary word to hear for the first time, or maybe even after years of knowing that this is what you have. But all the treatments work extremely well and they work for an extremely long time. There is hope. Hope to live a normal life, and hope to see your kids and your grandkids grow up. There’s always hope on the horizon, in my opinion.
Encouragement for CLL patients to advocate for themselves
Jeff: What can patients and their caregivers do or ask if their local hematologist-oncologist isn’t quite looking at this new wonderful stuff that’s on the plate right now? What if they’re just going with the old stuff?
Dr. Catherine Coombs: That’s such an important question. And, you know, I think it’s tricky. I think it depends on what your personality type is. My personality is that I want to make everyone happy. I never want to offend anyone. I certainly understand the hesitation to question your doctor. But I think in the end, you just have to realize this is your life. If your doctor is not sounding up to date or if you’re just not getting your questions answered, then you deserve more than that.
I just think it’s so important to advocate for yourself or advocate for your loved ones if things aren’t adding up. I think our community docs are amazing. The ones that I interact with, I have no idea how they keep up with everything they keep up with. To put things into context, there are around 20,000 cases of CLL diagnosed a year.
When you think about the common cancers that have a majority of patients, they’re seeing lung cancer, breast cancer – those are like 200,000 plus cases. CLL ends up just being a much smaller slice of what they’re seeing every day, and it’s just very hard to keep up. I would say most community docs I work with very much welcome the second opinion because I can teach them something and then we now have a relationship where they’ll ask me questions and we can work together.
So, number one, don’t be worried about offending your doctor. Number two, most doctors aren’t going to be offended. Number three, if they are, well, I don’t know what to say about that, but I don’t get offended. Back when I was at UNC, I had patients go to Duke and the Duke patients would come to me. Sometimes it’s just good to hear things twice. I think if your doctor is offended, that’s a red flag on their own ego. I think all that we should want as your doctors is for you to get the information you need. That is your job to advocate for yourself, and almost all doctors are going to be totally happy with it. We can learn something from each other as we share in your care journey going forward.
There is hope. Hope to live a normal life, and hope to see your kids and your grandkids grow up. There’s always hope on the horizon.
Dr. Catherine Coombs
Jeff: Thank you for that and I love the way you put it. Patients should not be concerned about asking questions. They shouldn’t be concerned about saying, why not? If they’re having trouble getting along with their doctor, like you said, that’s a red flag.
Navigating what symptoms you should share with your doctor
Michele: We have some more patient questions, so here’s one of them. Sara N. asks, “How do I know when I should contact my doctor between visits? Do they need to know about every infection or just about CLL symptoms?”
Dr. Catherine Coombs: Sara, that’s a great question. I think in the digital age, we certainly can let doctors know about every single detail, but I think it’s good to set up expectations. I try to do this on my first visit or maybe my second visit if we don’t have time to cover it.
But what things do I always want to know about, and then what goes into the other category? I always educate my patients on red-flag symptoms. Things that for my patients on watch and wait, watch and worry, active surveillance, things that make me think, we need to get you in right away. Unintentional weight loss, drenching night sweats, fevers. I go through the list of the things I always want to know about – a rapidly enlarging lymph node, etcetera.
Then there may be other symptoms, and the ones I want to know about are the ones that are worrying you. I don’t want you to go to bed freaking out about something that may be nothing. Just send me a message and I’ll tell you, that’s nothing or I need more information. Maybe let’s have you come in. I’d say, it’s never wrong if it’s something worrying you. But of course, we all have to acknowledge it could get to be a lot of messages if it’s every single thing. I think you just learn that over time as you establish with a doctor, but I think it’s good to go through what things should I let you know about right away, and what things can wait. Then obviously there’s some gray zone where it doesn’t hurt to just pass the info along and then you can get back a message and not worry about that.
Michele: In looking at a patient holistically, so to speak, regarding these little things that we may not think are important, such as all these various infections – I keep getting sinus infections. I’m trying to think of some other types of infections. Maybe you could list those for patients, some of the ones that they might be seeing that you want to know about.
Dr. Catherine Coombs: We do see an increase in infections in our patients with CLL. I do like to get a general sense of how often patients are getting infections. If they have a primary care doctor who’s very responsive, I’m okay with them treating these infections. I’m also okay taking the lead, whatever works best.
But when they become really frequent, especially if it ends up with the patient landing in the hospital, I absolutely do want to know about that. There are some strategies we have to lessen the incidence of these infections.
Patients with CLL, a proportion of them, don’t make enough immunoglobulins. If you’re landing in a situation where you’re having a lot of severe infections, meaning pneumonia that you’re in the hospital for, or terrible sinus infections, etc., that may be a reason to consider this intervention called immunoglobulin infusions.
I definitely like to know about things that I can fix. I’m okay knowing about things I can’t fix too. The ones where it’s like, this would change what we do, those are especially important. The patients may not know that before messaging me, and that’s okay. It’s okay to just message because you don’t know and then I’ll tell you there’s nothing to do or let’s bring you in and talk about X, Y, Z.
I always educate my patients on red-flag symptoms…Unintentional weight loss, drenching night sweats, fevers.
Dr. Catherine Coombs
Jeff: Fantastic. I’m going to make this a little bit personal as far as what I hope people are taking away from this discussion. When I was first diagnosed with CLL, my doctor told me straight up that I was going to die in about 6 years, and that doctor got fired. My next doctor told me, “Don’t worry, we’ve got this. You might die with this, but you’re not going to die from this.”
Listening to both of you fantastic doctors talk about the landscape of CLL and even use the 4 letter word “cure,” I am convinced that I am going to be able to continue doing everything that I want to do, and I want to do an awful lot of things at some point. If my daughters’ are cooperative, maybe I’ll become a grandfather, but I’m going to continue knocking out half-marathons. I’m going to continue knocking out full marathons. I’m going to drink good wine and good whiskey. I’m going to eat well. I’m going to laugh a lot. I’m going to smile a lot and I’m going to share my story so that patients and their caregivers know that that can be their life, too. Michele, how about you?
Michele: I agree some of my key takeaways are that there are so many things in research and we have the potential of being approved in the somewhat near future, which is yet another option for us. As you had explained, it does work in a different way than the traditional types of BTK inhibitors we now have. I think this is fabulous to have yet another option for patients.
Also, I love what you said about what you really need to look for in your own doctor and not be worried about offending your doctor. This is so vital for patients. I ask a million questions and I encourage patients to do so so that they can become more empowered for their own care and self-advocate for themselves.
It’s been so great hearing you and Dr. Levy both talk about patients asking questions and encouraging them so that patients are not afraid of this. This is again, one of the things I had started doing to try to get rid of the mystique around care and treatment with people’s doctors. I continue to do that.
In addition with Jeff – and we’ll be toasting soon, hopefully in person about this with something more than water, which we’ve been drinking during the program – and that is to live life to its fullest and to live a normal expected life span thanks to doctors like you, Dr. Coombs and Dr. Levy. I thank you so much for joining us, both of you and I thank all of our audience members watching us.
Dr. Catherine Coombs: And thank you both for all the work you do in patient advocacy. Like 10, 15 years ago when the Internet wasn’t available, I think there’s so much more fear. To be able to bring light in a way that patients can understand is so hugely important. So thanks for what you do as well and for having me.
Special thanks again to AbbVie and BeiGene for their support of our patient education program all about building shared treatment decision-making! The Patient Story retains full editorial control.
Natalia shares her myelofibrosis story, a rare form of blood cancer that leads to scarring in bone marrow, anemia, and fatigue.
In her story, she discusses her misdiagnosis and the long road she faced before being correctly diagnosed with myelofibrosis.
With a passion for painting, yoga, and Reiki healing, Natalia talks about how she coped with extreme fatigue and other symptoms. She explains why everyone should trust their gut and be a patient advocate, and what she’s doing to live life to the fullest.
I am a mom of two adults, Gabriel and Ingrid. I’m an artist, so I paint. I’ve been painting since I was in high school – oils, watercolors, acrylics. I am also an executive. I work for an aviation company. I’m the head of administrative operations there, so it’s a big job. The painting kind of releases stress.
Aside from that, I love getting together with my family because I love to cook. My grandfather was a chef and my mom was a really good cook. She had several restaurants, so I think I’m genetically predisposed to that within my family. I love music. I’m a historian – that was my major in university.
The business side is the survival side, but I think my creativity has helped me in my executive career a lot. I’m the type of person that, whenever there’s a problem, people come to me to brainstorm. That’s helped me a lot.
What were your initial symptoms and diagnosis?
At the end of 2021, in the fall, my mother had passed away in August and I was going through a divorce. I started feeling shortness of breath. I always thought, “Maybe I’m just really stressed out.” But at one point, it got so bad that I couldn’t sleep lying down. I would have to sleep sitting up.
I knew it wasn’t an asthma attack because it was different – the pressure felt different in my lungs.
That’s when I decided to call my cardiologist, Dr. Mechanic. I called her and I said, “I’m having this problem. Can I come in?”
She did some tests, and then she told me that I was diagnosed with something called pericarditis. That was the first indication that there was something wrong.
Did you ask any questions after receiving your diagnosis?
She gave me a treatment plan for 2 weeks. I was supposed to take 25 100-mg of aspirin – some crazy stuff like that. Before I left her office, I looked at her and said, “What could cause this?” Because you don’t just randomly have something like that. That question saved me.
I’m still here because she immediately looked at me and said, “Well it could be an autoimmune disease.” So I said, “Who would I go to for that?” And she said, “Well, you could try a rheumatologist.” And that’s exactly what I did.
What if I just walked away and said, “Okay. I have this and now I have to treat it.” I think you need to go further and say, “What could cause that?”
I knew it wasn’t an asthma attack because it was different – the pressure felt different in my lungs.
It’s just very random. I mean, if they tell you it’s something genetic or caused by a medicine you’re taking or something like that. But for her, there was no other indication of that happening to me. So that kind of saved me.
I immediately thought, “I am going to go.” I made the appointment and I saw the rheumatologist and she ran about 7 different blood tests on me.
The importance of asking your doctor questions
I respect doctors very much. They have so many patients and such little time. And that’s why I believe that you need to ask the questions – to have your list.
I never go to a doctor, since then, without a list of questions because it’s easy to forget. They’re rushing and you feel like you’re imposing or you [consider] the waiting room is full of people.
That one question, “I need more information” could save your life.
I never go to a doctor, since then, without a list of questions because it’s easy to forget.
Describe your visit to the ER
I had a very funny day because I had to go in to get my results from hematology. I was living in my daughter’s apartment at the time, on the third-floor walk-up. I walked out, got very dizzy, and fell down the stairs. I had to call her to help me untangle myself.
At tje doctor’s office, and the first question they asked was, “Have you fallen? Have you been falling? Have you fainted recently?” I told the doctor that I fell down the stairs and she told me to go to the ER. I responded with, “No, I have to go to work and I have meetings.”
She was looking at me weirdly and then she told me ”Your hematocrit was something like 59 and your hemoglobin is 17 so you must not be feeling well.” She said, “I’m not a hematologist so I can’t give you any more details or tell you anything, but you need to see a hematologist immediately.”
I think her words didn’t really make any sense to me because I’ve never had to deal with hemoglobin or anything like that. She was looking at me like I was a ghost, like I wasn’t supposed to be standing. Their expression immediately felt like a cold sensation from my heart to my stomach.
I said, “Okay, I’ll make an appointment immediately.”
The hematologist suspected everything was fine
I went to a wedding in Columbia. I was with both of my kids. It was a hectic schedule. I started feeling like I couldn’t breathe, I couldn’t go up the stairs. I was thinking, “This is probably the altitude, I’m in the mountains.” Came back, and started getting very, very ill and extremely tired.
That one question, “I need more information” could save your life.
I came back [from Columbia] and I went in for my appointment. They drew blood and then the doctor came in and says, “We’ll have the results by tomorrow but I believe what I’m looking at right now is a mistake.” She was looking at the labs from the rheumatologist and she said, “I think they made a mistake. By tomorrow we’ll have our lab results and it’s probably going to be very different. I don’t think there’s anything wrong with you.”
Cancer Diagnosis
Was this the same doctor you’d made an appointment to see?
I showed up on the 23rd to see a specific doctor, and they told me, “You’re going to see a different doctor.” I said, “Well, that was not what I wanted.” And they said, “Well, that’s what we have available.”
You’re here and you feel very trapped in the sense that I had already waited for a whole month to see the specific doctor. Then you have a situation where they told you it’s urgent. Are you going to walk away? No. You’re just going to go in and see whoever so you can get some answers. But I knew I was not with the person, that I felt, had the knowledge.
How did you find the doctor you wanted?
I go on the hospital page and look at hematology. [The doctor I chose] was basically just taking care of hematology disorders, blood disorders. I had seen [the doctor I was assigned] because she was part of that group, but her expertise was gynecological hematology and I thought it was something to do with breast cancer. So she had several things, but he was a specialist on blood disorders and that’s why I picked him.
Then you go to Healthgrades, of course. You see the patient comments to make sure that people are being treated well. For me, that was the person that had great reviews and knew about what I was there to find out about.
COVID delaying information on lab results
I wasn’t worried because she said, “It’s probably a mistake.” I completely trusted her views and went home. Then the next day, which was December 24th, she called and said, “You need to come in and you need to see me next week.” I said, “Well, I have a trip on Monday. I have my ticket.” And she’s said, “You can’t travel, you can’t get on a plane.” That’s when she explained to me, “Your hemoglobin is so high that if you get on a plane right now, you could have a stroke.”
I immediately had to cancel all of my plans. My kids were devastated. My family had an Airbnb. Everything abandoned. I went in to see her on December 28th – that was her first available appointment. I arrived and the minute that I got to the floor before I left the elevator, I was escorted out by the management because she had done a COVID test on me the week prior and it had come back positive.
My daughter and I were kicked out of the premises. I had no idea. I usually keep the little tests at home. I was testing because I knew I was going into a cancer place. I told her I tested this morning and they said, “No, we did the blood test. You’re positive.” I needed to wait 2 weeks with minimal information.
“Yes, you have something very serious, but you can’t come near the hospital because you have COVID.” It was probably the worst Christmas of my life because my mother had just passed, my kids went on another trip with their dad because the whole Columbia thing was scrapped, and I was sitting there just not knowing what it was and had to wait until January 12th to see the doctor again.
What did you do following your cancer diagnosis?
The doctor said she thought I had Polycythemia Vera and the way that we can immediately attack it is by doing phlebotomies. She wanted to start doing phlebotomies every 2 weeks.
That was the first day that I ran from her office to the infusion center and had attempted to have my first phlebotomy. That didn’t work out very well. I had to leave and come back the next day.
That was the “it” day because then you go home and you start looking this up and go into a bit of a panic.
When I realized what was happening to me emotionally, I called one of my best friends, Bernice. Her mom is a pediatrician. I spoke to her and I said, “Hey, I just heard this. I’m very scared.” She called her friend, who was a hematologist in Venezuela and called me back and gave me the lifeline of words.
She told me, “You’re going to be fine. It’s controllable. I have a friend that has this.” I stopped searching and just said, “Okay, I’m going with what she’s saying.”
You have to look for the most positive energy source, and that was mine.
You have to look for the most positive energy source, and that was mine.
Were there any additional tests you had to do?
Yeah, especially genetic tests. They look for certain genetic mutations. She couldn’t give me anything definitive until I completed that.
From there on, I start having phlebotomies. I think we started every week. Because there was so much going on, I started getting weak, and very dehydrated.
I’m scheduled for a biopsy on February 7th, so she starts checking. We’re doing scans of the brain looking for any sign of strokes. She checked my entire body. We did scans of everything – MRIs, etcetera – just to make sure I wasn’t having any blood clots because that’s what the condition causes.
Getting a Biopsy and Treatment
How did your body react to phlebotomies?
On February 7th, I do my biopsy. Biopsy results usually take 2 to 3 weeks to come back. By that time and during that time – January 31st, actually – I had already called in because I was so weak from the phlebotomies that my doctor gave me a letter so I could get some short-term leave.
From the end of January to the end of February, I’m already on medical leave, trying to control this. At one point I started telling her, “Look, I don’t think I can do these things because I go home for 2 or 3 days, I’m useless. Could you give me some fluids?”
I started figuring out that the pain I was feeling was probably from being dehydrated. She changed the way we were doing it and she would ask them to do the phlebotomy and then give me 2 hours of fluids afterward.
How did you feel after receiving your biopsy results?
Then the results come in. Of course, we have a very different conversation, her and I. She tells me, “This is going to be a lifelong situation where you’re going to be taking blood out. I need you to be at a certain level where you’re kind of anemic. We need to lower your hemoglobin to at least 11 or 12.” And I said, “Okay, let’s do it.”
To me, it was like I was already there. She wasn’t going to go look for anything else because I felt overwhelmed. That’s why you should do the research before because once you’re in there and you get that diagnosis, your mindset is very different. You’re just in crisis, in shock mode.
It was tough because with it came the knowledge that because you’re making so many red blood cells, your bone marrow is overactive. Your bone marrow starts getting tired and it starts getting fibrosis, which is like scar tissue.
She tells me at one point, we might get to a level where the opposite happens and you stop making the red blood cells and we go into something like leukemia. This is terrifying news.
At the same time, she said something kind of weird. She said, “Well, of all the cancers you could get, this is the best one.” [I] didn’t agree with that, because I don’t think there’s anything that you could say to someone that would sound good at that moment.
It was a knowledge that it was progressive, that there was absolutely no cure for this. I Googled, “Has anyone ever gone into remission?” and found one person in 1984. I kept it in one of my phone’s URLs. I kept it there until this year. I would look at it as if one person could get out of this, so can I.
What were some symptoms that arose with your treatments?
We start a process where they’re taking blood out. My veins are not easy to find, so that was another issue. I had one person that could find them [with] a special light.
You go home from the phlebotomies. I think it’s 500 cc’s that they take out every time you go. I had to drive myself because my entire family is working at this time. By the time I was getting home, my eyelids were getting heavy. I had to go up 3 floors and then and I could feel all my joints. It’s like a toothache in your bones.
Progressively, I started having pain in my hip, and then I couldn’t sleep at night because I started having night sweats. I had to purchase this little machine that is like a little air conditioner. Four times during the night I would have to put that on. I had the air conditioner going at home and had to put that on so I could come back to normal.
I started chewing ice. There’s a condition called pica that is caused by severe anemia, and then you get addicted to ice. I’d be chewing ice all day. Then at night, I would have to pee 7 times a night. My nights were horrible. I stopped exercising.
Quality of Life
What kept you going?
My life became very small. Then I had a conversation with my dad, and I told him, “I feel like I can’t do anything. I don’t have the strength to move around, to do the things that I normally do.” He said, “You have to move.” That voice stayed with me. Where I live, there was nowhere to walk around. He said, “Even if you go to the parking lot and you go 2, 3 times around the parking lot, you have to move.”
It’s true because it’s all about your circulation and the blood clot situation. You need to move and [my doctor] had told me that. But until I heard it from my dad, I was feeling like a victim.
I’m just taking in hits and I wasn’t coming out and doing anything about it. That gave me my first fighting punch. I was like, “Okay, let me move” and I started moving.
I would wake up every morning and I would do yoga in my room because I didn’t want to move around too much. I would do meditation, I would do yoga, then I would drive to this little park that I knew about. I would go around a few times. I would go to this organic store every day and buy the ingredients for the meal that I was going to have because that forced me to do something outside of the house.
I did TikTok videos about my recipes and kept looking for things to keep me going. I started reading a lot about spiritual healing meditation and called one of my really good friends, Marianne, and asked her, “Hey, do you know someone that does Reiki healing?” And she’s like, “I’m a Reiki healer. I went to the best school.” I had no idea!
She goes, “Start coming.” I would go and see her once a week and that just changed the entire process for me.
No signs of improvement with treatment
I started feeling that we were just taking blood out over and over. I thought at one point I was going to feel better and kept asking her, “I have to go back to work. Am I going to feel better?” And she kept saying, “You need to adjust your lifestyle to the condition.” And I said, “But there has to be something.”
She suggested hydroxyurea and she said that my insurance had approved it if I wanted to go on it. I said, “No, I don’t. I don’t want to take that. I don’t feel that’s going to add to anything. I’ve studied it, I’ve seen the side effects and I don’t think that I’m at the level where I would be able to handle that. I want to feel better before I go to the next step like that.”
She was struggling with me. I could tell that she kept looking at my results and scratching her head, “What’s going on?” Because one day it was the platelets and then it was the white blood cells. And then she was getting a handle on it.
I went to do my phlebotomy on May 10 and the nurse told me, “You are a hemoglobin level of 8.” Anyone who was a nurse or a doctor knows you can’t take more blood from that person. I know that now, I didn’t know that then. She asked me, “Do you think we should take the blood out?” I looked at her and said, “I’m not a doctor. You need to talk to my doctor.” At that point, I didn’t know if she was dealing with platelets or red blood cells. She said, “Okay, we’ll talk to your doctor.”
I came back on May 19th for another phlebotomy. The answer, when asked “Did you talk to the doctor?” was “It’s still in the treatment plan.” They took blood out that day and then they took out blood again on June 7th. That’s 2 times after my hemoglobin level 8.
I came back on the 9th because the gentleman that was doing my phlebotomy that day refused to do the IV on me. He said, “I don’t have the right package, I’m not going to do it.” He took my blood out in 11 minutes. It would normally take 30 minutes. He just destroyed me after that, I was so sick.
My daughter started calling the doctor at night. She told me she was going to call 911. I’m like, no, because I was afraid of going to a hospital. This is a very rare disease and I knew no one would know what to do with me. So on the 9th, I came back. They gave me the fluids.
Describe working while still battling cancer
By that time, I’m still going to work. I would get to the office. I would call my security guard. Jason would come down and I told him the first day, I said, “I’m so sorry because I know this is not your job scope or anything, but I need a human favor. I can’t carry my laptop anymore.” So he would wait for me.
I would give him the laptop bag and all the stuff that we carry for work. I would go park, then I would walk and he would wait for me. He was a gentle giant. He would wait for me and walk me to my office. Then it would take me about 15 minutes to recover from walking up.
I would have this huge thing of ice that I had to eat. The ice had some sort of chemical reaction in the brain that gives you a little bit of oxygen, so it would make me feel better.
I couldn’t have rice and potatoes for lunch. I would have a carrot and a cucumber because if I had a normal lunch, I would fall asleep on my desk. That’s when I realized, this can’t be it. Like, how is this happening?
Incorrect Treatment Advice
The doctor had made an error
I went to my sister’s house on the weekend of Father’s Day. Saturday, I couldn’t talk. I sat there and I couldn’t talk. I couldn’t move around.
The next morning, which was Father’s Day, I drove myself to the ER and they told me, “Your hemoglobin is at 6. We need to do a blood transfusion immediately.” And I said no, because my doctor had already told me, you can’t get a blood transfusion because the red blood cells are going to just explode. So I refused it.
Then I waited maybe 2 more days to see her because she was coming back from vacation.
When she finally saw my labs, she said to me, “I am so sorry. I miscalculated your numbers and you will need a blood transfusion now.” I was furious.
I would fall asleep on my desk. That’s when I realized, this can’t be it. Like, how is this happening?
She said, “Once you get the blood transfusion, you’re going to start making blood like crazy and we’re going to be back to the level that you were in January.” Imagine going through this every 2 weeks – phlebotomies and all the pain. How am I going to go back to that? That didn’t make sense to me.
She said, “We need to go right now. We need to put you in the ER.” I said, “No, I need some time. This is a serious situation. A blood transfusion is something very serious. I need to talk to my family. I need to go home and I need to think about this.”
What was your doctor’s reaction to your refusing a transfusion?
She was not very happy with me saying no because I think she realized the responsibility of me just going home the way that I was. But I went home and I called Bernice’s mom again. She called her friend, the hematologist and we waited until the next day because he’s in Venezuela. And he said, “She’s wrong. You’re not going to start making red blood cells like crazy. Your hemoglobin with the blood transfusion is only going to go up 2 points and that’s it. [For] the rest, you would need iron.” That’s another story.
So that’s when I called her back, on a Thursday. I spoke to her and I said, “I’m going to go through with the blood transfusion.” She said, “I’m going to have my office call you and schedule it immediately.” They never call me back, to this day, not even to find out if I’m still alive.
Did you still get a blood transfusion?
I waited until Saturday because my friend Lizzie works at the hospital. She told me, “You need to go into the hospital on a Saturday around 7 to 9 a.m. There won’t be anyone if you’re going through the emergency room.”
I started researching who had the best hematology group for my condition. I found South Miami Hospital. I found Dr. Kim, who was in charge of blood disorders. I went to her hospital but went through the emergency and then I was assigned to her.
From there, I got my blood transfusion. I think it was June 24th. My hemoglobin went from 6 to 8 within a few days. Then I was with the new hospital, a new doctor, and went from there.
How did your first doctor explain their miscalculation?
I said, “Well, how do you mean? Your team has been telling me that [my hemoglobin was level] 8 and I shouldn’t be taking blood out. Did they reach out to you?” And she said, “Yeah, but I thought that because you have Polycythemia Vera, you would make so much more blood, so I wasn’t concerned with that. I figured we were following the right pace, so you were making blood at the same speed that was taking out. I don’t think it should have been a problem.” That was the explanation I got.
Switching Hospitals and Doctors
Beginning treatments for anemia
I was with Dr. Kim from June until last month. In February, she started giving me iron pills because now we’re trying to get me out of very aggressive anemia where I have zero iron deposits.
She starts giving me the pills, she tells me there’s no more phlebotomies for a long time, you can now fly because you have blood! [She] started treating it in a very positive way, but I was still very weak. Without the phlebotomies, I start feeling a little bit stronger. I go back to work. I realized that I couldn’t do a lot of physical activity, but I tried to walk a little, maybe like 20 minutes a day just to help me out.
Everything was going fine but we kept doing labs and my hemoglobin numbers were not moving and my iron. I think all of last year, we were able to get it up to 9. That’s it. We’ll be stuck at 9 or even a little lower or go up to 9.5, but never more than 10. It was like 9-point-something always.
When I left on vacation in December, she told me “When you return, we might have to give you iron infusions because I’m not getting anywhere with the pills.”
Developing a papilledema
I come back from vacation, I start working. January 21st, I’m sitting here with my family having dinner, and I start seeing something very strange in my eye. The next morning, I wake up and I see I have a floater, a dark spot. I got very tired. My limbs felt tired. I stayed in bed all Sunday. Monday I call my ophthalmologist. They gave me an appointment for that morning.
At the time, one of my cousins sent a video in our chat about what it feels like to have a stroke, and in the video, there’s a picture of a person seeing what I was seeing. I panicked.
Dr. Kim and her team would answer phone, email, everything within 2 minutes. I tell her what’s going on. She said, “Don’t go to the ophthalmologist, go to the ER.” I went to the ER and she was already there, she came in immediately. I had MRIs done on my brain. I had something called papilledema, which is an edema of the brain, which affected the eye.
Getting a second biopsy and diagnosis
What happened (it’s probably because of all the anemia) they checked my numbers and my platelets were very high. They were 740. That’s when she realized, “This isn’t right. Her numbers are not responding and I need to do something.”
She told me “I’m going to have to do another biopsy,” which I was terrified of. She goes, “It just doesn’t make sense to me. I’ve been giving you iron for months and nothing changes, and now I see your platelets are up. This doesn’t make sense.”
February 7th, I go through another biopsy and she calls me 2 weeks later and says, “You have primary myelofibrosis, not Polycythemia Vera. It makes sense because in myelofibrosis sometimes you’re making a lot of red blood cells, and sometimes you’re making zero. Sometimes the problem is the platelets or the white blood cells.”
I had MRIs done on my brain. I had something called papilledema, which is an edema of the brain, which affected the eye.
Not having access to medical records from the previous doctor
Whatever she was reading, because she had the other doctor’s diagnosis and notes, was not what is happening.
The only thing that she’s able to see from my former hospital is what I have in my chart. She’s never able to get my official medical records, even though I sent 2 letters to the hospital and I called the hospital and spoke to, I don’t know how many people. So they never got my records.
They don’t answer anything. [I] kept sending the letters, because at one point, I called and they said, “Send a letter.” I did that during the fall of last year, but nothing happened.
[My doctor] said, “I don’t have anything to compare, but the notes that are on there. I need to see the actual pathology exam that was done.” She was under the assumption that whatever [my previous] doctor had put on her notes was what was happening.
How did you react to being diagnosed with myelofibrosis?
That was a very difficult week, a very dark week. I was so happy to know that there was a path. Now things made sense to me.
I was told immediately that I wasn’t going to stay with Dr. Kim anymore because she’s a benign hematologist. I needed to go to another hospital and go to malignancies. That was difficult because I was already very attached to Maria and Dr. Kim because they were awesome.
I was traumatized. I thought, “I don’t want another doctor. I’m good here.” You met someone you could trust, now I have to find someone.
But they were so sweet. They said, “We’re going to be with you until everything’s done.” The first thing they did is an iron infusion immediately, so I got an iron infusion. They gave me the options that are available in this situation.
They have an amazing new medicine. I believe it’s Jakafi. They also said, “Miami has an excellent cancer center in Baptiste’s, a brand-new building and it is just truly amazing what they’re doing there.” They told me “You have the option of getting a bone marrow transplant. They have a team there that does it.” That’s also another point that you feel great. “We’re going to refer you to this new doctor at this location.”
Changes in Lifestyle and Outlook
Finding hope by reading about patient’s experiences with myelofibrosis
Of course, the next morning, and the next 3 days are terrible because I, again, am looking at everything possible about myelofibrosis. It is terrifying until I found [The Patient Story].
I found Mary’s story. I had spent 3 days where I couldn’t move. I would cry 7 times a day. I live by myself, so it’s not a good environment for someone that’s going through this because I’m not hungry because of the anemia. I wasn’t sleeping well. I was just in a very dark place.
I see her story and the first thing she says about fatigue (I was feeling really tired), if you’re fatigued, you need to move. Don’t go take a nap – move.
I see her story and the first thing she says about fatigue (I was feeling really tired), if you’re fatigued, you need to move. Don’t go take a nap – move.
I immediately started thinking, “Yes, I’ve been at home for months with all the stuff that was going in my brain and taking this medicine that they had put me on, then they gave me this very difficult news.” I’m just going into that little world from last year. I immediately thought, “I need to call someone.” I knew that one person that would have the time to wake me up every morning and get me out of the house.
Getting back into an exercise routine
I called a [family friend] and said, “Hey, can you be here every day next week at 9 a.m. and get me out of the house?” I love biking outdoors. Walking is very difficult because it’s hot here in Miami. The heat is not good. But when you’re biking, you’re getting air and it’s just easier for me. He agreed, and for an entire week last week, he would come in and we would walk.
I mean, [at] first, we walked, but it didn’t work out. So I’m like, “No, biking” and we would bike [for] 12 minutes. I would have to sit down and catch my breath for the return. And then he would help me prep food. We went [with the] Mediterranean diet because the new hospital sent me a Zoom meeting where they told us food is medicine. That week, I was able to bike 4 times.
What’s your outlook on living with myelofibrosis?
You’re here to get your children through difficult situations. You’re not here just to live and breathe. You’re here to affect other people.
I decided my spiritual beliefs are, you have to fight for every inch of life that you can get. Even if it is less than normal and if it is painful sometimes.
Most of the time you are here to inspire, you are here to love. You’re here to get your children through difficult situations. You’re not here just to live and breathe. You’re here to affect other people. All of us affect each other. I mean, [The Patient Story] affected my life in such a positive way. This is what we do. So I said, “Whatever it is I need to do, I’m going to do it.” I stopped reading all the horrible stories that you find on Google.
[I] got my appointment with the specialist. I saw her on Monday. This week, I’m going to see the transplant specialist on the 8th. [I] got amazing news because they have a resident in that hospital that was able to obliterate or get rid of the graft versus host disease, which is one of the biggest problems after a transplant. I have my sister and my 2 kids as possible donors. I’ve had a crazy amount of people being brave enough to even say “I will do it.” I was like, “Wow, that’s amazing.”
Did biking improve your quality of life?
[Biking] makes a complete difference because your circulation is hindered by how thick your blood is with this condition. Once you start moving, you realize when you come back from it, you have 3 or 4 hours of high energy which you don’t have if you sit around. You don’t get the tingling in your hands or your feet.
Psychologically, you’re out, you’re getting some fresh sunlight. I think the worst thing you can do is lie down and close your shades because you just really need that vitamin D.
We human beings need everything around us that’s been created for us. Water, sunlight, other people. That’s the best medicine.
The biggest thing that helps is exercise because it helps with joint pain.
What are some other things that improved your quality of life?
Once I got the infusions, I stopped eating ice. I’m excited. That helps me sleep through the night a lot better.
If you’re having hot flashes, which you will have with these conditions, they sell these covers for your mattress that are cold and a pillow. The items that I bought helped me so much. You just put it on here. They sell them on Amazon for maybe 20 bucks. If you wake up in the middle of the night, you turn it on and you’re able to cool down enough to go to sleep.
In case you’re in a situation like I was where the anemia was so terrible and you need to work, having that lunch that I would have, carrots and cucumbers, would get me through the day so that I could come home, have a regular meal and be able to digest it and get sleepy on my couch, not at work.
I think the ice did help a lot during that time because it helped me breathe better.
Reflections
Have you spoken to your first doctor again?
No, I’m writing her a letter. A lot of people have told me, “Why don’t you do something about it?” I don’t want to do anything with litigation or anything like that, because I need positive energy in my life right now.
Trusting your gut
I believe you have to look at how things make you feel. It is difficult to say to a doctor, “You don’t make me feel right.” It’s not a fact, it’s just feelings. But feelings are very important, especially when you’re going through this.
When people are paying attention to you, pay attention. If they’re making eye contact, pay attention. If they’re looking at their watch and they’re in a hurry, you can fire your doctors. I learned this and it is the best thing to learn.
If you go to someone and they make you feel inaccurate, they discard your symptoms as not important…
I had gone to a cardiologist, different from Dr. Mechanic that year, and he had told me there was nothing wrong with me. When people are paying attention to you, pay attention. If they’re making eye contact, pay attention. If they’re looking at their watch and they’re in a hurry, you can fire your doctors. I learned this and it is the best thing to learn.
When she told me, for example, about the drug, I felt in my heart that I would rather go through the symptoms that I was having than take that medicine. I went and I studied it and I went into the blogs and I saw what people were going through and I said, “No, I don’t want this.” I, told her, “If you see that I’m close to dying, then I have to take it. I will. But at this point, do you feel that I’m at that stage?” She said, “Well, it would be great.”
Remember, they’re advocating for medicine. I’m not saying that’s [always] the case, but sometimes they are because they’re selling something they’re trying out too. Sometimes we’re guinea pigs. They’re trying stuff on you.
If it makes you feel weird, it doesn’t feel right, walk away. Say no, respectfully. I told her, “I’m sorry. I know you got it approved, but I’m not interested in that right now. I need time to process this, and I don’t feel like I want those side effects.” I think it’s kind of like chemotherapy medicine, so it’s a serious medicine that you can’t just be offering to people. Do your homework, read.
Also, if you are told to take something and it has to be that way, don’t believe the worst-case scenarios. We’re all different, we all react to things differently. Just focus on how you feel.
How does that energy of that person make you feel, in the case of a doctor, when they offer you things? She told me, “Let’s go for the blood transfusion right now.” I said, “No, I need time” and give yourself that time because there will come a time when you say, “I’m ready.”
Whatever it is, don’t let anyone rush you into anything. It’s your body, it’s your life.
I would have been on that medicine for a year and I would have been on the wrong medicine because right now they’re like, “No, we’re not going to give you that.” So imagine.
We’re all made of energy, so it’s the most important thing [to] be around people who present that energy. There are people that are going to come and look at you and you’re going to tell them what you’re going through. But because you look fine and you have hair, you don’t look like you’re very ill, they’re going to just tell you, “So and so has this disease and they’re fine.” Do not listen to that. You are a unique human being and only you know how you feel.
Communicating your needs to people
The other thing is work. We’re indispensable and we have to be there. That was my first struggle – I need to go back to work. I need to go back to work even though we have remote work. That’s helped me so much – my company gives us 2 days of remote work a week.
I’ve been able to keep my job because of that opportunity. Talk to the people around you, talk to your boss, talk to your assistants, talk to your co-workers. You don’t have to give them details, you just need to let them know.
I told my boss, “Hey, there’s certain things that I’m not very good at right now” like events. I was the life of the party. Now I’m not. [I’m] kind of sitting in a corner, but I told him that. He’s an amazing boss. He’s just so understanding. He’s like, “Okay,” because he didn’t know that. So you let them know.
Also, you can’t expect people to assume and know. You need to let people know if you’re not feeling well, because people are worried about their life.
Many times, I would not tell my boss or people in my family how I was feeling and I kept treading on. Then you get to a point where you get upset, and it’s not their fault. They’re fine, they’re not in your shoes. You’re the one that needs to communicate, “Hey, today I’m not going to be able to go to that party because I can’t stay up after 9 p.m.”
My lifestyle has changed completely. You can’t drink alcohol. I can’t do certain activities in the sun, for example, I can’t take sunlight. I changed a little bit of my lifestyle, but I let people know. I let them know I’m a little different now. I’m still me, but we’re going to have to do things a little different.
What’s your top advice to others?
I got so much support after I started speaking up. If you stay silent, it’s not going to help you. At the beginning, I was like, I’m not going to bother. Then you’re the one that is going home hurt and sad, and they’re not to blame. They don’t know what you’re feeling. So speak up. Let people know. Find a buddy if you need to. My husband’s my buddy. I call him, “Carlos, I know you’re a health nut, so you need to help me now.”
In this case, for example, you ask for help and sometimes you’re going to get help that is not what you thought you needed or the person. Take what they’re giving you. My friend gave me this mug, it says “Mindset Is Everything.” I read a book called “The Biology Of Belief.”
They focus on the placebo effect and the fact that 30% of people just heal without taking medicine. Focus on that. I mean, how amazing is it that just by believing that you’re taking something your own body will heal?
Special thanks again to AbbVie for its support of our independent patient education content. The Patient Story retains full editorial control.